
Abstract
In this prospective, non-comparative case series, four patients with severe and highly active adult-onset Still’s disease (AOSD), refractory to high doses of corticosteroids (which had been combined with methotrexate in three of them) and methotrexate were treated with infliximab (initial dose 3–5 mg/kg, continuing at intervals depending on the patient’s individual disease activity). Resolution of their symptoms, which was evident within few days after the first infusion, and a parallel rapid improvement of the acute inflammatory response indices were observed in all. Concomitant corticosteroid treatment was reduced after the first courses of treatment with infliximab, which was well tolerated, and complete disease remission was sustained during a 5–18-month follow-up period. Although further studies to confirm long-term efficacy and safety in larger numbers of patients are needed, we suggest that administration of infliximab with observation for objective improvement is the treatment of choice in cases of AOSD refractory to conventional treatment.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Adult-onset Still’s disease (AOSD) is a chronic, systemic inflammatory disorder characterized by a sudden onset of high, spiking fever that often follows pharyngitis, a transient salmon-like rash, and the presence of arthritis or arthralgia. Lymphadenopathy, liver and/or spleen enlargement, and pericarditis, pleuritis or polyserositis may also occur. Laboratory abnormalities of AOSD include marked leukocytosis with neutrophilia, high C-reactive protein (CRP) levels and erythrocyte sedimentation rate (ESR), abnormal liver function tests and lactic dehydrogenase (LDH) levels, and a characteristically pronounced increase in serum ferritin levels [1, 2]. AOSD has a chronic relapsing course, but a significant number of patients experience complete remission between relapses [2]. Current treatment of the acute disease in patients who fail to respond to non-steroidal anti-inflammatory drugs (NSAID) consists of high doses of systemic corticosteroids. Second-line agents, such as gold salts, or methotrexate (MTX) have been used for chronic disease, and even cyclophosphamide has been used in resistant cases [2, 3]. However, treatment is not always successful and many patients with AOSD prove refractory to conventional therapy or demand an unacceptably high corticosteroid dose [2, 3, 4]. Moreover, fatal cases of refractory AOSD, in the setting of disseminated intravascular coagulation, adult respiratory distress syndrome and hemophagocytic syndrome, have been reported [4, 5].
Overproduction or inappropriate production of tumor necrosis factor-α (TNF-α) plays a major role in the pathogenesis of chronic inflammatory diseases, such as rheumatoid arthritis [6], idiopathic juvenile arthritis [7], ankylosing spondylitis [8], inflammatory bowel disease [9] and Adamantiades–Behcet’s disease [10]. Infliximab, a chimeric murine–human monoclonal antibody that neutralizes TNF-α-mediated actions, has been used with considerable success in the treatment of these conditions [10, 11, 12, 13, 14, 15]. In view of the fact that recent data suggest that TNF may be also involved in the pathogenesis of AOSD [16, 17], we decided to treat with infliximab four patients with severe and highly active AOSD which was refractory to conventional therapy.
Patients
In this prospective, non-comparative case series, four men aged respectively 19, 20, 35 and 72 years, in whom the diagnosis of AOSD was established according to criteria developed by Yamaguchi et al. [18], are presented. Two patients had long-standing disease and experienced a severe relapse while on immunosuppressive treatment. A third patient presented an acute relapse following prolonged remission of his disease, and was initially treated with the conventional approach. The remaining patient had no previous history of AOSD and was also treated with NSAIDs upon diagnosis, followed by high doses of corticosteroids and methotrexate. Clinical and laboratory findings that were present before infliximab administration, as well as previous treatments, are summarized in Tables 1 and 2, respectively. All patients were rheumatoid factor and antinuclear antibody negative, and all were prescreened for latent TBC infection with PPD tests (all negative), clinical examination and chest radiographs [19].
Intravenous infusions of infliximab (Remicade, Schering-Plough) were given at a dose of 3–5 mg/kg on week 0, depending on each patient’s individual disease activity, continuing at 3–5 mg/kg with intervals of 4–12 weeks, as described in detail below. Clinical response was arbitrarily defined as remission of all symptoms (i.e. fever, arthritis, arthralgias, rash), and complete disease remission was defined as normalization of laboratory values, including hemoglobin, liver enzymes, and the indices of the acute inflammatory response that were abnormal before the initiation of infliximab therapy.
Results
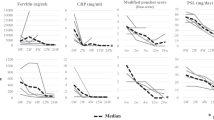
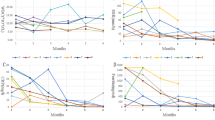
A rapid onset of clinical response was observed in all four patients within the first week after infusion of infliximab, and an impressive amelioration of laboratory values was evident within weeks. A complete remission of AOSD—i.e. all acute inflammatory response indices returned to normal levels—was also observed in all (Table 2). One patient discontinued infliximab after four infusions and remained free of disease during an 8-month follow-up period. The three remaining patients continue on infliximab, and up to December 2002 their complete remissions have been sustained for 18, 13 and 5 months, respectively (Table 2). Infliximab treatment was well tolerated. Brief case histories of the four patients are presented below.
Patient 1
A 20-year-old student, in whom the diagnosis of AOSD was made in March 2000, had been treated for over a year with prednisolone (10–50 mg) and methotrexate (20 mg/week). Any attempt to reduce the daily dose of prednisolone below 10 mg resulted in low-grade fever and malaise. In April 2001 he experienced a severe relapse and was admitted to Laikon Hospital. An increase of methylprednisolone to 1 mg/kg for a week, as well as a 4-day pulse (1 g/day IV) which followed, failed to control his disease. While steroid-induced hyperglycemia was being developed, he was given infliximab (3 mg/kg). To our surprise, resolution of all symptoms was observed within 1 week (Table 1). He was discharged on oral corticosteroids at progressively diminishing doses and concomitant methotrexate and NSAID treatment. On week 4, while his disease was in complete remission, a second course of infliximab (3 mg/kg) was given, continuing with infusions at intervals of 8–10 weeks. Noticeably, an attempt to increase the intervals between infusions to 12 weeks resulted in a mild disease flare, which was controlled within 24 h after the administration of infliximab. His disease remains in complete remission while on weekly methotrexate (15 mg) in addition to infliximab (Table 2). His steroid-related hyperglycemia has also resolved.
Patient 2
A 19-year-old male student was admitted to the hospital in September 2001 with a high fever, sore throat, arthralgias, pleuritis, and a salmon-like evanescent rash. After an extensive work-up that was unremarkable for other diseases the diagnosis of AOSD was established (Table 1). Initial treatment with NSAIDs and prednisolone (30 mg/day) was ineffective; finally, a daily dose of 80 mg of prednisolone was necessary to control his symptoms. Tapering of prednisolone dose to 30 mg/day caused an exacerbation of the disease and methotrexate 10 mg/week was added, which 1 month later was increased to 15 mg/week. During the next 3 months two consecutive attempts to decrease the prednisolone dose below 15 mg/day caused a high fever relapse; after the third relapse he was started on infliximab infusions of 3 mg/kg, in addition to weekly methotrexate and 20 mg of prednisolone daily. Within the first week a striking resolution of all symptoms, and near-normal levels of ESR and CRP, were observed. He received infliximab on weeks 2 and 6, continuing at 8-week intervals thereafter. Noticeably, he experienced a mild disease flare 3 days before the third infusion, but he has remained in complete remission ever since (Table 2). His current therapy also includes methotrexate 10 mg/week, and methylprednisolone 2 mg/day.
Patient 3
This patient was a 72-year-old farmer with a history of two episodes of high fever, oligoarthritis, severe anemia and mild liver involvement 14 and 10 years before his admission. At that time a tentative diagnosis of AOSD had been made and, in both instances, he had been successfully treated with NSAIDs and corticosteroids for 6 months. In September 2001 he presented with a high fever and accompanying chills, sore throat, marked asthenia, hip, wrist and shoulder arthralgias, a salmon-colored rash on the trunk and upper extremities, and pleuritis. He was first treated with broad-spectrum antibiotics for a suspected pulmonary infection and referred to our hospital. In addition to fever, rash and joint involvement he had a modest spleen and liver enlargement and left axillary lymphadenopathy (Table 1). Treatment with oral naproxen and intravenous prednisolone (1 mg/kg), followed by a 4-day methylprednisolone pulse (1 g/day) not only failed to control disease but resulted in a compromise of his renal function, as well as in steroid-induced hyperglycemia and myopathy. For these reasons, methotrexate was not added and naproxen was discontinued. He was then given a first infusion of 3 mg/kg of infliximab, followed by a second infusion after 2 weeks. He exhibited a fall in his fever after the first infusion and remained completely afebrile after the second. There was also a marked amelioration of the abnormal laboratory values with which he presented on diagnosis, and the tapering of corticosteroids resulted in normoglycemia and an improvement in the myopathy. The patient was discharged on oral prednisolone, 12.5 mg/day only. He received infliximab (3 mg/kg) on weeks 6, 10 and 18, as well as a 4-month course of oral rifampin, according to international guidelines [19], because of a suspicious history of previous exposure (pachypleuritis on chest CT scan). A complete remission of his disease was prominent 6 weeks after initiation of infliximab, including normalization of strikingly high ferritin levels. This remission has been sustained during an additional 8-month follow-up period after discontinuation of both infliximab and corticosteroids (Table 2). No evidence of latent TBC was noted.
Patient 4
A 35-year-old policeman was first diagnosed with AOSD in 1998. He initially received high doses of NSAIDs and methylprednisolone, to which gold salts were later added. His disease was only partially controlled and exhibited several relapses necessitating increases of the methylprednisolone dose. As a result of prolonged and high-dose corticosteroid treatment the patient became cushingoid, with a ‘moon face’ appearance. During the last trimester before admission his disease was poorly controlled, despite a further increase of methylprednisolone and gold salts doses to 40 mg/day and 50 mg/week IM, respectively. His fever rose to daily peaks of 40.5°, accompanied by chills and severe weakness and malaise. He was admitted to the hospital and treated with a further increase in the dosage of methylprednisolone up to 64 mg/day, and nimesulide 100 mg bid. A week later gold salts were discontinued and methotrexate was added. Febrile episodes were reduced to 1–2 per week, but his laboratory abnormalities remained unchanged and methotrexate was thus increased to 15 mg/week. Two months later a clinical improvement was evident, but the patient’s laboratory values remained severely abnormal (Table 1). At this time we decided to treat him with infliximab, which he received at a dose of 5 mg/kg on weeks 0, 2, 6 and 14. By the time of the last infusion he was in an excellent clinical condition for the first time in 4 years. A complete remission of AOSD, including normalization of very high ferritin levels, was observed while he was taking concomitant methotrexate (15 mg/week) and methylprednisolone (8 mg/day).
Discussion
High levels of proinflammatory cytokines, including TNF-α, have been found in the serum of patients with AOSD [16, 17]. It was thus reasonable to predict that a selective anti-TNF agent such as infliximab might be effective in the treatment of this chronic inflammatory condition. Therefore, we decided to use infliximab in our patients with severe and highly active AOSD who were refractory to conventional therapy. The schedule of administration was almost the same as that suggested for patients with rheumatoid arthritis, i.e. infusion of 3 mg/kg on weeks 0, 2 and 6, and every 8 weeks thereafter, in the first three patients [15]. However, because patient 3 had experienced a complete remission lasting 10 years before his relapse, we decided to discontinue infliximab after the fifth infusion. Indeed, he has remained free of active disease ever since. The remaining patient had the most refractory disease and he received higher doses of infliximab (5 mg/kg), as given in patients with Crohn’s disease [21].
All four patients exhibited a rapid remission of their systemic disease soon after the first infliximab infusion. This allowed corticosteroid tapering, thus freeing them of the related adverse effects, i.e. hyperglycemia, myopathy, and Cushing-like appearance. Interestingly, two of the four patients had failed to respond even to pulse methylprednisolone therapy. Because of the individualized nature of this disease, the slight differences that were observed between our patients in terms of the overall disease course, time for complete disease remission, and optimal schedule of infliximab administration, are to be expected. However, once complete remission was achieved, it was sustained in all during a 5–18-month follow-up period. Moreover, infliximab treatment was not related to any side effects in these patients.
Our report is added to the successful use of infliximab for refractory AOSD in small cohorts and cases of patients reported by Cavagna et al. [22], Kraetsch et al. [23], Huffstutter et al. [24], and Caramaschi et al. [25]. Collectively, in a total of 16 patients treated with infliximab all clinical features of the disease were completely suppressed. In contrast, in an open study of 12 patients with AOSD who received the TNF soluble p75 receptor etanercept for 6 months, two withdrew because of a disease flare, and of the seven patients who were considered responders only two met the ACR 70% response criteria. Moreover, among the three patients with fever and rash, these symptoms improved during etanercept treatment in only one [26]. A possibility that the efficacy of infliximab is superior to that of etanercept in AOSD may therefore exist, although this matter has not been addressed. It has recently been established that differences in the mode of action between these two anti-TNF agents account for their differential efficacy in inhibiting the inflammation in Crohn’s disease [27].
In conclusion, successful treatment of AOSD in our patients, taken together with other reports, suggests that administration of infliximab with observation for objective improvement is the treatment of choice in cases of AOSD refractory to conventional treatment. Given the restricted treatment options in AOSD and the potential of infliximab to successfully treat this disorder without the side effects resulting from prolonged use of corticosteroids and other non-selective immunosuppressants, a formal controlled trial to confirm its long-term efficacy and safety is justified.
Abbreviations
- AOSD:
-
Adult-onset Still’s disease
- CRP:
-
C-reactive protein
- ESR:
-
Erythrocyte sedimentation rate
- LDH:
-
Lactic dehydrogenase
- MTX:
-
Methotrexate
- NSAID:
-
Non-steroidal anti-inflammatory drugs
References
Fautrel B, Le Moel G, Saint-Marcoux B et al. (2001) Diagnostic value of ferritin and glycosylated ferritin in adult onset Still’s disease. J Rheumatol 28:322–329
Wouters JM, van de Putte LB (1986) Adult-onset Still’s disease; clinical and laboratory features, treatment and progress of 45 cases. Q J Med 61:1055–1065
Sato M, Takeda A, Honzu H, Saku N, Minato N, Kano S (1993) Adult Still’s disease with Sjogren’s syndrome successfully treated with intravenous pulse methylprednisolone and oral cyclophosphamide. Intern Med 32:730–732
Iglesias J, Sathiraju S, Marik PE (1999) Severe systemic inflammatory response syndrome with shock and ARDS resulting from Still’s disease: clinical response with high-dose pulse methylprednisolone therapy. Chest 115:1738–1740
Kumakura S, Ishikura H, Munemasa S, Adachi T, Murakawa Y, Kobayashi S (1997) Adult onset Still’s disease associated hemophagocytosis. J Rheumatol 24:1645–1648
Beckham JC, Caldwell DS, Peterson BL et al. (1992) Disease severity in rheumatoid arthritis: relationship of plasma tumor necrosis factor-alpha, soluble interleukin 2-receptor, soluble CD4/CD8 ratio, neopterin, and fibrin D-dimer to traditional severity and functional measures. J Clin Immunol 12:353–361
Mangge H, Kenzian H, Gallistl S et al. (1995) Serum cytokines in juvenile rheumatoid arthritis. Correlation with conventional inflammation parameters and clinical subtypes. Arthritis Rheum 38:211–220
Lange U, Teichmann J, Stracke H (2000) Correlation between plasma TNF-alpha, IGF-1, biochemical markers of bone metabolism, markers of inflammation/disease activity, and clinical manifestations in ankylosing spondylitis. Eur J Med Res 5:507–511
Van Deventer SJH (1997) Tumour necrosis factor and Crohn’s disease. Gut 40:443–448
Sfikakis PP (2002) Behcet’s disease: a new target for anti-tumour necrosis factor treatment. Ann Rheum Dis 61 [Suppl 2]:ii51–53
Kavanaugh A, St Clair EW, McCune WJ, Braakman T, Lipsky P (2000) Chimeric anti-tumor necrosis factor-alpha monoclonal antibody treatment of patients with rheumatoid arthritis receiving methotrexate therapy. J Rheumatol 27:841–850
Lovell DJ, Giannini EH, Reiff A et al. (2000) Etanercept in children with polyarticular juvenile rheumatoid arthritis. Pediatric Rheumatology Collaborative Study Group. N Engl J Med 342:763–769
Breban M, Vignon E, Claudepierre P et al. (2002) Efficacy of infliximab in refractory ankylosing spondylitis: results of a six-month open-label study. Rheumatology (Oxford) 41:1280–1285
Bell S, Kamm MA (2000) Antibodies to tumor necrosis factor alpha as treatment for Crohn’s disease. Lancet 355:858–860
Furst DE, Breedveld FC, Kalden JR et al. (2002) Updated consensus statement on biological agents for the treatment of rheumatoid arthritis and other rheumatic diseases (May 2002). Ann Rheum Dis 61 [Suppl 2]:ii2–7
Hoshino T, Ohta A, Yang D et al. (1998) Elevated serum interleukin 6, interferon-gamma, and tumor necrosis factor-alpha levels in patients with adult Still’s disease. J Rheumatol 25:396–398
Fujii T, Nojima T, Yasuoka H et al. (2001) Cytokine and immunogenetic profiles in Japanese patients with adult Still’s disease. Association with chronic articular disease. Rheumatology (Oxford) 40:1398–1404
Yamaguchi M, Ohta A, Tsunematsu T et al. (1992) Preliminary criteria for classification of adult Still’s disease. J Rheumatol 19:424–430
Furst DE, Cush J, Kaufmann S, Siegel J, Kurth R (2002) Preliminary guidelines for diagnosing and treating tuberculosis in patients with rheumatoid arthritis in immunosuppressive trials or being treated with biological agents. Ann Rheum Dis 61[Suppl 2]:ii62–63
Reference omitted
Hanauer SB, Sandborn W, Practice Parameters Committee of the American College of Gastroenterology (2001) Management of Crohn’s disease in adults. Am J Gastroenterol 96:635–643
Cavagna L, Caporali R, Epis O, Bobbio-Pallavicini F, Montecucco C (2001) Infliximab in the treatment of adult Still’s disease refractory to conventional therapy. Clin Exp Rheumatol 19:329–332
Kraetsch HG, Antoni C, Kalden JR, Manger B (2001) Successful treatment of a small cohort of patients with adult onset of Still’s disease with infliximab: first experiences. Ann Rheum Dis 60 [Suppl 3]:iii55–57
Huffstutter JE, Sienknecht CW (2002) Treatment of resistant Adult Still’s disease with infliximab-A report of two cases. Arthritis Rheum 46[Suppl]:326
Caramaschi P, Biasi D, Carletto A, Bambara LM (2002) A case of adult onset Still’s disease treated with infliximab. Clin Exp Rheumatol 20:113
Husni ME, Maier AL, Mease PJ et al. (2002) Etanercept in the treatment of adult patients with Still’s disease. Arthritis Rheum 46:1171–1176
Van Deventer SJH (2001) Transmembrane TNF-a, induction of apoptosis, and the efficacy of TNF-targeting therapies in Crohn’s disease. Gastroenterology 121:1242–1246
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kokkinos, A., Iliopoulos, A., Greka, P. et al. Successful treatment of refractory adult-onset Still’s disease with infliximab. A prospective, non-comparative series of four patients. Clin Rheumatol 23, 45–49 (2004). https://doi.org/10.1007/s10067-003-0775-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-003-0775-5