
Abstract
The finding of a normal or inflamed vermiform appendix within an inguinal hernia is termed Amyand’s hernia. It is extremely rare in children, especially in infants and neonates. When it occurs, it is usually misdiagnosed as an irreducible or strangulated inguinal hernia, and the accurate diagnosis is made intraoperatively. We report two cases of Amyand’s hernia in premature neonates. Both patients presented on admission with signs and symptoms indicating a strangulated right inguinal hernia, and the accurate diagnosis was made intraoperatively. One of them had progressed to local peritonitis. Appendicectomy and hernia repair were made at the same time through an inguinal transverse incision, and the postoperative course was uneventful in both. We point out the need to consider acute appendicitis in the differential diagnosis of strangulated right inguinal hernia.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The presence of a normal or inflamed vermiform appendix in an incarcerated inguinal hernia is termed Amyand’s hernia [1]. The chance of finding the appendix within the inguinal hernia sac is reported to be approximately 1% when the appendix is normal and 0.08–0.13% when inflamed. It is extremely rare in infants and neonates; an accurate incidence cannot be estimated because less than twenty cases have been reported in the literature so far [2,3].
In this work we report two premature neonates with Amyand’s hernia. Both of them had an inflamed vermiform appendix within the sac of a right inguinal hernia.
Case 1
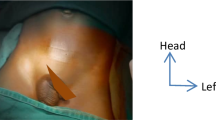
A 35-day-old premature male was admitted with a one-day history of anorexia, vomiting, mild fever, and inguinal swelling. On physical examination, an inflamed irreducible inguinal protrusion was found. Routine blood tests disclosed mild leucocytosis. Abdominal plain X-ray films were not specific and ultrasonography revealed a congested intestinal loop within the inguinal hernia. With a diagnosis of a strangulated inguinal hernia, the patient was submitted to surgical exploration through a transverse inguinal incision. An inflamed appendix, completely disconnected from its base, was found intraoperatively within the hernia sac (Fig. 1). There was also spillage of intestinal content through the open appendiceal base and the cecum was inflamed, stiffened, and attached firmly to the right iliac fossa. Appendicectomy and primary hernia repair were performed through inguinal incision. Subsequently a separate transverse abdominal incision was made to allow better surgical exposure of the appendiceal base at the cecum and to inspect the entire abdominal cavity. Local peritonitis at the right iliac fossa was found. The stump was ligated and the peritoneal cavity irrigated. The surgical wounds were closed without drainage. The postoperative course was uneventful and the histological examination of the specimen revealed an amputated gangrenous vermiform appendix.

Inflamed and completely disconnected appendix within the sac of the inguinal hernia. Arrow indicates the point of disruption
Case 2
A 32-day-old premature male was admitted with a short history of vomiting and anorexia. On physical examination an inflamed, irreducible right inguinal hernia was found. Routine blood tests revealed mild leucocytosis. Abdominal plain X-ray films were normal and ultrasonography showed an intestinal loop within the inguinal hernia. With a diagnosis of a strangulated inguinal hernia, he underwent surgical exploration through a transverse inguinal incision. Meticulous dissection of the inguinal region revealed an inflamed, vermiform appendix within the sac of an inguinal hernia. The appendix adhered to the inner surface of the sac. Appendicectomy and primary hernia repair were performed at the same time through the inguinal incision. The postoperative course was uneventful and the histological examination of the specimen revealed acute appendicitis.
Discussion
Although inguinal hernia is a common finding in premature neonates, with an incidence reaching up to 18%, acute appendicitis in this age group is very rare. Acute appendicitis in infants occurs in 2% of pediatric appendicitis cases. Neonatal appendicitis is extremely rare and represents 0.1% of all infantile cases. It has been estimated that 50% of such cases are premature neonates, and in one-third of these the inflamed appendix lies within a hernia sac [4,5]. The rarity of its occurrence in neonates and infants that are less than one year old is characterized by an inordinate delay in diagnosis and a high incidence of perforation.
During the last decade (1995–2005), 2,978 appendicectomies were performed in our department. Only two patients were premature neonates and had acute appendicitis that presented as Amyand’s hernia. The clinical and laboratory findings on admission were similar to those of a strangulated right inguinal hernia. Both patients were submitted to urgent surgical exploration via inguinal incision and the accurate diagnosis was made intraoperatively. One of them also had local peritonitis in the right iliac fossa. He was submitted to a separate laparotomy in an effort to achieve better exposure of the appendiceal base and to inspect the abdominal cavity. Both patients were submitted to hernia repair and appendicectomy at the same time through the inguinal incision.
The pathophysiology of Amyand’s hernia is unknown and the relationship between incarceration and inflammation of the appendix has not been clarified. Some authors raised the question of whether Amyand’s hernia with acute appendicitis is an incidental finding or whether there is a relationship between incarceration and inflammation [6,7]. Others, including the authors, support the theory in which the appendix becomes vulnerable to trauma as soon as it enters the sac. Its blood supply may be subsequently cut off or significantly reduced, resulting in inflammation and bacterial overgrowth. Additionally, contraction of the abdominal muscles and other sudden increases in intraabdominal pressure may cause compression of the appendix, resulting in ischemia, bacterial overgrowth, and inflammation of the appendix [8,9].
We assume that the inflammation of the appendix in our patients was secondary due to the compression of the neck of the appendix from the inguinal ring. This compression provoked vascular compromise, bacterial overgrowth, inflammation, and subsequent perforation. This hypothesis was supported by the fact that both appendices were perforated closed to their bases at the level of the inguinal ring.
Clinical presentation varies considerably, depending on the extent of the inflammation and the presence or absence of peritoneal contamination. It can present as an incarcerated–strangulated hernia, or less commonly as scrotal abscess, scrotal fistula, or as acute testicular torsion [2]. In premature neonates, a painful swelling of the inguinoscrotal region, especially when accompanied by inflammation of the surrounding soft tissues, should lead to suspicion of Amyand’s hernia.
Treatment is the urgent surgical exploration of the inguinal region. If the infection is restricted within the hernial sac, appendicectomy and primary hernia repair can be performed at the same time through the inguinal incision. Additional laparotomy may be deemed necessary in cases of peritoneal contamination. Due to delay in diagnosis, the mortality rate in the general population is high, varying from 14 to 30%, and is associated with septic complications. In contrast, the mortality rate is near zero in neonates and infants because inguinoscrotal induration and inflammation leads to early surgical intervention [5,9,10].
It is concluded that appendicitis within Amyand’s hernia is extremely rare in neonates. When it occurs it is usually misdiagnosed as strangulated inguinal hernia, which also represents a surgical emergency. It should be considered in the differential diagnosis of strangulated right inguinal hernia in premature neonates. The proper treatment is the urgent surgical exploration of the inguinal region. Appendicectomy and hernia repair can be made safely, at the same time, through the inguinal transverse incision.
References
Amyand C (1736) Of an inguinal rupture, with a pin in the appendix coeci, incrusted with stone; and some observations on wounds in the guts. Phil Trans Royal Soc 39:329
Ashraf HM, Ibrahim FR, Talal A (2000) Scrotal appendicitis mimicking acute testicular torsion in a neonate. Ann Saudi Med 20:55–56
D’Alia C, Lo Schiavo MG, Tonante A, Taranto F, Gagliano E, Bonnano L, Di Giuseppe G, Pagano D, Sturniolo G (2003) Amyand’s hernia: case report and review of the literature. Hernia 7:89–91
Kumar VH, Clive J, Rosenkrantz TS (2002) Inguinal hernia in preterm infants. Pediat Surg Int 18:147–152
Guelouz N, Rigourd V, Dommergues MA (2003) Acute neonatal appendicitis in an inguinal hernia. Arch Pediat 10:1079–1082
Bar-Maor JA, Zeltzer M (1978) Acute appendicitis located in a scrotal hernia of a premature infant. J Pediat Surg 13:182–183
Srouji MN, Buck BE (1978) Neonatal appendicitis: ischemic infarction in incarcerated inguinal hernia. J Pediat Surg 13:177
Abu-Dalu J, Ucra I (1972) Incarcerated inguinal hernia with a perforated appendix and periappendicular abscess. Dis Colon Rectum 15:464–465
Weber RV, Hunt ZC, Kral JG (1999) Amyand’s hernia: Etiologic and therapeutic implications of two complications. Surg Rounds 22:552–556
Solecki R, Matyja A, Milanowski W (2003) Amyand’s hernia: a report of two cases. Hernia 7:50–51
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Livaditi, E., Mavridis, G. & Christopoulos-Geroulanos , G. Amyand’s hernia in premature neonates: report of two cases. Hernia 11, 547–549 (2007). https://doi.org/10.1007/s10029-007-0242-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10029-007-0242-3