
Abstract
Purpose Incisional hernia (IH) is common complication following laparotomy. Research suggests that the use of a prophylactic mesh can reduce the rate of IH. We performed an updated meta-analysis to better understand the evidence regarding prevention of IH using prophylactic mesh.
Methods
PubMed, clinictrials.gov.uk, and the Cochrane database were searched for randomised controlled trials comparing closure of the abdomen after laparotomy using a prophylactic mesh with suture closure. A meta-analysis was then performed. The primary outcome was the occurrence of IH.
Results
Eight studies were identified for inclusion in the meta-analysis with a total of 727 patients.
Primary outcome
There was a significant reduction in the occurrence of IH in the mesh group vs. the suture repair group, OR 0.14 (95% CI 0.07–0.27).
Secondary outcomes
There was a significant increase in the number of seromas in the mesh group vs. the suture repair group, OR 1.73 (95% CI 1.04–2.87). There was also a significant increase in operative time in the mesh group vs. the suture repair group SMD 0.24 (95% CI 0.00–0.48).
Conclusions
This meta-analysis found a reduction in the occurrence of IH after a laparotomy when a prophylactic mesh is used versus a suture repair. The majority of patients included in the studies were deemed to be at high risk of IH. There appears to be sufficient evidence to recommend the use of a prophylactic mesh during laparotomy in high-risk patients.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Incisional hernia (IH) is a common complication following laparotomy, affecting 5–20% of midline laparotomies [1, 2]. Complications include bowel obstruction, strangulation, and perforation sometimes necessitating emergency surgery. Even in the absence of these severe complications, IH has a negative impact on quality of life [3]. Whilst repair is possible recurrence rates are high, 32% with mesh repair [4].
Risk factors for developing an IH can be divided into patient factors and surgery related factors. Patient factors include diabetes, smoking, obesity, corticosteroids, and connective tissue disorders, including patients with an abdominal aortic aneurysm [1]. Factors related to surgery include the incision, the suture material, and the suture length-to-wound length ratio [5].
The standard method for closure of the abdominal wall is en-mass using slowly absorbable suture monofilament suture, with a suture length to wound length ratio of at least 4:1 [6]. Recent research suggests that addition of a prophylactic mesh can reduce the rate of IH [7, 8]. Several meta-analyses conducted have found that this method reduces the incidence of IH when compared to closure with sutures alone [9,10,11], although the quality of included RCTs was low and there were limited data regarding other outcomes. Since the meta-analysis was performed by Timmermans et al. [11], further four studies have been published. The meta-analyses performed by Borab et al. and Wang et al. included both absorbable and non-absorbable meshes; in addition, the former only included patients with at least one risk factor for IH. This meta-analysis excludes studies investigating absorbable or biologic meshes, to investigate the effect of prophylactic non-absorbable mesh placement in the general population.
Methods
This meta-analysis was undertaken in line with the PRISMA statement [12].
Eligibility criteria
The following inclusion criteria were applied: Prospective randomised controlled trials, looking at surgery using a midline incision in an adult population, comparing the insertion of a non-absorbable synthetic mesh during closure with standard en-mass closure without mesh, with a follow-up period of at least 12 months. There were no restrictions on dates published or language. Only published data were included in this meta-analysis.
Search strategy
PubMed, clinictrials.gov.uk, and the Cochrane database were searched using the following terms:
PubMed
((“Surgical Mesh”[Mesh]) OR “Prostheses and Implants”[Mesh]) OR (mesh OR implant OR prosthes*) AND (“prevention and control”[Subheading]) OR (prophylax* OR prevent*) AND “Hernia”[Mesh] AND (Randomised Controlled Trial[ptyp]).
Clinicaltrials.gov.uk and Cochrane database
(“mesh” OR “prosthesis” OR “implant”) AND “laparotomy” AND “hernia”.
The search was limited to randomised controlled trials in humans. The titles and abstracts were screened by RP and JA and reference lists of included studies were screened manually, along with those of previous meta-analyses for additional studies.
Study selection
After the initial screening of titles and abstracts, publications were selected for full-text review. The eligibility criteria were applied to these papers to identify studies for inclusion.
Data collection
Data were extracted from the identified publications by RP and recorded in Review Manager 5.3. Data entry was verified by JA.
The primary outcome was the occurrence of an IH during post-operative follow-up period. Secondary outcomes included operative duration, time to discharge, mortality and the occurrence of chronic pain, partial wound dehiscence, haematoma, and wound infection.
Assessment of bias
Each study included was assessed for bias using the Cochrane Collaboration’s tool [13] for the assessment of bias independently by RP and JA. Areas of discrepancy were resolved by discussion with SW.
Data analysis
Data were analysed using Review Manager 5.3 [14]. Pooled odds ratios were calculated and standardised mean differences with an inverse variance method were calculated for discrete and continuous data, respectively. A random-effects model was used in all analyses as study populations varied. The I 2 value of heterogeneity was calculated for each analysis undertaken. Publication bias was assessed with the aid of funnel plots.
A further sub-analysis was undertaken comparing sublay-to-onlay mesh placement.
Results
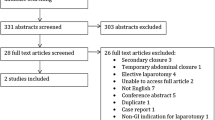
The search resulted in 475 studies. After screening titles and abstracts, 21 papers were selected for full-text review. After applying the eligibility criteria eight of these studies remained in the analysis. The PRISMA flow diagram is shown in Fig. 1.

Prisma diagram showing flow of citations through systematic review process
There were 727 patients included in this meta-analysis. There was variation in the populations selected for each study: two studies recruited patients undergoing abdominal aortic aneurysm repair [8, 15]; two recruited patients having open bariatric surgery [16, 17]; two selected patients with risk factors for IH [18, 19]; one included all elective laparotomy patients [20]; and one included elective and emergency colorectal procedures [21]. Full details of the study characteristics can be seen in Table 1.
Five of the included studies placed the mesh in a sublay position [8, 15,16,17,18], posterior to the rectus muscle, whilst three used an onlay mesh [19, 21]. Follow-up ranged from 13 months to 5 years.
The assessment of bias can be seen in Fig. 2.

Assessment of bias. Figure showing the assessment of bias for each included study against the seven domains according to the Cohcrane Collaboration’s tool. + = low risk of bias; − = high risk of bias; ? = uncertain risk of bias. Created using Review Manager 5.3 [14]
Primary outcome
The primary outcome was reported for all patients included in the meta-analysis. There was a significant reduction in the occurrence of IH in the mesh group compared to the suture repair group. The pooled odds ratio was 0.14 (95% CI 0.07–0.27). There was no significant heterogeneity, I 2 16% (Fig. 3).
Both the sublay and onlay mesh subgroups showed a significant reduction in the occurrence of IH compared with the suture repair group, odds ratios of 0.16 (95% CI 0.07–0.36) and 0.11 (95% CI 0.03–0.45), respectively. In the sublay group, I 2 was 0%; however, the onlay group showed significant heterogeneity, I 2 54%.
Secondary outcomes
Secondary outcomes are recorded in Table 2. Forest plots for secondary outcomes are seen in Figs. 4, 5, 6, 7, 8, 9, 10, 11. Funnel plots for these outcomes are shown in Figs. 12, 13.
Bevis et al. [15] reported operative duration as a median and so these data were not included in the meta-analysis. There was no significant difference found in this study, median duration of 140 (range 90–300) min in the control group and 150 (90–225) min in the mesh group. Abo-Ryia et al. [16] reported no significant difference in operative time between mesh and control groups in each of the three operations included in their study, the number of patients in each group was not available and so these data could not be included in the meta-analysis.

Forest plot of incisional hernia. Odds ratio, inverse variance, 95% CI. Created using Review Manager 5.3 [14]
Discussion
This meta-analysis confirms that the occurrence of IH in patients undergoing laparotomy was significantly reduced by the placement of a prophylactic mesh, compared to closure with sutures alone.

Forest plot of seromas. Odds ratio, inverse variance, 95% CI. Created using Review Manager 5.3 [14]
Several studies included did not comment on the process of randomisation or the blinding of participants. Whilst it is not possible for the surgeon to be blinded in these studies, it is important that the outcome is assessed by an independent assessor who is blinded to the treatment to reduce the risk of outcome bias.

Forest plot of chronic pain. Odds ratio, inverse variance, 95% CI. Created using Review Manager 5.3 [14]
Previously, only patients deemed to be at high risk of IH repair have been included in randomised controlled trials. In this meta-analysis, two studies that did not limit inclusion to high-risk patients [20, 21] were included. Both of these studies found that prophylactic mesh repair reduced the incidence of IH, in this wider demographic of patients. One of these studies included patients undergoing emergency surgery; these patients also benefited from the use of a prophylactic mesh without an increase in morbidity when compared to the non-mesh group [21].

Forest plot of haematoma. Odds ratio, inverse variance, 95% CI. Created using Review Manager 5.3 [14]
Studies included in this meta-analysis had follow-up durations ranging from 12 months to 4 years. It is possible that the use of a prophylactic mesh delays the formation of an IH. Some early studies have identified that the number of incisional hernias continued to increase up to 5 years after surgery; however, large hernias and complications were less likely in those developing after 3 years [22], [23]. Conversely, a systematic review including 14,618 patients failed to show that the rate of incisional hernias increased with follow-up beyond 1 year [1]. RCTs with longer follow-up durations are required to investigate whether incisional hernias are prevented rather than deferred by prophylactic mesh.

Forest plot of hospital stay. Standardised mean difference, inverse variance, 95% CI. Created using Review Manager 5.3 [14]
Whilst chronic pain was only reported in two studies [18, 19] included in this meta-analysis, the previous studies of patients undergoing mesh repair of an IH report rates of chronic pain at 7.1% [24]. This is, therefore, an important outcome for future study.

Forest plot of mortality. Odds ratio, inverse variance, 95% CI. Created using Review Manager 5.3 [14]
There does, however, remain a debate about the optimal position for a prophylactic mesh. Whilst onlay meshes have a mechanical disadvantage when compared to a sublay mesh, they may be less time-consuming to place [21]. A Cochrane review identified two studies comparing sublay and onlay meshes for IH; it did not identify a significant difference in recurrence of hernia, satisfaction with cosmetic appearance, or infection rate [25]. A sub-analysis of each group confirmed that the reduction in IH rates was apparent in both groups; however, no RCTs comparing these prophylactic sublay and onlay meshes directly were identified.

Forest plot of operative time. Standardised mean difference, inverse variance, 95% CI. Created using Review Manager 5.3 [14]
The previous meta-analyses [9,10,11] also found significant reductions in the incidence of incisional herniae with prophylactic mesh placement. Timmermans et al. [11] concluded that there was a significant reduction in the number of incisional hernias with prophylactic mesh placement; however, there was insufficient data regarding the incidence of complications to recommend the routine use of prophylactic meshes. Our study found that the rate of seromas was significantly greater in the prophylactic mesh group; this was also concluded by Borab et al. [10]. and Wang et al. [9]. The operative time was also significantly greater in the mesh group; however, no significant difference was found for haematomas, wound infection, chronic pain, hospital stay, partial dehiscence, or mortality. These secondary outcomes were not reported across all of the studies (Table 1), limiting the conclusions that can be drawn.

Forest plot of wound dehiscence. Odds ratio, inverse variance, 95% CI. Created using Review Manager 5.3 [14]
Although these previous meta-analyses [9,10,11] have demonstrated a similar reduction in the incidence of incisional herniae when both non-absorbable and biologic meshes are included, it is not clear how non-absorbable and biologic meshes compare directly with respect to rates of incisional herniae, seroma, and chronic pain. A systematic review [26] found very limited, poor quality evidence to support the use of biologic mesh to reduce the rate of incisional herniae. It concluded that there were no studies comparing non-absorbable and synthetic meshes directly and no evidence to support the use of biologic mesh to prevent incisional herniae. A trial comparing non-absorbable and biologic meshes in the closure of laparotomies is warranted.

Forest plot of wound infection. Odds ratio, inverse variance, 95% CI. Created using Review Manager 5.3 [14]
Potential concerns limiting the use of prophylactic mesh include fear of infective complications when placing a mesh in a contaminated environment. However, Bessa et al. found that polypropylene meshes could be used safely in the context of bowel resection [27]. Garcia Urena et al. [21] included patients undergoing emergency colorectal procedures and found that use of a mesh was not associated with increased rates of infection.

Funnel plots for incisional hernia, chronic pain, mortality, operative time, hospital stay, and wound dehiscence. Created using Review Manager 5.3 [14]
Recent randomised controlled trials [2, 28] have compared closure of the abdominal wall using the conventional 4:1 closure, with smaller sutures placed closer together with a higher suture length:wound length ratio. Theoretically, the smaller sutures confer an advantage as there is less tissue damaged by each stitch. These studies found lower rates of wound infection and a halved incidence of IH. In six of the eight studies included in this meta-analysis, the 4:1 rule was applied in the non-mesh group; in the other two, no comment was made on the technique used to close the abdominal wall in this group. Further randomised controlled trials comparing prophylactic mesh with closure using smaller stitches and a higher ratio of suture length to wound length are required.

Funnel plots for haematoma, wound infection, and seroma. Created using Review Manager 5.3 [14]
Another factor that must be considered is the cost associated with the use of prophylactic mesh. Whilst synthetic meshes are not as expensive as their biological counterparts, they do represent an increased cost over primary suture closure. Fischer et al. [29] conducted a cost analysis; they found the use of a prophylactic mesh after laparotomy to be more cost effective.
This meta-analysis demonstrates the benefit of prophylactic mesh placement in a combination of patients with and without risk factors for IH with minimal evidence of post-operative complications. However, a model to predict the risk of IH could reduce any unnecessary complications and save both time and money. Fischer et al. [30] studied the incidence of incisional herniae post laparotomy and associated risk factors, enabling them to create a composite risk score. In their cohort of 12,373 patients, there was a wide variation in incidence of IH from 0.5 to 20.6%, in the low and extreme risk groups, respectively. A similar study by Basta et al. [31] is risk stratified patients following bariatric surgery. They were able to accurately predict the risk of incisional herniae in this population. Both studies report increased healthcare costs associated with their higher risk groups. The use of a risk stratification model would allow healthcare providers to be more targeted when considering the use of a prophylactic mesh.
This meta-analysis has confirmed that the use of a prophylactic mesh significantly reduces the occurrence of IH after a laparotomy, with a slight increase in rates of seroma and no increase in SSI, haematoma, or chronic pain. The majority of studies only included patients deemed to be at high risk of IH, prior to operation. There appears to be sufficient evidence to recommend the use of a prophylactic mesh during laparotomy in high-risk patients. Although the evidence is limited in patients without risk factors and in emergency surgery, there appears to be a similar reduction in rates of IH when a prophylactic mesh is used, warranting further investigation.
References
Bosanquet DC, Ansell J, Abdelrahman T et al (2015) Systematic review and meta-regression of factors affecting midline incisional hernia rates: analysis of 14,618 patients. PLoS One. doi:10.1371/journal.pone.0138745
Millbourn D, Cengiz Y, Israelsson LA (2009) Effect of stitch length on wound complications after closure of midline incisions: a randomized controlled trial. Arch Surg 144:1056–1059. doi:10.1001/archsurg.2009.189
van Ramshorst GH, Eker HH, Hop WCJ et al (2012) Impact of incisional hernia on health-related quality of life and body image: a prospective cohort study. Am J Surg 204:144–150. doi:10.1016/j.amjsurg.2012.01.012
Burger JWA, Luijendijk RW, Hop WCJ et al (2004) Long-term follow-up of a randomized controlled trial of suture versus mesh repair of incisional hernia. Ann Surg 240:578–585. doi:10.1097/01.sla.0000141193.08524.e7
Diener MK, Voss S, Jensen K et al (2010) Elective midline laparotomy closure: the inline systematic review and meta-analysis. Ann Surg 251:843–856. doi:10.1097/SLA.0b013e3181d973e4
Muysoms FE, Antoniou SA, Bury K et al (2015) European hernia society guidelines on the closure of abdominal wall incisions. Hernia 19:1–24. doi:10.1007/s10029-014-1342-5
Muysoms FE, Dietz UA (2016) Prophylactic meshes in the abdominal wall. Chir. doi:10.1007/s00104-016-0229-7
Muysoms FE, Detry O, Vierendeels T et al (2016) Prevention of incisional hernias by prophylactic mesh-augmented reinforcement of midline laparotomies for abdominal aortic aneurysm treatment: a randomized controlled trial. Ann Surg 263:638–645. doi:10.1097/SLA.0000000000001369
Wang X-C, Zhang D, Yang Z-X et al (2017) Mesh reinforcement for the prevention of incisional hernia formation: a systematic review and meta-analysis of randomized controlled trials. J Surg Res 209:17–29. doi:10.1016/j.jss.2016.09.055
Borab ZM, Shakir S, Lanni MA et al (2017) Does prophylactic mesh placement in elective, midline laparotomy reduce the incidence of incisional hernia? A systematic review and meta-analysis. Surgery 161:1149–1163. doi:10.1016/j.surg.2016.09.036
Timmermans L, de Goede B, Eker HH et al (2013) Meta-analysis of primary mesh augmentation as prophylactic measure to prevent incisional hernia. Dig Surg 30:401–409. doi:10.1159/000355956
Moher D, Liberati A, Tetzlaff J, Altman DG (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. J Clin Epidemiol 62:1006–1012. doi:10.1016/j.jclinepi.2009.06.005
Table 8.5.a: the Cochrane Collaboration tool for assessing risk of bias. http://handbook.cochrane.org/chapter_8/table_8_5_a_the_cochrane_collaborations_tool_for_assessing.htm. Accessed 29 Sep 2016
Review Manager (RevMan) (2014) [Computer program] Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration
Bevis PM, Windhaber RAJ, Lear PA et al (2010) Randomized clinical trial of mesh versus sutured wound closure after open abdominal aortic aneurysm surgery. Br J Surg 97:1497–1502. doi:10.1002/bjs.7137
Abo-Ryia MH, El-Khadrawy OH, Abd-Allah HS (2013) Prophylactic preperitoneal mesh placement in open bariatric surgery: a guard against incisional hernia development. Obes Surg 23:1571–1574. doi:10.1007/s11695-013-0915-1
Strzelczyk JM, Szymański D, Nowicki ME et al (2006) Randomized clinical trial of postoperative hernia prophylaxis in open bariatric surgery. Br J Surg 93:1347–1350. doi:10.1002/bjs.5512
El-Khadrawy OH, Moussa G, Mansour O, Hashish MS (2009) Prophylactic prosthetic reinforcement of midline abdominal incisions in high-risk patients. Hernia 13:267–274. doi:10.1007/s10029-009-0484-3
de la Peña CG, Achirica CM, Domínguez-Adame E, Díez JM (2003) Primary closure of laparotomies with high risk of incisional hernia using prosthetic material: analysis of usefulness. Hernia 7:134–136. doi:10.1007/s10029-003-0124-2
Caro-Tarrago A, Casas CO, Salido AJ et al (2014) Prevention of incisional hernia in midline laparotomy with an onlay mesh: a randomized clinical trial. World J Surg 38:2223–2230. doi:10.1007/s00268-014-2510-6
García-Ureña MÁ, López-Monclús J, Hernando LAB et al (2015) Randomized controlled trial of the use of a large-pore polypropylene mesh to prevent incisional hernia in colorectal surgery. Ann Surg 261:876–881. doi:10.1097/SLA.0000000000001116
Höer J, Lawong G, Klinge U, Schumpelick V (2002) Factors influencing the development of incisional hernia. A retrospective study of 2,983 laparotomy patients over a period of 10 years. Chir 73:474–480. doi:10.1007/s00104-002-0425-5
Mudge M, Hughes LE (1985) Incisional hernia: a 10 year prospective study of incidence and attitudes. Br J Surg 72:70–71. doi:10.1002/bjs.1800720127
Langbach O, Bukholm I, Benth JŠ, Røkke O (2016) Long-term quality of life and functionality after ventral hernia mesh repair. Surg Endosc. doi:10.1007/s00464-016-4850-9
den Hartog D, Dur AHM, Tuinebreijer WE, Kreis RW (2008) Open surgical procedures for incisional hernias. Cochrane Database Syst Rev 3:CD006438. doi:10.1002/14651858.CD006438.pub2
Muysoms FE, Jairam A, López-Cano M et al (2016) Prevention of incisional hernias with biological mesh: a systematic review of the literature. Front Surg 3:53. doi:10.3389/fsurg.2016.00053
Bessa SS, Abdel-fattah MR, Al-Sayes IA, Korayem IT (2015) Results of prosthetic mesh repair in the emergency management of the acutely incarcerated and/or strangulated groin hernias: a 10-year study. Hernia 19:909–914. doi:10.1007/s10029-015-1360-y
Deerenberg EB, Harlaar JJ, Steyerberg EW et al (2015) Small bites versus large bites for closure of abdominal midline incisions (STITCH): a double-blind, multicentre, randomised controlled trial. The Lancet 386:1254–1260. doi:10.1016/S0140-6736(15)60459-7
Fischer JP, Basta MN, Wink JD et al (2015) Cost-utility analysis of the use of prophylactic mesh augmentation compared with primary fascial suture repair in patients at high risk for incisional hernia. Surgery 158:700–711. doi:10.1016/j.surg.2015.02.030
Fischer JP, Basta MN, Mirzabeigi MN et al (2016) A risk model and cost analysis of incisional hernia after elective, abdominal surgery based upon 12,373 cases. Ann Surg 263:1010–1017. doi:10.1097/SLA.0000000000001394
Basta MN, Mirzabeigi MN, Shubinets V et al (2016) Predicting incisional hernia after bariatric surgery: a risk stratification model based upon 2161 operations. Surg Obes Relat Dis 12:1466–1473. doi:10.1016/j.soard.2016.03.022
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
R. Payne, J. Aldwinckle, and S. Ward declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Human and animal rights
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
Formal consent is not required for this type of study.
Rights and permissions
About this article

Cite this article
Payne, R., Aldwinckle, J. & Ward, S. Meta-analysis of randomised trials comparing the use of prophylactic mesh to standard midline closure in the reduction of incisional herniae. Hernia 21, 843–853 (2017). https://doi.org/10.1007/s10029-017-1653-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10029-017-1653-4