
Abstract
We report a case of neglected, strangulated, inguinal hernia in a middle-aged male, which presented as a scrotal fecal fistula. This is the first such case reported in an adult. The patient was treated by resection and anastamosis of the ileum, local debridement of the scrotum and Shouldice repair for the inguinal defect.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Inguinal hernia is a common surgical problem in adult males. Obstruction and strangulation are the most serious complications of this condition, while the formation of a spontaneous fecal fistula is one of the rarest, with only seven cases [1–7] documented in the literature to date, all of which occurred in children. This is the first report, of a spontaneous enterocutaneous fistula in an adult, which ultimately developed into a strangulated inguinal hernia.
Case report
A 42-year-old male presented to the emergency department with complaints of a foul smelling discharge from the scrotum that had persisted for 7 days. He had a history of a spontaneously reducing right inguinoscrotal swelling for 3 years which had become irreducible during the last month. He had been referred by the primary care physician, with the diagnosis of a Fournier’s gangrene. Local examination showed a tender inguinoscrotal swelling. The skin of the right side of scrotum had sloughed off, and there was a feculent discharge from the wound. His vital signs were normal.
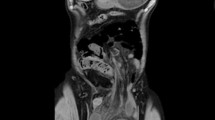
A strangulated inguinal hernia with a enterocutaneous fistula in the scrotum was diagnosed (Fig. 1). The patient was administered intravenous fluids and broad-spectrum antibiotics and was scheduled for surgery. The abdomen was opened by a lower midline incision. There were no signs of any peritoneal contamination. The bowel was dilated proximal to the herniating loop. The scrotum was explored by an inguinoscortal incision (Fig. 2) and the perforated bowel was dissected free from the scrotal adhesions. The bowel in the hernial sac was grossly edematous and sloughed out. It was resected and a single layer, end to end, extramucosal, illeo-illeal anastamosis was done to restore intestinal continuity. After a thorough irrigation of the inguinal region, the hernia was repaired by the Shouldice method. The necrotic scrotal skin and fascial layers were debribed and dressing was applied. The scrotal skin was closed 10 days later.

Picture of scrotal fecal fistula

Intra-operative picture showing inguinal and abdominal exploration
The patient made an uneventful recovery and was discharged on the 12th post-operative day. One year post-operatively, he is doing well.
Discussion
A spontaneous fecal fistula as a result of a strangulated inguinal hernia is rare. Seven such cases have been reported in the literature, all of which occurring in children [1–7]. All seven cases were reported in India and Africa, two areas where health care facilities are relatively scarce.
The patient did not have any signs of obstruction because the hernia was of the Richter’s type, and the obstruction was partially relieved after the formation of a fistula. In the other cases reported, one hernia was of the Richter’s [5] type and all of the others presented with abdominal distension and pain, along with inguinoscrotal swelling and fecal discharge from scrotum.
Scrotal strangulated herniae may be associated with testicular ischemia and infarction due to compression of the testicular vessels by the hernial sac, which would necessitate orchidectomy. The testis was, however, preserved in this case.
Necrotizing fascitis of the scrotum was reported in all of the reported cases with one exception [4]. Prompt debridement and covering of the testis with scrotal fascia should be carried out with secondary closure of the scrotal skin. Bowel continuity is established following resection of the gangrenous bowel and debridement of the scrotum.
Conclusion
Neglected incarcerated inguinal hernia may strangulate and rarely present with scrotal necrotizing fascitis and enterocutaneous fistulae.
References
Rao PL, Mitra SK, Pathak IC (1980) Fecal fistulla developing in inguinal hernia. Indian J Pediatr 47:253–255
Rattan KN, Garg P (1998) Neonatal scrotal fecal fistula. Pediatr Surg Int 13:440–441
Gupta DK, Rohatagi M (1993) Inguinal hernia in children an Indian experience. Pediatr Surg Int 8:446–468
Kasat LS, Waingankar VS, Anilkumar TK, Bahety G, Meisheri IV (2000) Spontaneous scrotal fecal fistula in an infant. Pediatr Surg Int 16:443–444
Ameh EA, Awotula OP, Amoah JN (2002) Spontaneous fecal fistula in infants. Pediatr Surg Int 18:524–525
Chidran LB, Uba AF, Iya D, Dakum NK (2004) Spontaneous scrotal fistula in a neonate: report of a case. Niger J Surg Res 6:59–60
Rao PL, Mitra SK, Pathak IC(1980) Fecal Fistulla developing in inguinal hernia. Indian J Pediatr 47:253–255
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Koshariya, M., Naik, S. & Rai, A. Incarcerated inguinal hernia presenting as spontaneous scrotal fecal fistula. Hernia 10, 434–435 (2006). https://doi.org/10.1007/s10029-006-0119-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10029-006-0119-x