
Abstract
Purpose
The primary objective was to describe 30-day outcomes after primary inguinal paediatric hernia repair.
Methods
Prospectively collected data from the National Patient Registry covering a 2-year study period 1 January 2005 to 31 December 2006 were collected. Unexpected outcomes were defined as either/or hospital stay for >1 day (i.e. 2 nights at hospital or more), readmission within 30 days, reoperations within 12 months after repair including repair for recurrence, and death within 30 days after repair.
Results
The study cohort comprised 2,476 patients, and unexpected outcome was found in 267 patients/repairs (10.8 %). Prolonged hospital stay was by far the most prevalent indicator of unexpected outcome. Prolonged hospital stay was in 8.2 %, readmission in 2.1 %, reoperation in 0.7 %, and complications were observed in 1.1 %. One patient died within 30 days after repair, but death was not associated with the inguinal hernia repair. The usual technique was a simple sutured plasty (96.5 %). Emergency repair was performed in 54 patients (2.2 %) mainly in children between 0 and 2 years (79.6 %). During the 1 year follow-up, reoperation for recurrent inguinal hernia was performed in 8 children after elective repair (recurrence rate 0.3 %). Paediatric repairs were for most parts performed in surgical public hospitals, and most departments performed less than 10 inguinal hernia repairs within the 2 years study period.
Conclusion
These nationwide results are acceptable with low numbers of patients staying more than one night at hospital, low morbidity, and no procedure-related mortality.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
There is a lack of evidence for early outcome in terms of hospital stay, reoperation rate, and morbidity as well as the choice of method for repair for inguinal hernia in children [1–5]. Also, it has not been established whether it is necessary to operate or if watchful waiting can be used in children with inguinal hernia [1]. In Denmark, we have for many years perioperatively registered patients >18 years old within the frames of the Danish Hernia Database [6–8]. Thus, the Danish Hernia Database has been a success to improve surgical outcome with special reference to recurrence, choice of method for repair, type of anaesthesia, and focus on chronic pain [7]. In contrast, there is no national data on operative activity and surgical outcome after paediatric inguinal hernia repair.
The primary aim of the present study was to describe unexpected outcomes in terms of prolonged hospital stay, 30-day readmission and mortality as well as reoperations of any kind within the first year after primary inguinal hernia repair in children. We also registered frequency of emergency repair and hospital activity in terms of number of repairs per department in Denmark during the 2-year study period.
Methods
Results were based upon prospectively collected data from the National Patient Registry (NPR) covering the period 1 January 2005 to 31 December 2006. The NPR does not provide information on individual surgical expertise, number of surgeons, number of procedures per surgeon, or hernia size. Although not validated specifically for paediatric hernia repair, the high data quality of NPR with respect to the type of surgical procedure, independent of diagnosis, has been demonstrated previously for several other surgical procedures [9–11]. Since inguinal hernia repair in children aged 0–2 years usually requires specialized paediatric anaethesiologic service, we divided the data set into the age groups 0–2 years, 3–7 years, and 8–17 years (patients of 18 years or older were not included). At the primary operation, the code for diagnosis was K409 (ICD10 code for unilateral inguinal hernia), but the diagnosis at readmissions were not restricted as inclusion criteria for the study. Thus, all reoperations and readmissions were included.
We used four indicators to identify unexpected outcome: Either/or hospital stay for >1 day, that is, 2 nights at hospital or more; readmission within 30 days; reoperations within 12 months after repair including repair for recurrence; and death within 30 days after repair. We excluded children with contralateral repair within the inclusion- and follow-up period (see below). Also, before study start, it was decided that repairs were excluded from analysis in case of missing file information, cancellation of operation, or preoperative admittance to hospital >1 day before hernia repair (the latter exclusion criterion was to focus on uncomplicated elective repairs). For all patients with unexpected outcome, for repairs other than sac removal or simple suture repair (operation code JAB00 and JAB10), and for emergency repairs, a copy of the patient’s file was obtained from the surgical department for detailed analysis. If the operation code was wrong (e.g. if the code was given as JAB30, and no mesh was used), then we corrected the code in the present analysis. Within this group, we defined emergency repair as a procedure in patients coming to hospital without a beforehand planned inguinal hernia repair. Thus, the present data set has been verified against the source data as described elsewhere [9, 12].
This type of study did not require approval by The Local Ethical Committee because it is regarded as a quality assurance project. The umbrella organization at The National Board of Health for surgical outcome studies has an approval from The Danish Data Agency for these kinds of trials.
Statistics
To avoid statistical analysis within a “wrong sampling unit” (as several events may occur per patient and per surgical procedure) and thus to prevent a statistical distortion of our morbidity, readmission, and mortality results, we assessed only one complication (that is reoperation for the most severe) and/or one readmission per hernia repair [9, 12]. For data analysis, we used descriptive non-parametric statistics and 95 % confidence intervals (CI) when appropriate. The study was descriptive, and calculation of sample size was not possible, but inclusion was based on consecutive patients during a fixed study period.
Results
The study profile is shown in Fig. 1. During the 2 years study period, 2,521 repairs for paediatric inguinal hernia were performed in Denmark. Due to pre-study exclusion criteria, 45 patients were excluded leaving a study cohort of 2,476 patients.

Study profile
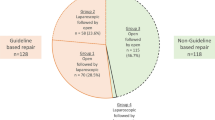
Repairs were most often performed in children between 3 and 7 years (49.8 %) followed by 0–2 years (28.9 %) and 8–17 years (21.3 %) (Fig. 2a), and mainly in boys (79 %) (Fig. 2b). The usual technique was a simple sutured plasty (96.5 % KJAB00 and KJAB10) (Fig. 2b), but mesh reinforcement by laparoscopic (laparoscopic repair (KJAB11) was done in 11 children between 8 and 17 years) or open repair (Lichtenstein repair (KJAB30) in 75 children between 8 and 17 years). Emergency repair was performed in 54 patients (2.2 %) mainly in children between 0 and 2 years (79.6 %; CI: 68.9–90.3) compared with 3–7 years (16.7 %; 6.8–26.6) and 8–17 years (3.7 %; 0.0–8.7). Emergency repairs were all included in the outcome group (see below). The cause of emergency repair was incarceration (n = 46), pain (without incarceration) (n = 7), and strangulation (n = 1). The primary hospital stay was median 0 days (range 0–14).

a Number of departments performing inguinal hernia repairs in patients between 0–2 years, 3–7 years, and 8–17 years divided into public surgical, urological, gynaecologic, and private hospitals. b Percents of repairs, males, and simple sutured repairs in patients between 0–2 years, 3–7 years, and 8–17 years. c Number of departments performing 1–9, 10–19, and 20–39, and >39 inguinal hernia repairs in patients between 0–2 years, 3–7 years, and 8–17. No. number
The group of patients with unexpected outcome counted 267 patients/repairs (10.8 %) (Fig. 1). None of these patients were coded as open mesh repairs (n = 75) or laparoscopic (mesh) repairs (n = 11). Complications were observed in 28 patients (1.1 %), and readmissions were observed in 52 patients (2.1 %) (Table 2). According to predefined criteria patients with unexpected outcome (but without a complication), there were 11 patients with no pathophysiologic reason for fever, 5 patients with pain, and one patients with botox treatment (Table 2). Prolonged hospital stay was the most prevalent indicator for unexpected outcome in the outcome group (no overlap of CI’s, Table 1). Unexpected outcome was observed in 267 (10.8 %) patients (Fig. 1) with either/or prolonged hospital stay in 8.2 %, readmission in 2.1 %, reoperation in 0.7 %, and/or death in 0.04 % (Table 1). Prolonged hospital stay, readmission, and reoperation were most often observed in 0–2 years old children (Table 2). The most frequent reasons for prolonged hospital stay, readmission, and reoperation were observation, fever, and repair for recurrence, respectively (Table 2).
One patient died within 30 days after repair overall mortality 0.04 %; a 3-week old boy underwent emergency repair due to incarceration. The child was discharged fully recovered after one day but brought dead to hospital at the 29th post-operative day after unsuccessful resuscitation. Based on autopsy and parent’s anamnesis, the cause of death was established as borderline sudden infant death not related to the inguinal hernia repair.
During the 1 year follow-up, reoperation for recurrent inguinal hernia was performed in 8 children after elective repair (recurrence rate 0.3 %). All children with recurrence repairs were readmitted to hospital within the first 30 days due to suspected recurrence, and none of the children underwent reoperation during the first 30 days for complications. In addition, one child was operated for a contralateral inguinal hernia during the first year after the index inguinal hernia repair.
Paediatric repairs were for most parts performed in surgical public hospitals (Fig. 2a), and most departments performed less than 10 inguinal hernia repairs within the 2 years study period (less than 5 repairs per year) (Fig. 2c). For the children aged 0–2 years, the repairs were performed in a total of 40 departments in Denmark, and only 4 departments performed more than 20 operations during the 2 years study period (Fig. 2c). The 3 private hospitals performed 1, 2, and 3 repairs, respectively, and the 6 urological departments performed 1, 2, 8, 9, 16, and 19 repairs, respectively. A similar pattern was found in children between 3–7 year and 8–17 years, respectively. Thus, for the children 3–7 years, the 8 private hospitals performed 1, 1, 1, 2, 4, 5, 5, and 6 repairs, respectively, during the 2 years, and the 12 urological departments performed 1, 1, 1, 1, 1, 2, 5, 5, 7, 11, 28, and 41 repairs, respectively, during the 2 years. The gynaecological department performed 1 repair during the 2 years. For the children 8–17 years, the 7 private hospitals performed 1, 1, 1, 1, 1, 2, and 2 repairs, respectively, during the 2 years, and the 8 urological departments performed 2, 2, 2, 2, 4, 7, 8, and 18 repairs, respectively, during the 2 years.
Discussion
This nationwide prospective study basically demonstrated a satisfactory early outcome following paediatric inguinal hernia repair. Hospital stay was in most patients no more than 1 day, and only few children were readmitted to hospital, and recurrence rate was less than 1 % after 1 year. Finally, surgery-related 30-day mortality was for practical reasons non-existing.
The Danish Hernia Database have published extensively in the past decade [6, 13] and contributed to improve surgical quality in patient undergoing inguinal hernia repair. However, the database does not register patients <18 years, and outcomes based on nationwide data on paediatric hernia repair has not been available. The present study was, therefore, also undertaken to analyse possible needs for surgical quality improvement as suggested by Borenstein et al. [14]. They found, in a cohort study including 20,545 paediatric repairs with results collected in a population database with a maximum of 8 years follow-up (median follow-up not specified) that paediatric surgeon specialisation and high-volume general surgeons reduced the risk of recurrence but not complications. The risk of recurrences and complications for repairs performed by paediatric surgeons and high-volume general surgeons were at the same level as in our study and in other large scale national reports [15]. In Denmark, surgical treatment for inguinal hernia in children is divided, so that children below 2 years of age are operated in dedicated paediatric surgical departments, primarily because of the presence of specialized anaesthetic care. Thus, children below 2 years of age are operated in dedicated paediatric surgical departments, whereas repairs in children between 2 and 17 years are performed in many more surgical departments, but typically, only if a medical paediatric department is available in the hospital.
The surgical method for paediatric inguinal hernia repair in Denmark and internationally at present is primarily open surgery in the groin with resection of the peritoneal sac, and if a formal inguinal canal has been established in the child, then a single or two resorbable sutures may be added at the internal ring if the surgeon evaluates the size of the annulus to be “too big” [1–3, 5]. Normally, a mesh is not used in patients below 18 years of age, but there are no national or international recommendations for the choice of surgical approach when operating for inguinal hernia in patients between 2 and 18 years of age [1, 2, 15]. Unfortunately, we do not have systematic data regarding criteria for using meshes in open or laparoscopic repairs. Regrettably, there are also no national or international guidelines on the use or not of mesh in paediatric patients with inguinal hernias. Fortunately, long-term results with respects to recurrence after inguinal hernia repairs using simple sutured plasty without a mesh are generally good.
As in all surgical procedures, there is of course an operative risk when operating for inguinal hernia in children, but the exact complication rate is unknown. All departments have probably seen infections, testicular atrophy, and recurrences. Other countries have not published national complication rates, but series from single departments have reported rates for testicular atrophy up to 10 % and recurrence rates up to 9 % [3]. The present study found only one child with ischaemic orchitis, but this specific complication may by higher since we only registered readmissions and reoperation for complications.
Like for other surgical procedures, there may be a positive effect of centralizing operations to lower complication rates for dedicated paediatric surgeons and general surgeons with a high caseload [14]. The present study showed that surgical activity was spread between regular surgical departments, urological departments, and private hospitals, and inguinal hernia repairs were performed in many departments, where most were performing less than 5 cases per year. We did not statistically compare surgical departments for outcome. The reason for this was that sample sizes for prolonged hospital stay, readmissions, reoperation, and death were too small to allow definitive conclusions based on statistical analysis. Also, we had no information on surgeons’ volume or paediatric specialisation but only centre volume.
The overall purpose of creating a surgical national database is to improve the surgical quality of care. The national inguinal hernia databases in Denmark and Sweden have been instrumental in reducing recurrence rates and the use of outdated surgical methods as well as the use of spinal anaesthesia [6–8, 13]. Overall, the surgical quality of care for paediatric inguinal hernia repair seems to be satisfactory in Denmark. Thus, establishment of a paediatric inguinal hernia database is currently not indicated. There are, however, still research questions in paediatric hernia repair that need to be addressed including long-term chronic pain [1, 16, 17], but this can preferably be done in the setting of multicenter prospective randomized controlled trials with close follow-up for specific outcome parameters as well as in large scale prospective long-term follow-up studies [16, 17].
In conclusion, our national results after paediatric inguinal hernia repair provide sufficient evidence for not promoting a prospective paediatric inguinal hernia database to improve surgical practice, despite many departments performing few procedures.
References
Rosenberg J (2008) Pediatric inguinal hernia repair—a critical appraisal. Hernia 12:113–115. doi:10.1007/s10029-007-0316-2
Lau ST, Lee Y-H, Caty MG (2007) Current management of hernias and hydroceles. Semin Pediatr Surg 16:50–57. doi:10.1053/j.sempedsurg.2006.10.007
Fette AM, Höllwarth ME (2001) Special aspects of neonatal inguinal hernia and herniotomy. Hernia 5:92–96. doi:http://www.ncbi.nlm.nih.gov/pubmed/11505656
Chinnaswamy P, Malladi V, Jani KV, Parthasarthi R, Shetty RA, Kavalakat AJ, Prakash A (2005) Laparoscopic inguinal hernia repair in children. JSLS 9:393–398. doi:http://www.ncbi.nlm.nih.gov/pubmed/16381352
Kurkchubasche AG, Tracy TB (2004) Inguinal hernia/hydrocele. Oper Tech Gen Surg 6:253–268. doi:10.1053/j.optechgensurg.2004.10.004
Rosenberg J, Bisgaard T, Kehlet H, Wara P, Asmussen T, Juul P, Strand L, Andersen FH, Bay-Nielsen M, Danish Hernia Database (2011) Danish Hernia Database recommendations for the management of inguinal and femoral hernia in adults. Dan Med Bull 58:C4243. doi:http://www.ncbi.nlm.nih.gov/pubmed/21299930
Kehlet H, Bay-Nielsen M, Hernia Database Collaboration (2008) Nationwide quality improvement of groin hernia repair from the Danish Hernia Database of 87,840 patients from 1998 to 2005. Hernia 12:1–7. doi:10.1007/s10029-007-0285-5
Nordin P, Haapaniemi S, van der Linden W, Nilsson E (2004) Choice of anesthesia and risk of reoperation for recurrence in groin hernia repair. Ann Surg 240:187–192. doi:10.1097/01.sla.0000130726.03886.93
Bisgaard T, Kehlet H, Bay-Nielsen MB, Iversen MG, Wara P, Rosenberg J, Friis-Andersen HF, Jørgensen LN (2009) Nationwide study of early outcomes after incisional hernia repair. Br J Surg 96:1452–1457. doi:10.1002/bjs.7055
Schulze S, Iversen MG, Bendixen A, Larsen TS, Kehlet H (2008) Laparoscopic colonic surgery in Denmark 2004–2007. Colorectal Dis 10:869–872. doi:10.1111/j.1463-1318.2008.01497.x
Funch-Jensen P, Bendixen A, Iversen MG, Kehlet H (2008) Complications and frequency of redo antireflux surgery in Denmark: a nationwide study, 1997–2005. Surg Endosc 22:627–630. doi:10.1007/s00464-007-9705-y
Bisgaard T, Kehlet H, Bay-Nielsen M, Iversen MG, Rosenberg J, Jørgensen LN (2011) A nationwide study on readmission, morbidity, and mortality after umbilical and epigastric hernia repair. Hernia 15:541–546. doi:10.1007/s10029-011-0823-z
Bay-Nielsen M, Kehlet H, Strand L, Malmstrøm J, Andersen FH, Wara P, Juul P, Callesen T, Danish Hernia Database Collaboration (2001) Quality assessment of 26,304 herniorrhaphies in Denmark: a prospective nationwide study. Lancet 358:1124–1128. doi:10.1016/S0140-6736(01)06251-1
Borenstein SH, To T, Wajja A, Langer JC (2005) Effect of subspeciality training and volumen on outcome after pediatric inguinal hernia repair. J Pediatr Surg 40:75–80
Vogels HD, Bruijnen CJ, Beasley SW (2010) Establishing benchmarks for the outcome of herniotomy in children. Br J Surg 97:1135–1139. doi:10.1002/bjs.7041
Zendejas B, Zarroug AE, Erben YM, Holley CT, Farley DR (2010) Impact of childhood inguinal hernia repair in adulthood: 50 years of follow-up. J Am Coll Surg 211:762–768. doi:10.1016/j.jamcollsurg.2010.08.011
Aasvang EK, Kehlet H (2007) Chronic pain after childhood groin hernia repair. J Pediatr Surg 42:1403–1408
Conflict of interest
TB, HK, JO, and JR declare no conflict of interest directly related to this study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bisgaard, T., Kehlet, H., Oehlenschlager, J. et al. Acceptable nationwide outcome after paediatric inguinal hernia repair. Hernia 18, 325–331 (2014). https://doi.org/10.1007/s10029-013-1077-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10029-013-1077-8