
Abstract
Linkage and cytogenetics studies have found the Angelman syndrome (AS) chromosomal region to be of relevance to autism disorder (AD) or autism spectrum disorder (ASD). Autism is considered part of the behavioural phenotype in AS based on formal autism assessments (autism diagnostic interview—revised [ADI-R] and autism diagnostic observation schedule [ADOS]), which have mainly addressed the deleted AS group. We explored 23 AS patients including all genetic subtypes and made a co-morbid diagnosis of AD/ASD in 14/23 (61%), which does not include 4 cases classified within the broader autism spectrum disorder (bASD). Deletions accounted for the main fraction (35%), ubiquitin-protein ligase E3A (UBE3A) mutation represented 13%, imprinting defects and uniparental disomy 9 and 4%, respectively. UBE3A mutations due to lack of the homologous to the E6-associated protein carboxyl terminus domain (n = 3) were associated with the ASD, while more distal mutations (n = 3) seem to escape from a co-morbid diagnosis of autism/autism spectrum. Differences in severity of autistic features were seen across subtypes of AS, with some behavioural features being unique to AS and some representing all forms of developmental disability. Autism signs (poor/lack of eye contact, showing, spontaneous initiation of joint attention, social quality of overtures [ADOS algorithm items for Diagnostic and Statistical Manual of Mental Disorders—IV (DSM-IV)/International Statistical Classification of Diseases and Related Health Problems—10 (ICD-10) autism diagnosis belonging to the reciprocal social interaction domain]) discriminating all the co-morbid AS categories from non-autistic AS belonged to the social interaction domain. Impairments in the communication domain (gestures, pointing, use of another’s body, frequency of vocalisation towards others [ADOS algorithm items for DSM-IV/ICD-10 autism diagnosis belonging to the communication domain]) justified classification of co-morbid AD/ASD vs the classification of less affected bASD. Evaluation of the behaviour domain suggested that repetitive sensory and motor behaviours correlate with a low developmental profile rather than being specific to autism.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Angelman syndrome (AS; MIM#105830; MIM, Mendelian Inheritance in Man) is a neurodevelopmental disorder characterised by severe mental retardation, absence of speech, movement or balance disorder and dysmorphic facial features [1]. The AS behavioural phenotype has been regarded as the most consistent clinical feature. A happy sociable disposition, frequent and sometimes inappropriate laughter, easily excitable personality and jerky movements [2, 3] are usually reported as specific to AS [4]. Abnormal food-related behaviours (e.g. eating non-food items, apparent increased appetite, orientation to food) are often seen in the older AS child or young adult similar to what is observed in individuals with Prader–Willi syndrome. Fascination with crinkly items, such as certain types of paper and plastic, has been recently considered to expand the well-known sensory interest of attraction to water [1].
AS is the result of functional defects in the ubiquitin-protein ligase E3A gene (UBE3A, MIM*601623) underlied by a variety of genetic abnormalities of the imprinted 15q11–q13 chromosomal region [5]. The following genetic alterations: deletion on the maternal chromosome 15 (70%), paternal chromosome 15 uniparental disomy (UPD; 2%) point mutations of the UBE3A gene (10%) and epimutations, i.e. imprinting defects (ID; 5%), have been recognised. No identifiable molecular abnormality is found in the remaining AS patients (10–13%). UBE3A shows tissue-specific imprinting, being expressed exclusively from the maternal allele in brain tissue [6]. Different mechanisms of UBE3A silencing (i.e. distinct genetic subtypes) correlate with clinical presentations of varying severity [7]. The phenotypic groups display the most pronounced differences in the achievement of developmental milestones, growth parameters, such as body mass index and head circumference, and age of onset, frequency and severity of seizures. Statistically, deletion patients are the most severely affected, while UPD and ID patients, whose phenotypes as a group were found to be indistinguishable, are the least affected, as they have a lower incidence of microcephaly and severe seizures [7, 8]. Moreover, almost half of UPD and ID patients have more than three words in their vocabulary [7, 8], while individuals harbouring Class I deletions (BP1–BP3) show a complete lack of vocalisation, and those with smaller Class II deletions (BP2–BP3) are able to produce at least some syllabic sounds [9]. UBE3A mutation patients fall in the middle: they are statistically similar to deletion patients with respect to seizures, absence of speech and microcephaly; they are similar to UPD and ID patients in the development of motor skills, ability to follow simple commands and development of early obesity [8]. Behavioural problems are present in all patients irrespective of the type of genetic/epigenetic abnormality [2]. The AS chromosome region has been found to be of relevance to the autism spectrum disorders (ASD) by numerous studies showing either linkage of 15q11–q13 chromosome region to ASD [10–12] or region-specific chromosomal rearrangements, mainly duplications of maternal origin [13–16]. To gain insights into the effects of these duplications, Baron et al. [17] carried out a genomic and functional profiling of lymphoblast cell lines derived from autistic individuals with isodicentric chromosome 15. This work demonstrated that 112 transcripts were significantly dysregulated, including UBE3A, which was 1.5- to 2.0-fold upregulated, leading to augmented ubiquitination in response to genotoxic stress. Indeed, a few features in AS, such as severe mental retardation, absence of speech, abnormal EEG/epilepsy and inappropriate social behaviour, overlap with those often seen in autism [2]. Moreover, recent studies have focused on the epigenetic involvement of UBE3A in autism [18, 19], but only a few examined the frequency and magnitude of autistic traits in AS [9, 24, 25]. Based on this evidence and the availability of a large cohort of AS patients representative of all the main genetic subtypes, we have explored the co-morbidity between AS and ASD aiming at a parallel evaluation of occurrence and expressivity of the autism-related spectrum in all known AS genetic subtypes.
Materials and methods
Patients selection and classification
Twenty-three AS patients, including eight with 15q11–13 microdeletion, two pat 15UPD, six with ID defect and seven with UBE3A mutations, were enrolled for this study. Recruitment of patients was based on the Molecular Biology Laboratory database of Istituto Auxologico Italiano and was supported by the Italian Angelman Syndrome Association, Organizzazione Sindrome di Angelman (ORSA). Assessments were carried out at the Clinical Genetics Centres of Istituto Auxologico Italiano (Milan) and Troina (Sicily).
The designation of the diagnosis of autism disorder (AD)/ASD included the use of the autism diagnostic observation schedule (ADOS), developed by Lord et al. [26]. Module 1 was adopted for preverbal individuals and for individuals who do not use spontaneous phrase speech consistently. The ADOS is a standardised, direct observational, semi-structured assessment tool used to help facilitate the diagnosis of ASD. It is designed to assess a child’s communication skills, the nature and quality of social interactions and the quality of play. Subjects who scored above the cut-off threshold on both the social and the communicative areas were considered to have co-morbid autism or ASD [26]. Subjects reaching cut-off scores for autism in the reciprocal social interaction area and for autism spectrum in the communication and reciprocal social interaction combined areas were defined as having a broader phenotype of autism disorder (bASD). Table 1 summarises the threshold scores in the three domains of communication and social interaction suitable to classify the patients as autism, autism spectrum and broader autistic phenotype. Whenever possible, the autism diagnostic interview—revised (ADI-R) [27] was used with parents of AS individuals who reached the ADOS cut-off scores for AD/ASD. The ADI-R is a standardised, semi-structured investigator-directed parent interview developed for use in the differential diagnosis of autism, which provides information necessary for an International Statistical Classification of Diseases and Related Health Problems—10 (ICD-10) and Diagnostic and Statistical Manual of Mental Disorders—IV (DSM-IV) diagnosis of autism. Three areas of functioning are assessed by ADI-R, including communication and language skills, the nature and quality of reciprocal social interactions, and repetitive behaviours and stereotyped patterns of behaviour. ADI-R items are of value in understanding the communication and social skills at 4–5 years of age in older subjects and in providing additional information on the behavioural domain, which may add useful information regarding the current behavioural items. All parents of AS patients who could be interviewed were asked about the repetitive behaviours and stereotyped patterns of their children [28] irrespective of the co-morbid diagnosis.
A control group of individuals with idiopathic autism [29], characterised in the same way as the AS group by severe mental retardation and absence of speech, was also enrolled for this study. Idiopathic autism patients were given a diagnosis by the application of DSM-IV criteria and ADOS and ADI-R classifications. All patients had been previously tested and found negative for chromosomal anomalies, cryptic subtelomeric rearrangements, 15q11–q13 microduplications, fragile X and metabolic defects. A few of them were also tested for Mecp2 and UBE3A mutations and epigenetic defects of the 15q11–13 region. Age range at time of ADOS evaluation in the idiopathic group was 3 to 9 years. Those tested below age 6, continued to be non-verbal at follow-up.
Written informed consent was obtained from a parent for videotaping the ADOS assessments. The study was supported by the Ethical Clinical Research Committee of Istituto Auxologico Italiano.
Molecular testing
Methylation test and genotyping were carried out according to standard diagnostic protocols for Southern blot and bisulphite methylation polymerase chain reaction (PCR) [2, 30, 31]. Microdeletions within AS smallest region of overlap were investigated by Southern blot and hybridisation to IC3 probe provided by Dr. Buiting. PCR and sequencing conditions of UBE3A isoform 1 are available on request. Subjects with idiopathic autism, besides being subjected to extensive clinical and neuropsychological investigations, were screened out for 15q proximal microduplications. Details on polymorphic loci and bacterial artificial chromosome clones used for microsatellite segregation analysis and fluorescence in situ hybridisation studies carried out to exclude cryptic chromosomal and molecular rearrangements in the control group are available on request. All samples were obtained after informed consent.
Results
Starting from a cohort of 108 AS patients found to harbour a causative genetic/epigenetic alteration, we selected 23 patients representative of all AS genetic subtypes to perform a targeted clinical evaluation of any single or combined autistic traits. Selection started from the AS patients falling into the rare subtypes (UPD/ID defects) to include a comparable number of patients with the common lesions (deletion, UBE3A mutation). Co-morbidity of AD/ASD traits was investigated by using the ADOS and ADI-R tests as described in “Materials and methods”. Corroboration of the clinical AD/ASD diagnosis was the first main aim of this study, being the prerequisite to perform a pilot study on the distribution of AD/ASD signs across the different AS subgroups. Table 2 reports the clinical data of the enrolled 23 patients listed according to AS genetic group and, within each group, from older to younger. All patients are unrelated with the exception of cases 18 and 20, who are sisters. Clinical details, such as gender, developmental milestones, severity of mental retardation, onset and type of seizures, EEG findings, growth parameters, the presence of behavioural uniqueness and the kind of movement/balance disorder, are provided to address genotype/phenotype correlations. Clinical data of AS patients enrolled for the behaviour studies are representative of the known differences reported for the AS subgroups [1, 7, 8]. The age of patients at ADOS evaluation (shown in Table 2) ranges from 28 months to 37 years; 7/24 were adult patients. The ADI-R [27] was completed for all with the exception of parents of patients 1, 2 and 3, who were institutionalised and parents not available. After the ADOS and ADI interviews, each AS patient was classified as having (1) overt autism, (2) autism spectrum or (3) broader autistic spectrum, or displaying (4) normal behaviour and given a specific symbol accordingly (Table 2).
The patients with deletions are the most severely impaired, because the co-morbid diagnoses includes autism (6/8) or an ASD (2/8). The UPD group, which accounts for only 1–2% of AS [32, 33], included only two patients who could be examined, one having and the other lacking a co-morbid diagnosis of autism. ID patients, similar to the vast majority of ID in AS, represent primary epigenetic mutations, as no imprinting centre deletions were detected by Southern blot. Out of six ID patients, one met the criteria for the AD diagnosis, one for ASD and two displayed a bASD phenotype. Of the two negative patients, one (16) was a mosaic of ID and normal cells, as shown by the presence of a faint maternal band detected by methylation-specific PCR analysis of the SNURF–SNRPN locus (data not shown). Out of seven UBE3A-mutated patients, five were confirmed to fit the diagnosis of autism with three and two falling within the AD and bASD categories, respectively. The UBE3A mutations, mostly of novel description and not included in a previous study [31], are shown in Fig. 1.

Schematic representation of UBE3A gene: exons 1 to 7 are included in the 5′UTR and, therefore, not shown; exons 8 to 16 represent the coding sequence, while the 3′ end of exon 16 is part of the 3′UTR. Exon 9, covering >50% of coding sequence, is the target of most of UBE3A mutations. The D15S122 locus, within an intron in the 5′UTR, is also shown, as it has been associated to idiopathic autism by linkage disequilibrium [11]. The horizontal lines mark the exons encoding domains in the protein with a known function. HECT is a conserved C terminal domain involved in substrate recognition and ubiquitin transfer, targeting proteins for degradation through the proteasomal pathway. The behavioural phenotype of each of the seven UBE3A-mutated AS patients (patients 17_23 whose clinical features are reported in Table 2) is depicted by the symbols used in Table 2
In summary, 6/8 deleted, 1/2 UPD and 1/6 ID patients received the ADOS classification of autism (8/23 = 35%). Two deleted patients, one belonging to the ID group and three out of seven with UBE3A mutation fitted the autism spectrum category (6/23 = 26%). A co-morbid diagnosis of AD/ASD was therefore made in 61% (14/23) of the AS patients enrolled for this study. The remaining patients were either not classified as being on the spectrum (5/23 = 22%) or belonging to the broader autism phenotype (4/23 = 17%; Table 3).
A few annotations should be made about clinical characteristics in relation to the autism diagnostic groups. None of AS patients included in this study spoke in sentences; the individual with a mosaic ID regularly used ‘who is’ and ‘what is’ and mimicked the intonation of more complex sentences, as only single words/word approximations were recognisable. Nine patients (5, 9, 13, 15, 16, 17, 19, 20, 23) regularly used few single words/word approximations other than ‘mama’ and ‘dada’ with a range number of 1–18 and most of them with three words (only individuals 16 and 19 consistently used extra words: 12 and 18, respectively). When excluding patient 5 (AD) and 17 (ASD), AS subjects with better expressive verbal skills did not meet the AD/ASD criteria.
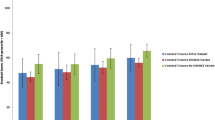
The ADOS items that appeared to discriminate the less affected broader autistic phenotype from the autism spectrum were the frequency of vocalisation directed to others, use of another’s body to communicate, pointing, gestures and response to joint attention (Fig. 2a,b). ADOS items appearing to discriminate AS patients with AD from those with the milder ASD were unusual eye contact, shared enjoyment in interaction and response to joint attention (Fig. 2b,c). Statistical analyses were not carried out because of low numbers in each AS and autism co-morbid group.

Scores (0, 1, 2 on the Y-axis) comparison of ADOS algorithm items (X-axis) in the three groups of co-morbidity of AS with: the broader phenotype of autism (a), the autism spectrum (b), autism (c) and in the co-morbidity of the latter AS-autism group and an equivalent group of ‘idiopathic’ autism (d). Scoring of zero (represented like a small rectangle for visualization purposes) corresponds to a normal behaviour, while scoring of 2 indicates a severely abnormal behaviour. For ‘unusual eye contact’ item, the choice of 1—for abnormal behaviour—is not contemplated in the ADOS protocols
A non-statistical comparison of social and communication ADOS diagnostic algorithm items between the AD AS group (eight) and eight idiopathic autism patients was also undertaken. Deficits in both domains of the co-morbid autism group mirrored those of the idiopathic autism patients, with a quantitative difference in the following items: frequency of vocalisation directed to others, pointing, gestures, facial expressions directed to others, shared enjoyment in interaction, showing, response to joint attention and quality of social overtures, all of which were more severe in the idiopathic group. Unusual eye contact and spontaneous initiation of joint attention were equivalent, while the use of another’s body to communicate was more frequently abnormal in the AS group (Fig. 2c,d).
The behaviours domain, which includes repetitive sensory and motor behaviours and interests (RSMB) and insistence on sameness (IS), for describing behaviour of individuals who display greater difficulties with compulsions/rituals and resistance to minor changes, was investigated. Significant differences did not emerge among the AS patients classified in the different autism subgroups. Indeed, RSMB were recognised in all Angelman patients regardless of ASD status, suggesting that the RSMB domain correlates with a low developmental profile, rather than being specific of autism, as reported for idiopathic autism [28]. It was instead the quality of hand/upper limb mannerisms (uplifted hand flapping, jerky movements, hands closed in a fist), an excessive/repetitive use of gestures, an idiosyncratic response to smell (retching), as well as the presence of an easily excitable personality, frequent smiling/laughter outbursts, which were unique for AS, irrespective of the autism status. Among RSMB, jerky movements, uplifted hand flapping and behavioural uniqueness (Table 2) have been reported as consistent diagnostic criteria for the syndrome. Hands close in a fist, an excessive/repetitive use of gestures and an idiosyncratic response to smell (retching) were found to be peculiar for AS compared to idiopathic autistic individuals. Characterisation of the hand/upper limb mannerisms, the gestures and the behavioural uniqueness (Table 2) was based on a targeted re-examination of ADOS videotapes of all AS patients. ‘Frequent’ (ν) means that the behaviour occurred in a consistent portion of the evaluation (at least a half). The behavioural uniqueness was found in 8 out of 23 AS patients, of which 6 received a co-morbid diagnosis of AD/ASD. Therefore, the behaviour specifically associated with AS may be, at least in a portion of patients, only apparently sociable and may mask the additional autistic features associated with social communication difficulties.
Discussion
Based on studies systematically addressing the evaluation of autism symptoms in AS [22–24], autism is considered part of the behavioural phenotype found in AS. Sahoo et al. [9] found, in formal autism assessments, co-morbid diagnoses of autism and AS in 50% (11/22) of deleted patients, most carrying the larger Class I deletions. Peters et al. [23] also explored, in formal autism assessments, the co-morbidity of AD in two UPD and in one mutated AS patient, excluding a co-morbid diagnosis of autism in all except one of the two UPD cases. Likewise, Trillingsgaard and Ostergaard [24] found a co-morbid diagnosis in 81% (13/16) of deleted AS patients: 10 out of 13 fulfilled the ADOS criteria for autism diagnosis, with the remaining 3 for an ASD. Before these studies, autism had been linked with AS only by description of four children carrying the typical maternal deletion [20] and was not linked for one case with UPD [21]. The deleted group has been the most investigated among the genetic subtypes and is the group for which the percentage of co-morbid diagnoses of autism is highest, ranging from 50 [9] to 80 [24] up to 100% [20]. We found a co-morbid diagnosis of autism/autism spectrum in 61% of Angelman patients. All the known genetics subtypes, represented in similar proportion in the sample here investigated, if we consider UPD and ID Angelman patients as unique groups [7, 8], account for this percentage. As 8 out of the 14 co-morbid diagnoses are deleted Angelman patients (Table 3), this subgroup with a more severe phenotype is significantly associated with a co-morbid diagnosis of autism. Therefore, the differences reported in Steffenburg et al. [20] and Thompson and Bolton [21] studies may be due to examination of a different subset of children with AS. Our two milder co-morbid deleted AS patients (3 and 8) may carry a Class II or an atypical deletion. Based on our very small sample, the UPD group appears to be variegated with reference to the autism spectrum phenotype, as one UPD had a co-morbid diagnosis of autism and the other did not. Expansion of the sample would be useful in finding the proportion of co-morbid diagnoses in this group. To the best of our knowledge, the ID group has never been investigated before for a co-morbid diagnosis of AD/ASD. With regard to the dual diagnosis of AS and autism, the ID subset well represents the whole autism spectrum, having the full range of severity of autistic features. Conversely, none of the UBE3A-mutated patients here evaluated fulfilled the criteria of full autism. Within this subgroup, mutations leading to lack of the homologous to the E6-associated protein carboxyl terminus (HECT) domain function (patients 17, 18, 22) fitted the ASD, while mutations saving the cysteine catalytic site in the distal HECT domain (patients 19, 21, 23) seem to escape from a co-morbid diagnosis of autism/autism spectrum (Fig. 1) raising a possible genotype/phenotype correlation that might be looked for in future studies. In patient 23, the 22 nt duplication, which starts at aminoacid 805 and stops translation after 25 aa, spares other functional sites and the 3D structure of the protein. Accordingly, RNA analysis from patient 23’s blood shows the presence of both the normal and the UBE3A mutated transcript (data not shown), whose fate, however, remains to be established. We cannot exclude that the transcript may be degraded by an RNA decay mechanism in patients carrying aminoterminal mutation. Only patients carrying UBE3A frameshift mutations have been here considered; it remains to evaluate whether missense mutations patients have a milder or null expression of autistic features. The finding that patient 20 carries, like her elder sister (patient 18), a mutation (c311dupA) affecting proximally the HECT domain, but displays a milder behavioural phenotype, might be due to one (or more) modifier gene/s whose product(s) may interact in a epistatic manner with UBE3A protein. The difference could also be due to earlier educational and psychological interventions. One may extrapolate that AS patients belonging to each class can receive a co-morbid diagnosis of autism and/or autism spectrum and that less severe autistic symptoms are associated with patients with the UBE3A mutation, UPD or ID compared to those with the deletion.
AD is a common neurodevelopmental disorder of complex genetic aetiology. According to the proposed polygenic model, several synergistically acting genes in an unfavourable genotypic combination may be required to produce the full autistic phenotype [34, 35]. Our working hypothesis was that the AS critical region is a candidate to harbour autism susceptibility genes besides UBE3A, which can be considered as the main susceptibility gene for predisposing AS patients to AD/ASD. The clinical category of broader ASD was introduced to get higher sensitivity in picking up autism signs, as there is a continuum within the autism spectrum and from this spectrum to typical behaviour and social communication. However, this mild phenotypic category, which is important for clinical follow-up and rehabilitation, is not included in the computation of the overall co-morbidity.
The higher incidence of autism traits in AS patients carrying classical or variant AS microdeletion as compared to all the other AS subtypes might indicate that, apart from UBE3A, additional flanking genes contribute to the expression of overt autism by cumulative or synergic action. Autism candidates, the non-imprinted in Prader–Willi/Angelman syndrome (NIPA)-1, NIPA-2, cytoplasmic fragile X mental retardation 1 interacting protein 1 and γ-tubulin complex protein-5 genes, have been identified in the region by comparing the extent of 15q11–q13 deleted segment in co-morbid autistic-AS patients vis-à-vis to AS-only-affected patients [9]. Inclusion of all known AS genetic subtypes in the study was considered mandatory, because evidence of involvement of imprinted autism susceptibility gene/s, other than UBE3A, in the critical region could be obtained by comparing co-morbid autism in ID- and UPD-AS patients to co-morbid autism in UBE3A AS patients. The absence of co-morbidity with autism in some UPD and ID Angelman patients suggests that UBE3A haploinsufficiency is necessary but not sufficient to produce autism. On the other hand, as no UBE3A-mutated patient fulfilled the criteria for autism, compared to the UPD and ID group, duplication of this data, by testing a higher number of AS patients carrying the UBE3A mutation, will confirm the hypothesis that one (or more) imprinted/non-imprinted genes in the critical region are necessary for a full diagnosis of autism in Angelman patients. Further knowledge on the genotype/behavioural phenotype correlation in the mutated group will, as well, enable to determine if UBE3A is involved in the predisposition to AD/ASD, as suggested by the linkage disequilibrium findings of D15S122 locus, located within a 5′ untranslated region (5′UTR) intervening sequence of UBE3A, in idiopathic autism [11] and by studies on functional profiling of duplicated chromosome 15q11–q14 cell lines [17].
Evaluation of AS patients with autism has also allowed the definition of the signs in the different autism domains, which can discriminate the different grades of severity. The RSMB domain has been confirmed to be related to global developmental-disability factor in which repetitive motor and sensory phenomena are common, while the IS domain appears more specific to AD and it is related to more social deficits [28].
This targeted study on AS patients evaluated for autism or autism spectrum traits using a comparison group of autism idiopathic patients highlights the behaviour overlap between AD and AS consistent with an important role in autism aetiology for UBE3A and neighbouring genes.
References
Williams CA, Beaudet AL, Clayton-Smith J, Knoll JH, Kyllerman M, Laan LA, Magenis RE, Moncla A, Schinzel AA, Summers JA, Wagstaff J (2006) Angelman syndrome 2005: updated consensus for diagnostic criteria. Am J Med Genet A 140:413–418. DOI 10.1002/ajmg.a.31074
Clayton-Smith J, Laan L (2003) Angelman syndrome: a review of the clinical and genetic aspects. J Med Genet 40:87–95
Horsler K, Oliver C (2006) Environmental influences on the behavioral phenotype of Angelman syndrome. Am J Ment Retard 111:311–321. DOI 10.1352/0895-8017
Berry RJ, Leitner RP, Clarke AR, Einfeld SL (2005) Behavioral aspects of Angelman syndrome: a case control study. Am J Med Genet 132A:8–12. DOI 10.1002/ajmg.a.30154
Horsthemke B, Buiting K (2006) Imprinting defects on human chromosome 15. Cytogenet Genome Res 113:292–299. DOI 10.1159/000090844
Rougeulle C, Cardoso C, Fontes M, Colleaux L, Lalande M (1998) An imprinted antisense RNA overlaps UBE3A and a second maternally expressed transcript. Nat Genet 19:15–16
Varela MC, Kok F, Otto PA, Koiffmann CP (2004) Phenotypic variability in Angelman syndrome: comparison among different deletion classes and between deletion and UPD subjects. Eur J Hum Genet 12:987–992. DOI 10.1038/sj.ejhg.5201264
Lossie AC, Whitney MM, Amidon D, Dong HJ, Chen P, Theriaque D, Hutson A, Nicholls RD, Zori RT, Williams CA, Driscoll DJ (2001) Distinct phenotypes distinguish the molecular classes of Angelman syndrome. J Med Genet 38:834–845
Sahoo T, Peters SU, Madduri NS, Glaze DG, German JR, Bird LM, Barbieri-Welge R, Bichell TJ, Beaudet AL, Bacino CA (2006) Microarray based comparative genomic hybridization testing in deletion bearing patients with Angelman syndrome: genotype–phenotype correlations. J Med Genet 43:512–516. DOI 10.1136/jmg.2005.036913
Cook EH, Courchesne RY, Cox NJ, Lord C, Gonen D, Guter SJ, Lincoln A, Nix K, Haas R, Leventhal BL, Courchesne E (1998) Linkage-disequilibrium mapping of autistic disorder, with 15q11–13 markers. Am J Hum Genet 62:1077–1083
Nurmi EL, Bradford Y, Chen Y, Hall J, Arnone B, Gardiner MB, Hutcheson HB, Gilbert JR, Pericak-Vance MA, Copeland-Yates SA, Michaelis RC, Wassink TH, Santangelo SL, Sheffield VC, Piven J, Folstein SE, Haines JL, Sutcliffe JS (2001) Linkage disequilibrium at the Angelman syndrome gene UBE3A in autism families. Genomics 77:105–113. DOI 10.1006/geno.2001.6617
Curran S, Powell J, Neale BM, Dworzynski K, Li T, Murphy D, Bolton PF (2006) An association analysis of candidate genes on chromosome 15 q11–13 and autism spectrum disorder. Mol Psychiatry 11:709–713. DOI 10.1038/sj.mp.4001839
Repetto GM, White LM, Bader PJ, Johnson D, Knoll JH (1998) Interstitial duplications of chromosome region 15q11q13: clinical and molecular characterization. Am J Med Genet 79:82–89
Gurrieri F, Battaglia A, Torrisi L, Tancredi R, Cavallaro C, Sangiorgi E, Neri G (1999) Pervasive developmental disorder and epilepsy due to maternally derived duplication of 15q11–q13. Neurology 52:1694–1697
Thomas NS, Browne CE, Oley C, Healey S, Crolla JA (1999) Investigation of a cryptic interstitial duplication involving the Prader–Willi/Angelman syndrome critical region. Hum Genet 105:384–387. DOI 10.1007/s004399900159
Bolton PF, Dennis NR, Browne CE, Thomas NS, Veltman MW, Thompson RJ, Jacobs P (2001) The phenotypic manifestations of interstitial duplications of proximal 15q with special reference to the autistic spectrum disorders. Am J Med Genet 105:675–685. DOI 10.10012/ajmg.1551
Baron CA, Tepper CG, Liu SY, Davis RR, Wang NJ, Schanen NC, Gregg JP (2006) Genomic and functional profiling of duplicated chromosome 15 cell lines reveal regulatory alterations in UBE3A-associated ubiquitin-proteasome pathway processes. Hum Mol Genet 15:853–869. DOI 10.1093/hmg/ddl004
Samaco RC, Hogart A, LaSalle JM (2005) Epigenetic overlap in autism-spectrum neurodevelopmental disorders: MECP2 deficiency causes reduced expression of UBE3A and GABRB3. Hum Mol Genet 14:483–492. DOI 10.1093/hmg/ddi045
Makedonski K, Abuhatzira L, Kaufman Y, Razin A, Shemer R (2005) MeCP2 deficiency in Rett syndrome causes epigenetic aberrations at the PWS/AS imprinting center that affect UBE3A expression. Hum Mol Genet 14:1049–1058. DOI 10.1093/hmg/ddi097
Steffenburg S, Gillberg CL, Steffenburg U, Kyllerman M (1996) Autism in Angelman syndrome: a population-based study. Pediatr Neurol 14:131–136
Thompson RJ, Bolton PF (2003) Case report: Angelman syndrome in an individual with a small SMC(15) and paternal uniparental disomy: a case report with reference to the assessment of cognitive functioning and autistic symptomatology. J Autism Dev Disord 33:171–176
Peters SU, Beaudet AL, Madduri N, Bacino CA (2004) Autism in Angelman syndrome: implications for autism research. Clin Genet 66:530–536. DOI 10.1111/j.1399-0004.2004.00362.x
Peters SU, Goddard-Finegold J, Beaudet AL, Madduri N, Turcich M, Bacino CA (2004) Cognitive and adaptive behavior profiles of children with Angelman syndrome. Am J Med Genet A 128:110–113. DOI 10.1002/ajmg.a.30065
Trillingsgaard A, Ostergaard JR (2004) Autism in Angelman syndrome: an exploration of comorbidity. Autism 8:163–174. DOI 10.1177/1362361304042720
Veltman MW, Craig EE, Bolton PF (2005) Autism spectrum disorders in Prader–Willi and Angelman syndromes: a systematic review. Psychiatr Genet 15:243–254
Lord C, Rutter M, DiLavore PC, Risi S (2001) Autism diagnostic observation schedule manual. WPS, Los Angeles
Lord C, Rutter M, Le Couteur A (1994) Autism diagnostic interview—revised: a revised version of a diagnostic interview for caregivers of individuals with possible pervasive developmental disorders. J Autism Dev Disord 24:659–685
Shao Y, Cuccaro ML, Hauser ER, Raiford KL, Menold MM, Wolpert CM, Ravan SA, Elston L, Decena K, Donnelly SL, Abramson RK, Wright HH, DeLong GR, Gilbert JR, Pericak-Vance MA (2003) Fine mapping of autistic disorder to chromosome 15q11–q13 by use of phenotypic subtypes. Am J Hum Genet 72:539–548
Muhle R, Trentacoste SV, Rapin I (2004) The genetics of autism. Pediatrics 113:472–486
Chotai KA, Payne SJ (1998) A rapid, PCR based test for differential molecular diagnosis of Prader–Willi and Angelman syndromes. J Med Genet 35:472–475
Russo S, Cogliati F, Viri M, Cavalleri F, Selicorni A, Turolla L, Belli S, Romeo A, Larizza L (2000) Novel mutations of ubiquitin protein ligase 3A gene in Italian patients with Angelman syndrome. Human Mutat 15:387
Engel E (1997) Uniparental disomy (UPD). Genomic imprinting and a case for new genetics (prenatal and clinical implications: the “Likon” concept). Ann Genet 40:24–34
Prasad C, Wagstaff J (1997) Genotype and phenotype in Angelman syndrome caused by paternal UPD 15. Am J Med Genet 70:328–329
Bailey A, Le Couteur A, Gottesman I, Bolton P, Simonoff E, Yuzda E, Rutter M (1995) Autism as a strongly genetic disorder: evidence from a British twin study. Psychol Med 25:63–77
Pickles A, Bolton P, Macdonald H, Bailey A, Le Couteur A, Sim CH, Rutter M (1995) Latent class analysis of recurrence risks for complex phenotypes with selection and measurement error: a twin and family history study of autism. Am J Hum Genet 57:717–726
Acknowledgements
We are very thankful to the patients’ families and to the Italian Angelman Syndrome Association (ORSA) for their valuable collaboration and kindness. We would like to thank Marcello Essenziale, in Milan, and Antonio Trovato, in Troina, for videotaping and technical support. This study was partially supported by Ministry of Health, grant number: ICS 030.11-RF225 (NEMEC).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bonati, M.T., Russo, S., Finelli, P. et al. Evaluation of autism traits in Angelman syndrome: a resource to unfold autism genes. Neurogenetics 8, 169–178 (2007). https://doi.org/10.1007/s10048-007-0086-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10048-007-0086-0