
Abstract
Purpose
This study compared the short-term outcomes of the non-mesh (Desarda) and mesh (Lichtenstein) methods of hernia repair among Black African patients, with regard to acute postoperative pain, day of return to normal gait, operative time and complications.
Methods
A total of 101 participants (51 in the Lichtenstein arm and 50 in the Desarda arm) were enrolled into this single centre double-blind randomised controlled trial. The outcome measures were evaluated at 1–2 h, 3, 7 and 14 days. The power of the study was set at 80%, CI at 95% and a two-sided P < 0.05 was considered statistically significant.
Results
There was no significant difference in the mean pain score (based on Visual Analogue Scale 0–10) between the study arms [3rd postoperative day (POD): 3.33 ± 1.75 for Lichtenstein and 2.73 ± 1.64 for Desarda, Effect size (CI): 0.59 (−0.088–1.272) and the scores on the 7th POD were 1.31 ± 1.19 for Lichtenstein and 1.31 ± 1.34 for Desarda, effect size (CI): 0.00 (−0.509–0.509)]. No difference was observed in regard to mean day of resumption of normal gait [2.44 ± 1.62 for Lichtenstein and 2.06 ± 1.13 for Desarda, effect size (CI): 0.08 (−0.030–0.193)]. A significant difference was recorded in regard to operative time, with the Desarda repair markedly shorter in duration [15.9 ± 3.52 min for Lichtenstein repair and 10.02 ± 2.93 min for Desarda’s repair, effect size (CI): 5.92 (4.62–7.20), P = 0.0001]. Complication rates were similar in the two study arms.
Conclusions
The results of the study showed that the effectiveness of the Desarda technique with respect to influencing the early clinical outcomes of hernia repair is similar to that of the Lichtenstein method. However, the operator in this study showed that the Desarda repair requires significantly shorter operative time.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Inguinal hernias are still the most commonly seen surgical condition in the outpatient departments of hospitals in Uganda and in most African countries. In Mulago Hospital, Uganda, emergency hernia operations constitute 68% [1] of the inguinal hernia surgery performed. A similar situation is prevalent in Ghana, where only two out of ten patients who require surgery are actually operated [2]. In Uganda, an estimated seven patients are seen in surgical outpatient department (SOPD) on each clinic day, but only two may be operated.
Several techniques have been employed in the treatment of inguinal hernias since Bassini first described his method in 1887. In Uganda, Bassini repair is still used widely despite its shortcomings [1]. The wide use of Bassini repair presents us with the undesirable complications of tension repairs such as chronic groin pain and high recurrence rates [1]. The use of a mesh for repair is not practised widely in most African countries because of its prohibitive costs. The Shouldice method, which compares closely with mesh repair, is also used only rarely in Uganda, probably because of the complexity involved in tissue dissection and repair.
The Desarda technique of inguinal hernia repair—used and acclaimed by its developer, Prof. M.P. Desarda, since 1990—seeks to overcome the challenges faced when using tension tissue-repair and mesh repair techniques. Desarda’s technique is based on the concept of providing a strong, mobile and physiologically dynamic posterior inguinal wall. The technique is simple, as well as being easy to learn and perform. It does not require complicated dissection or suturing. It does not require any foreign material, and does not use weakened muscles or transversalis fascia for repair. The results are superior to those previously published in the field of hernia surgery [3–5].
The effectiveness of the Desarda technique has not been investigated sufficiently in the African population. No sufficiently large datasets from randomised comparative studies are available to consult. In a randomised controlled study at Mulago Hospital in Uganda, Situma et al. [6] found no significant difference in short-term outcomes between modified Bassini and Desarda’s repair with regard to postoperative acute pain and resumption of normal gait.
To validate the use of Desarda’s repair in the African population, a comparison to the open mesh (Lichtenstein) method—the criterion standard—must be established. The purpose of this study is thus to compare early clinical outcomes of Desarda’s repair with those following the Lichtenstein technique for the treatment of primary inguinal hernias among adult African patients.
Materials and methods
The study was a single-centre, double-blind randomised controlled trial (only the outcomes assessor and participants were blinded), carried out at Mulago Hospital, the teaching hospital for Makerere University School of Medicine.
The study was conducted for 4 months, between April and July 2009. A total of 101 Black African patients aged 18 years and above who presented with a primary, reducible inguinal or inguino-scrotal hernia and consented to participate were enrolled consecutively into the study. A t test formula, N = [(1/q1 +1/q2) × (Zα + Zβ)2 × S2] ÷ E2 was used to determine the sample size, with a power of 80% to detect a significant difference (P < 0.05, two-sided). To detect as significant a 0.8 point difference (E) between the two groups in the mean pain scores, with a standard deviation (SD) of 1.36 from previous studies and a loss to follow up of 4%, 101 participants were required. Patients with giant inguino-scrotal hernias, obstructive uropathy or chronic obstructive pulmonary disease, and impaired mental state were excluded from the study. Using a computer-generated simple random sequence, the participants were assigned to either Desarda or Lichtenstein treatment arms. The allocations were concealed in sealed opaque envelopes.
Preparation
All operations were performed as elective day cases by the Principal Investigator (W.M.) under the supervision of a Senior Consultant surgeon. Amoxycillin-Clavulanate (1.2 g) was administered intravenously at the start of the operation. The surgical site was prepared using chlorhexidine solution. Lignocaine hydrochloride 0.5% (plus Adrenaline 1:200,000) was used as a local anaesthetic at a maximum dosage of 3 mg/kg body weight. A groin skin crease (transverse) incision measuring about 7.5 cm was employed in every participant, starting 2 cm above and medial to the pubic tubercle. The standard procedure of opening in layers (skin, fascia, external oblique aponeurosis) and subsequent herniotomy was followed for all patients. Repair of the posterior wall of the inguinal canal was then embarked on.
Interventions
The surgical procedures were carried out based on the techniques as described by Lichtenstein and Desarda [3].
Desarda technique
Details of the Desarda repair techique are illustrated in Figs. 1 and 2: The upper (medial) leaf of the external oblique aponeurosis (EOA) is sutured to the inguinal ligament from the pubic tubercle to the deep inguinal ring using 2/0 Ethilon interrupted sutures. The first 1–2 sutures are taken in the anterior rectus sheath. The last suture is taken so as to narrow the deep ring sufficiently without constricting the spermatic cord. A splitting incision is then made in this sutured medial leaf, partially separating a strip of width 1.5–2 cm. This splitting incision is extended medially up to the rectus sheath and laterally 1–2 cm beyond the deep ring. The medial insertion and lateral continuation of this strip was kept intact. A strip of the EOA is now available, the lower border of which is already sutured to the inguinal ligament.

Illustration of the Desarda repair: 1 Upper (medial) leaf, 2 interrupted sutures taken to suture the medial leaf to the inguinal ligament, 3 pubic tubercle, 4 deep ring, 5 spermatic cord, 6 lower (lateral) leaf (reproduced with permission from Prof. M.P. Desarda)

Illustration of the Desarda repair: 1 Reflected upper (medial) leaf after a strip has been separated, 2 internal oblique muscle seen through the splitting incision made in the upper leaf, 3 interrupted sutures between the upper border of the strip and conjoined muscle and internal oblique muscle, 4 interrupted sutures between the lower border of the strip and the inguinal ligament, 5 pubic tubercle, 6 Internal ring, 7 spermatic cord, 8 Lower (lateral) leaf (reproduced with permission from Prof. M.P. Desarda)
The undetached strip of the external oblique aponeurosis forms the posterior wall. The upper free border of the strip can now be sutured to the internal oblique or muscle arch lying close to it with 2/0 Nylon interrupted sutures throughout its length. The aponeurotic portion of the internal oblique muscle is used for suturing to this strip wherever and whenever possible without tension; however, it is not essential for the success of the operation. This results in the strip of the EOA being placed behind the cord to form a new posterior wall of the inguinal canal. At this stage the patient is asked to cough and the increased tension in the strip is clearly visible. The spermatic cord is placed in the inguinal canal and the lateral leaf of the EOA is sutured to the newly formed medial leaf of the EOA in front of the cord as usual, again using 2/0 Nylon interrupted sutures. Undermining of the newly formed medial leaf on both its surfaces facilitates its approximation to the lateral leaf without tension. The first stitch is taken between the lateral corner of the splitting incision and lateral leaf of the EOA. The skin is then closed by interrupted Nylon 3/0 or 4/0 vertical mattress suture, and dressed with two or three layers of haemostatic gauze with elastoplast applied to completely cover the gauze.
Lichtenstein technique
Proline mesh—Monofilament Standard Polypropylene Mesh (PMS3), Size 6 × 11 cm, manufactured by Ethicon—was used. The mesh is fashioned to fit the posterior wall of the inguinal canal. A slit 2 cm long is made in the lateral aspect of the mesh, and the spermatic cord placed between the two tails of the mesh. The cord is then tagged in the cephalad direction and the medial end of the mesh is made to overlap the pubic bone by approximately 2 cm. The mesh is then sutured to the fibro-periosteum of the pubic bone using interrupted polypropylene (Proline) 3/0 suture. The interrupted sutures are continued laterally, suturing the inferior edge of the mesh to the shelving edge of the inguinal ligament, to a point 2 cm lateral to the deep inguinal ring. The superior edge of the mesh is then secured likewise to the internal oblique aponeurosis or muscle approximately 2 cm from the aponeurotic edge, while the lower edges of the two tails are sutured to the shelving edge of the inguinal ligament to create a new deep ring made of mesh.
Finally, the cord is allowed to fall back on the strengthened posterior wall of the canal, the aponeurosis of the external oblique repaired with interrupted Proline 3/0 suture and the superficial ring reconstructed to fit snugly around the cord. This is followed by closure of the skin with interrupted nylon 3/0 suture and the wound is then dressed.
Postoperative care and follow-up
After skin closure, Diclofenac 75 mg was injected intramuscularly and the patient discharged on the following drugs and instructions:
-
Tabs Diclofenac Sodium 50 mg 8 hourly for 5 days (to be taken after meals). OR Tabs Aceclofenac 100 mg 12 hourly for 5 days (for patients with Peptic Ulcer Disease).
-
Capsules Ampiclox 500 mg 6 hourly for 5 days.
-
Instructions not to open up the wound dressing nor wet it when bathing.
-
Instructions to report back immediately in the event of excessive pain at the incision site, bleeding or wound discharge.
-
Instructions on how to fill in the pain VAS (Visual Analogue Scale for pain) at home on the 3rd POD were repeated and the patient asked to repeat them to ensure that they had been understood.
-
The patients were allowed drinks as soon as they felt like after the operation (normally 3–4 h after).
The participants were followed up at 1–2 h, 7th POD and 14th POD. Pain assessment was based on pain felt in the morning after walking 50–100 m. All patients were instructed not to restrict their normal activities and they could start routine non-strenuous work from 3–4 days after surgery. Patients were told not to drive until 3–4 days after surgery as the foot reaction time does not return to normal until then.
Study variables
The predictor variables examined were: method of inguinal hernia repair (Mesh-Lichtenstein and Non-mesh-Desarda); demographic characteristics (age, sex, BMI and occupation); and clinical characteristics (location of hernia, type of hernia based on Nyhus classification and duration of hernia). The primary outcome variables were: pain score (VAS on scale of 0–10) and time taken to return to normal gait (days). The secondary outcome variables were: operative time (min) and intra-operative complications. Normal gait was defined as the ability to walk comfortably or move freely after surgery (as measured by ability to bend, squat, kneel, stoop, climb a staircase, to drive, to carry luggage weighing 10 kg or more). Operative time was defined as the duration of the repair, counted from the beginning of a particular repair technique (after herniotomy has been performed) and ending when the last stitch of the repair is knotted, before closing the other layers of the wound.
Data analysis
Data were entered into a computer using Epidata-Entry 3.1 (http://www.epidata.dk/) and then exported to the statistical package STATA 10 (http://www.stata.com) for analysis. Analysis was based on an intention-to-treat design. Mean pain score, day of return to normal gait and operative time were compared using Student’s t test. Comparison of complication rates was performed by χ 2 (Chi-square) or Fisher’s exact test. Bivariate and multivariate analysis using t test, χ 2, analysis of variance (ANOVA) with Bonferroni tests and multiple regression analysis were done to evaluate the influence of baseline factors on the key outcomes. The power of the study was set at 80%, confidence interval at 95% and a two-sided P < 0.05 was considered statistically significant. Accuracy of randomisation was analysed using the χ 2 Contingency Table Test and evaluation of effectiveness of blinding was also analysed using percentage agreements.
Results
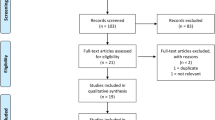
A total of 101 participants were enrolled into the study. All participants received their allocated intervention. While two participants (3.9%) in the mesh (Lichtenstein) arm were lost to follow-up, only one participant (2.0%) in the non-mesh (Desarda) arm did not complete the follow-up. However, the difference in the loss to follow-up between the study arms was not statistically significant (χ 2 = 0.323, P = 0.570) (Fig. 3).

Patients flow diagram based on the Consort guidelines [7]
Characteristics of study population
Baseline characteristics of study population are listed in Table 1. Males constituted 87% (88/101) of the subjects in this study, with a ratio of 6.8 males: 1 female. The age of the study subjects was not normally distributed, with median age at 32 years and percentile range, p25–p75 (23–50). The majority, 71/101 (71%) of the subjects had normal BMI (Table 2).
The majority of participants (62%) had inguinal hernias on the right side. There were 79/101 (78%) indirect hernias, with the majority being in Nyhus class IIIB (40%) (Tables 3, 4).
The distribution of baseline demographic and clinical characteristics was similar in the two intervention arms.
Pain score and mean day of return to normal gait
There was no significant statistical difference in mean pain scores at the four time points between the two intervention groups (P > 0.05; Table 5). However, a noticeable, but not statistically significant difference was observed on the 3rd POD, with lower mean pain scores among the non-mesh subjects (P = 0.0874). The difference, 0.39 (−0.172–0.949), of the mean day of return to normal gait between the groups was not statistically significant (P = 0.1722) (Fig. 4).

Pain score trends
The general trend showed an increase in pain score on the 3rd POD, followed by a marked decline in scores on the 7th day, with the pain score being nearly zero on the 14th day in the non-mesh group.
One-way analysis of pain score and treatment arm showed a noticeable difference in pain scores on the 3rd day. However, this was not statistically significant (Fig. 5).

Days required for return to normal gait by method of repair
The vast majority of participants in the study population returned to normal gait within 2–3 days. Four participants in the non-mesh group and three in the mesh group resumed normal gait 4 h after surgery. However, the lone participant in the mesh group who resumed normal gait on the 10th day had also developed a moderate scrotal haematoma on the 3rd POD, with pain scores of 7, 5 and 1 on the VAS on the 3rd, 7th and 14th POD, respectively (Fig. 6).

Mean day of return to normal gait for the study population by study group
Overall, the participants in the non-mesh group returned to normal gait earlier than those in the mesh group and the overall study population.
Operative time
Mesh repair took longer to accomplish, with a difference of 5.92 min (95% CI = 4.62–7.20) compared to the non-mesh repair (P = 0.0001) (Table 6, Fig. 7).

Operative time by method of repair
The great majority of participants in the mesh arm were operated within 13–20 min, whereas those in the non-mesh arm were operated within 8–11 min. Note that the operative time in this study refers to time taken to carry out only the actual repair of the posterior wall of the inguinal canal, not skin incision to skin closure time.
Complications
The proportion of participants experiencing any complications was similar between the mesh and non-mesh groups: 8 (15.7%) of 51 and 9 (18.0%) of 50, respectively (Table 7).
Intraoperatively, two male participants aged 67 and 32 years in the non-mesh group experienced injuries to the ilioinguinal and iliohypogastirc nerves, respectively, and one male participant aged 67 years in the mesh group suffered an iliohypogastric injury. However, there was no statistical difference between the two intervention arms (P = 0.617). The one ilioinguinal nerve was severed during mobilisation of the spermatic cord from the floor of the inguinal canal. Of the two iliohypogastric nerves, one was inadvertently cut in the process of mobilising the external oblique aponeurosis for the Desarda repair, and the other became torn from excessive retraction during fixation of the mesh superolateral to the deep inguinal ring. An effort was made to identify all these nerves, but the iliohypogastic nerves could not be identified in two male subjects.
On the 7th POD, eight (7.9%) participants developed moderate scrotal oedema, four (7.8%) occurring in the mesh group and four (8.0%) in the non-mesh group. Three (3.0%) scrotal haematomas were observed, two (3.9%) in the mesh group and one (2.0%) in the non-mesh group. All these complications developed in participants with indirect, especially Nyhus class IIIB, hernias. The patients with scrotal oedema and one patient with a small scrotal haematoma were managed conservatively. However, two participants with moderately sized scrotal haematomas improved after needle aspiration.
One 54-year-old male participant in the mesh group, with a Nyhus class IIIB indirect hernia of 40 years duration, developed a small seroma. It developed between the 4th and 6th POD and had subsided by the 14th POD on conservative management. None of the participants developed surgical site infection (wound sepsis). There was no statistical difference in the distribution of these complications.
On the 14th POD, four (7.8%) participants in the mesh group and one (2.0%) in the non-mesh group reported pain scores of 1–2 (VAS). This difference was not statistically significant (P = 0.168). The pain was neuropathic in nature—suggestive of nerve entrapment. All these participants had initially experienced almost complete remission of pain by the 10th POD. The same seven (6.9%) participants who had scrotal oedema on the 7th POD were found to still have it on the 14th POD. However the oedema had reduced steadily by the 14th POD.
One 25-year-old participant in the non-mesh group with a Nyhus class IIIB hernia, developed a small hydrocoele. He had presented, at the time of surgery, with a small hydrocoele on the contralateral side. Another male participant in the non-mesh group, aged 23 and with a Nyhus class IIIB hernia, reported reduced sensation at the operation site. No participant developed wound sepsis by the 14th POD. No single participant developed more than one complication at a time during the study.
Discussion
The need to find an efficient, safe but simple and affordable method of hernia repair for the African population provided the basis for this study. The study was designed to establish the short-term clinical outcomes of hernia repair using Desarda’s technique—a non-mesh tissue-only repair that is claimed to be able to restore the normal physiology of the inguinal canal as effectively as mesh-based repairs. There was no statistically significant difference between the Desarda and Lichtenstein methods with regard to acute postoperative pain scores; time to resumption of normal gait (ability to move freely, bend, squat, stoop, walk up a few stairs, or carry light weights of about 10 kg); and perioperative complications. However, the Desarda repair was found to require a significantly shorter operative time (P = 0.0001).
The pain experienced by participants in the two study arms was similar at the four time points examined (1–2 h, 3rd POD, 7th POD and 14th POD). The mean pain score was highest on the 3rd POD in both arms. The overall trend showed lower scores among the Desarda group, but this was not statistically significant (P = 0.087). The explanation for the higher scores on the 3rd POD could be that the postoperative inflammatory process is at its peak. In this study, the mean pain scores on the 3rd POD were 3.33 ± 1.75 for Lichtenstein and 2.73 ± 1.64 for Desarda [effect size (95% CI): 0.59 (−0.088–1.272)] and the scores on the 7th POD were 1.31 ± 1.19 for Lichtenstein and 1.31 ± 1.34 for Desarda [effect size (95% CI): 0.00 (−0.509–0.509)]. This was comparable to the scores in the studies by Situma et al. [6], Desarda [4], and Lau et al. [8]. Post incisional infiltration of Macaine and a combination of oral Dextropropoxyphene 32.5 mg and Voltaren suppositories 50 mg were used in the study by Lau et al. [8]. The pain scores on the 7th POD were however higher in studies by S.M. Situma and P. Kyamanywa in Uganda (personal communication). Desarda scored pain based on the mild-moderate-severe scale, and thus his scores could not be compared accurately to scores in this study.
The similarity in pain scores in the study arms possibly confirms that the Desarda repair, as claimed by its inventor and others, is indeed a tension-free tissue repair. Since the participants in this study and that of Situma experienced more pain on the 3rd POD, it is recommended that analgesics be adjusted accordingly to control pain at a particular time point after hernia surgery. The relatively low pain scores at 1–2 h after operation was most likely achieved by the prolonged analgesic effect of lignocaine induced by adrenaline 1:200,000 and by the intramascular injection of Diclofenac 75 mg given to all participants at the end of the operation.
It is interesting to note that, whereas four subjects in the mesh group reported neuropathic type pain (due to nerve injury or entrapment) only one participant in the non-mesh group developed similar pain on the 14th POD. This difference was, however, not statistically significant. All these participants had experienced almost complete remission of pain by the 10th POD. Long-term follow-up of this group of participants would help to establish if they will develop the dreaded chronic postoperative pain. Chronic postoperative pain is defined as pain that has persisted for more than 3–6 months postoperatively [9].
A multivariate analysis with multiple regression analysis established that the POD (P = 0.0001), obesity (BMI > 30) (P < 0.050), and Nyhus class IIIB hernias (P < 0.050) influenced significantly intensity of pain after hernia repair irrespective of the method used. It is not surprising that the POD influenced the pain score in this study, since the period after surgery is a known factor in modifying the course of post-injury inflammatory process. The influence by Nyhus class IIIB hernia on the pain score could be due to the more extensive raw wounds created after dissection and mobilisation of the sac from the cord. This group of participants tended to develop scrotal oedema, which may also explain the higher pain scores. Age, as reported by Lau et al. [8] and P. Kyamanywa in Uganda (unpublished; personal communication) did not seem to influence pain.
The mean day of return to normal gait was 2.44 ± 1.62 for mesh and 2.06 ± 1.13 for non-mesh [effect size (95% CI): 0.08 (−0.030–0.193)]. This difference was not significant. Four of the participants in the mesh group and three in the non-mesh group had resumed normal gait 4 h after surgery. Other studies have reported slightly higher mean day of resumption of normal gait: Situma et al. [6] (Desarda’s repair 3.62 ± 1.84 days, Bassini repair 3.62 ± 1.79 days); P. Kyamanywa in Uganda (unpublished; personal communication) (Lichtenstein 4.7 ± 1.9 days, Bassini 4.0 ± 1.8 days). In a retrospective study by Desarda [4], the mean time to return to work, was 8.48 ± 2.43 days with his technique and 12.462.1 ± 1 days in the mesh group. In another study by Desarda [3], 98.25% of patients were ambulatory with limited movement up to the bathroom within 6–8 h, whereas 97.6% experienced free movement within 18–24 h. Although the operative definition of normal gait in this study differed to some extent from that of Desarda [4], these findings seem to confirm that Desarda’s repair is comparable, if not superior, to the Lichtenstein mesh repair.
Although from analysis of variance (ANOVA), age group and Nyhus class of hernia seemed to influence slightly the participants’ day of return to normal gait, this model (P = 0.0045), further multiple regression analysis revealed that subjects aged above 60 experienced a delayed return to normal gait compared to the other age groups (P < 0.05). Although these analyses, and the associated conclusions, stand a risk of creating spurious associations, other studies have explored and found associations between age and return to normal activities [9]. In this study, Nyhus class IIIB hernias were associated with delayed return to normal gait compared with Nyhus class II hernias (P = 0.008). The explanation for the seemingly delayed return to normal gait among these two groups could possibly be due to a “senility induced” sedentary life-style among the elderly, and the relatively greater pain experienced by patients with Nyhus IIIB type hernia.
The operative time in this study was taken as the duration of actual repair technique, from the end of herniotomy (ligation of the sac) to the time of placement of the last stitch of repair (before embarking on closure of external oblique aponeurosis). The duration of 15.9 ± 3.52 min for Lichtenstein repair, and 10.02 ± 2.93 min for Desarda’s repair [effect size (95% CI): 5.92 (4.62–7.20)] was found to be statistically significant (P = 0.0001). The author, a Senior House Office in General Surgery, did all the operations. Thus the difference observed can be ascribed to the challenges inherent in the repair technique itself. However, the possibility of operator bias towards a particular method of repair could have contributed to this difference. For unbiased assessment of the operative time, a group(s) of surgeons with clearly defined skills in hernia operations based on the two repair techniques should be involved in a study. This approach would improve both the internal and external validity of such a study.
In this study, a 6–8 cm long transverse (skin crease) groin incision was employed in all patients. The operator experienced delays in mesh repair as a result of difficult retraction for the placement of sutures superolateral to the internal inguinal ring. No extra retraction was required in the Desarda repair. Situma et al. [6], on average, performed a Desarda repair in 13.26 min—2.73 min longer than required for the Modified Bassini repair. In a comparative study by Desarda [3], operative time was not assessed. Other comparative studies considered duration of operation [10, 11]; however, these could not be compared with the findings of this study because the latter studies involved other methods of hernia repair and the definition of operative time was not the same as in this study. Time, being an indispensable resource, should always be considered in the selection of the most cost-effective methods of hernia repair.
The effect of baseline demographic and clinical factors on operative time was evaluated. Participants aged above 60 years required a relatively longer operative time compared to those aged 20–29 years (P = 0.0399). Surgery on obese participants took relatively longer but this was not statistically significant (P = 0.0820). The difficulties faced in accessing the repair site in obese patients may explain these differences. Duration of hernia of more than 60 months required longer operative times than those of <60 months, but again this difference was not statistically significant (P = 0.0801). The difference in duration based on gender reported by P. Kyamanywa in Uganda was not observed in this study.
There was no significant difference between the two study arms with regard to intra-operative and postoperative complications. Desarda [4] observed rates of complications of about three times higher in the Lichtenstein mesh repair than in his novel technique. The most common complication in this study was scrotal oedema [eight (7.9%)–four (7.8%) in Lichtenstein repair and four (8.00%) in Desarda’s repair] and scrotal haematoma [three (3.0%)–two (3.9%) in Lichtenstein and one (2.00%) in Desarda]. There were no wound site haematomata. These complications were successively managed conservatively.
Virtually all complications arose in males with Nyhus class IIIB hernias, indicating the challenges involved in mobilisation and resection of the sac in this category of patients. The absence of the spermatic cord in females makes it easier to mobilise the hernia sac. The round ligament in females is often excised with the sac. In all large inguino-scrotal hernias, the sac was excised and its fundus, adherent onto or continuous with tunica vaginalis, was left in situ—this safeguards against injury to the cord structures, postoperative haematomas and scrotal oedema that may result from complete excision of the sac.
Wound sepsis was not observed in this study. Intravenous injection of Enhancin (Amoxicillin + Clavulanate) 1.2 g was administered to patients at the start of operation in this study. This may, though not exclusively, explain the absence of wound sepsis in this series. Utmost attention was paid to the routine infection control. In one study done by P. Kyamanywa in Uganda, a wound sepsis rate of 5% was recorded in the Lichtenstein group. None was observed in the Bassini group. Situma [6] reported sepsis rates of 3.8% in the Desarda group and 1.9% in the Bassini group. No prophylactic antibiotics were used in these studies. Odula reported a wound sepsis rate of 6.7% in a study involving both emergency and elective hernia repairs at Mulago Hospital [1].
The higher rate of seromas reported in a study by Samir et al. [11] and one by P. Kyamanywa in Uganda (unpublished) were not observed in this study. Seromas may result from extensive tissue dissection. The studies mentioned above showed that seromas are an inherent problem in mesh-based hernia repairs. The explanation for this is not clear; however, it is known that the mesh is invaded rapidly by fibroblasts that fill up the pores in the mesh. This could result in delayed absorption of the serous fluid accumulating in the wound after the operation, leading to seroma formation.
The absence of severe adverse events in this study demonstrates that both Desarda and Lichtenstein methods can be employed safely in day case surgery under local anaesthesia in surgical out-patient theatres of most hospitals in resource-constrained countries.
Study limitations
-
1.
The methods of assessment of normal gait and pain (by use of the Visual Analogue Scale), though widely employed, are subject to participant and observer bias. An effort was made at every stage of the trial to blind the participant and the outcomes assessor. Any possible shortcomings pertaining to the methods of data collection were due mainly to the inherent problems of these methods. The outcomes assessor was specially trained prior to the start of the trial.
-
2.
With regard to postoperative complications, notably the absence of wound sepsis in this study, its generalisation to the general population is limited only to those patients with similar baseline characteristics, and who can afford prophylactic antibiotics.
-
3.
Since the follow up of the participants in this study was designed to be completed in 2 weeks, due to the limited time and funds available, some short-term complications that possibly occurred 2 weeks postoperatively were not documented. Two months would be a suitable period of follow-up to observe most of the delayed early complications of hernia repair.
Conclusions
-
1.
This study has shown that the efficacy of the Desarda technique with respect to influencing the short-term outcomes of hernia repair is comparable to that of Lichtenstein method.
-
2.
In the operator’s hands, the Desarda repair was shown to take a significantly shorter operative time than the Lichtenstein repair. In the face of resource constraints, this should make surgeons consider the Desarda’s repair as a more cost-effective method.
-
3.
The Desarda and Lichtenstein methods can be employed safely in day case surgery under local anaesthesia in surgical out-patient theatres of hospitals in resource-constrained communities.
-
4.
This study affirmed the fact that in male patients with Nyhus class IIIB hernias, and irrespective of the technique of hernia repair used, a judicious and meticulous approach to the mobilisation and resection of the sac should be observed. Surgery in these patients is attended by more postoperative pain, delayed return to normal gait, and increased intra-operative and postoperative complications.
Recommendations
-
1.
A clinical trial comparing the Lichtenstein and Desarda methods for inguinal hernia repair involving a larger study population should be carried out in an African setting to establish the long-term efficacy of the Desarda method. In addition, there is a need for long-term follow up of the cohort of patients in this study to establish long-term outcomes such as recurrence and chronic groin pain.
-
2.
Multi-centre trials comparing the Desarda and Lichtenstein methods should be carried out at referral and district hospitals in Africa to enhance the generalisation of the results because of the anticipated heterogeneity in patient populations and centre practices. This also would help to solicit a wider range of clinical opinions concerning the Desarda method.
-
3.
We are cognisant of the fact that this was a small study. However, in view of the available literature—including the study done by Prof. M.P. Desarda—it is recommended that surgeons, surgical trainees and medical students in training schools in resource-poor communities be encouraged, through continuing medical education, to acquaint themselves with the Desarda method of inguinal hernia repair.
References
Odula PO, Kakande I (2004) Groin hernia in Mulago Hospital, Kampala. East Central Afr J Surg 9(1):48–52
Ostrow B (2005) What is the most appropriate repair for groin hernias in Africa? Surgery in Africa—Monthly Review. August issue
Desarda MP (2006) Physiological repair of inguinal hernia: a new technique (study of 860 patients). Hernia 10:143–146
Desarda M, Ghosh A (2006) Comparative study of open mesh repair and Desarda’s non-mesh repair in a district hospital in India. East Central Afr J Surg 11(2):28–34
Desarda MP (2003) Surgical physiology of inguinal hernia repair—a study of 200 cases. BMC Surgery 3: 2. doi:10.1186/1471-2482-3-2
Situma SM, Kaggwa S, Masiira NM, Katumba SK (2009) Comparison of Desarda versus modified Bassini inguinal hernia repair: a randomized controlled trial. East Central Afr J Surg 14(2):70–76
Newcombe RG (2001) Reporting of clinical trials in the JO—the consort guidelines. Br J Orthod 27(1):69–70
Lau H, Lee F (2001) Determinant factors of pain after ambulatory inguinal herniorrhaphy: a multi-variate analysis. Hernia 5:17–20
Kehlet H (2008) Chronic pain after groin hernia repair. Br J Surg 95(2):135–136
Bringman S, Wollert S, Sterberg JÖ, Smedberg S, Granlund H, Heikkinen TJ (2006) Three-year results of a randomized clinical trial of lightweight or standard polypropylene mesh in Lichtenstein repair of primary inguinal hernia. Br J Surg 93:1056–1059
Samir SA, Sasi Yallalampalli BA, Ahmad MS, Charles FB, Albo D, Berger DH (2007) Improved outcomes with the prolene hernia system mesh compared with the time-honored Lichtenstein onlay mesh for inguinal hernia repair. The Am J Surg 193:697–701
Funding
Funds were received from the following organisations: Makerere University and Mulago National Referral and Teaching Hospital.
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical standards
The study was duly approved by the Research and Ethics Committee of Makerere University College of Health Sciences. The study was also registered at http://register.clinicaltrials.gov with identifier, NCT00941941.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Manyilirah, W., Kijjambu, S., Upoki, A. et al. Comparison of non-mesh (Desarda) and mesh (Lichtenstein) methods for inguinal hernia repair among black African patients: a short-term double-blind RCT. Hernia 16, 133–144 (2012). https://doi.org/10.1007/s10029-011-0883-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10029-011-0883-0