
Abstract
Purpose
This study aimed to determine via systematic review and meta-analysis the proportion of maxillofacial trauma resulting from different etiologies among children and adolescents.
Methods
A systematic review of articles published from 2006 to 2015 (10 years) in English language was performed. The following databases were used: PubMed/MEDLINE, Scopus, and Web of Science. Observational studies reporting the number of children and/or adolescents who suffered maxillofacial trauma resulting from different etiologies were included. Studies were selected by two independent reviewers (Kappa = 0.737). A proportion meta-analysis using random-effect models was performed to estimate the pooled prevalence and the 95% confidence intervals (CI) using Der-Simonian and Laird weights. Heterogeneity among studies was assessed using the I 2 statistics.
Results
A total of 27 studies remained after qualitative analysis including 402,339 patients. The male/female ratio ranged from 1.5:1 to 3.5:1. Road traffic accidents corresponded to the main etiology agent of maxillofacial trauma (34%; 95% CI, 25–44), followed by falls (31%; 95% CI, 25–37), violence (11%; 95% CI, 4–19), sports (4%; 95% CI, 3–5), and others (5%; 95% CI, 2–8). Heterogeneity among studies was high, even stratifying by world region. The adapted version of the Newcastle-Ottawa scale for observational studies showed an intermediate score for most of the included studies.
Conclusions
Results suggest that road traffic accidents represent the main cause of maxillofacial trauma among children and adolescents. However, results should be interpreted with caution due to the high heterogeneity.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Trauma is an important cause of morbidity and deaths among children and adolescents [1, 2], and when the face is affected, it can lead to esthetic, functional [3, 4], and psychological problems [5, 6]. Maxillofacial trauma comprises both facial fractures and soft tissue injuries. In terms of epidemiology, children and adolescents are less affected than the adult population [7–9]. Fractures can be considered a rare event in children [10–13], but facial injuries including soft tissues occur more frequently [3, 14]. Several studies have described that less than 15% of all cases of maxillofacial fractures occur to the pediatric population [2, 13, 15–22].
There are some factors that distinguish the young population from the other age groups, for example, the facial bone of a child is distinct from that of an adult [23, 24], the cranium/face ratio is incredibly large at birth (8:1) and decreases to 2.5:1 in adults [2]. The small size of the face during childhood can influence the decrease of maxillofacial trauma and be a protective factor; however, the cranium absorbs most of the impact in trauma events [11–13].
A great number of mechanisms of occurrence related to maxillofacial trauma have been reported in children and adolescents, but the main causes remain road traffic accidents (RTA), falls, violence, and sports. Studies carried out worldwide are considerably divergent regarding the predominant etiology. Some authors have hypothesized that factors such as social environment, economy, and cultural differences can play a significant role on maxillofacial trauma causes [8, 9, 25, 26].
Although its epidemiology in children and adolescents has been extensively studied, no systematic review has been published to summarize the best literature about its etiology in the young population. Boffano [27] reported a systematic review of maxillofacial trauma; however, the authors included only facial fractures and studies were not specific to children and adolescents. To date, understanding of maxillofacial trauma etiology among young populations is controversial and limited.
In this context, this study aimed to determine via systematic review and meta-analysis the proportion of maxillofacial trauma resulting from different etiologies among children and adolescents. This systematic review can contribute to the advancement of scientific knowledge and provide a better understanding of the etiology of maxillofacial trauma among young people in different regions worldwide, which is the key point to develop public policies aimed at prevention, health promotion, and rehabilitation.
Methods
Search strategy
The present systematic review was performed based on the main consideration of PRISMA Statement–Preferred Reporting Items for Systematic Reviews and Meta-analyses [28] and some points of the Cochrane Handbook for Systematic Reviews of Interventions (version 5.1.0, updated March 2011). Although the Cochrane Handbook is more focused on interventions, some considerations are appropriate for other types of reviews [29]. Prior to the search of all relevant studies carried out from 2006 to 2015, a protocol was written to guide the review phases. This protocol included the following: (a) authors’ participation and contributions, dates of the review process, and innovation; (b) literature background up to the present moment, objectives, and design method (including databases, descriptors, idiom, inclusion and exclusion criteria, and qualitative analysis).
The PICO strategy was originally designed for systematic reviews of Randomized Clinical Trials to help healthcare professionals to choose the best evidence for clinical practice [30, 31]. For the present review, the PICO question was not as appropriated as it could, then we assumed an alternative strategy question for observational studies, the PECO question proposed by Maia and Antonio [32]. The authors consider the following stepwise for systematic reviews: P (Patient Population), I (Intervention or Exposure—in case of observational studies), C (Comparison), and O (Outcomes). Thus, the PECO approach used for the present systematic review was Population (children and adolescents with maxillofacial trauma), Exposure (etiology of maxillofacial trauma), Comparison (the different continental regions: Africa, America, Asia, and Europe), and Outcome (prevalence of maxillofacial trauma for each etiology).
The search for relevant studies was carried out on 29 November 2015. The following databases were used: PubMed/MEDLINE, Scopus, and Web of Science. Additional source was conducted by hand searching on Journals of included studies and with the reference list. The search for relevant studies was carried out on 29 November 2015. An additional search was performed on 01 January 2016, to verify if any important study was published or accepted between 30 November and 31 December.
The MeSH terms chosen for the search were facial injuries, maxillofacial injuries, etiology, epidemiology, child, pediatrics, and adolescent. In order to specify the search, the Boolean operator NOT was used to exclude the following MeSH terms: animals, burns, facial nerve, and eye, since a high number of studies are linked with these terms if we do not exclude them. The search history used on databases search was “(facial injuries OR maxillofacial injuries) AND (etiology OR epidemiology) AND (child OR pediatrics OR adolescent) NOT animals NOT burns NOT facial nerve NOT eye.”
For the selection of studies, first, those that met the following inclusion criteria were selected: studies published between 2006 and 2015 related to non-fatal victims, in English language and studies with the clear objective of investigating the etiology of maxillofacial trauma in children and/or adolescents. The concept of maxillofacial trauma in this review involves both facial fracture and/or soft tissue injury. Studies with the following characteristics were excluded: specific for one type of mechanism (e.g., specific for traffic accidents, falls, sports, or firearm) and studies regarding only one type of maxillofacial trauma (e.g., specific for orbital/nasal/zygomatic fracture, nasal epistaxis, dentoalveolar trauma, mandibular fracture, or soft tissue only), since the aim of the present review was to analyze maxillofacial trauma as a whole. In addition, 14 studies with no abstract available, 1 book chapter, and 1 study published in another language were also excluded.
The initial search (titles and abstracts) was based on reading, and the judgment decision to include or exclude was related to the eligibility criteria. After this, studies that did not meet the eligibility criteria were excluded. The second phase of the search process involved the analysis and full reading of included studies that apparently were related with the focus of the present review. On this occasion, two independent reviewers (KGNB and ÍMB) read the full articles and the Kappa coefficient was used to test the inter-reviewer agreement according to the inclusion and exclusion criteria (Kappa = 0.737). These articles were obtained on Portal Journal Capes-BR (accessed via university login). Finally, after the independent analysis and agreement assessment, divergent opinions were discussed by consensus.
Data extraction
Data extraction was performed by two independent researchers (KGNB and ÍMB). The authors used a form to extract the required information from each study under analysis. The form was developed considering the following items: (1) study objective, (2) description of the etiology of maxillofacial trauma, and (3) quality analysis (described above). For each study included after the final qualitative analysis, the following items were extracted: study period, country, study type, sample size, age (children/adolescents), source of information, type of maxillofacial trauma analyzed, main cause of maxillofacial trauma, male/female ratio, and quality score of qualitative analysis.
Methodological quality assessment
The quality of studies included after the eligibility process was peer reviewed by KGNB and ÍMB. It involves the subjective analyses of each reviewer and the observation of some pre-established aspects, such as objective, description of mechanisms, and overall quality of studies. To help with a better understanding of quality, an adapted version of the Newcastle-Ottawa scale (NOS) [33] was used for observational studies, awarding stars to eligible categories (selection, comparability, and exposure/outcome) for each article. The scale scores range from 0 (lowest grade) to 6 (highest grade). The original NOS was developed for case-control and cohort studies; however, some authors have adapted it for cross-section studies [34], using the applicable items for this type of investigation. The item comparability of NOS was not used because it is not applied for the purpose of articles included in the analysis, thus the maximum value attributed for each study is four stars.
The following NOS items used were:(a) sample selection criteria (case definition; representativeness and selection of patients) and (b) trauma evaluation (diagnosis and sample loss). For sample selection criteria, one star is attributed if the study was conducted with a clinical examination or medical record with a validated instrument or referred from a hospital. In the representativeness item, one star is attributed for studies that reported patient’s trauma in a defined hospital or clinic, in a defined area, health maintenance organization, communities, or random sample and sample calculation. The diagnosis item awarded one star for clinical examination reporting the use of a standardized scale or report of observer agreement Kappa, and the sample loss item consider one star for studies reporting sample loss ≤20%. Table 1 shows the complete scale description.
Statistical methods and data synthesis
A proportion meta-analysis using random-effect models was performed to estimate the pooled prevalence and the 95% confidence intervals (CI) using Der-Simonian and Laird weights. The random model was used in order to minimize the effect of heterogeneity among studies [35]. The variance of raw proportions was stabilized using the Freeman-Tukey double arcsine transformation [36]. Metaprop command was used so that no study with 0% or 100% proportions was excluded from the meta-analysis [37]. Heterogeneity among studies was assessed using the I 2 statistics, which describes the percentage of total variation due to inter-study heterogeneity [38]. Forest plots were constructed using the estimated proportion/prevalence of maxillofacial trauma resulting from each etiology. Analyses were performed using Stata version 14.0 (Stata Corp., College Station, USA) and StatsDirect version 3.0 software (StatsDirect Ltd., Altrincham, UK).
Results
Study characteristics
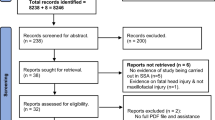
The review process yielded 1296 records, including duplicated documents. Of these, 121 were duplicated on the databases and needed to be excluded. Therefore, 1175 documents were screened by reading titles and abstracts and only 40 articles were included according to the eligibility criteria. The inter-reviewer agreement was 0.737 (Kappa coefficient). In terms of number, this Kappa value represents the disagreement of four studies. Two of them were excluded after consensus (one related to gender analysis and one review article). The final number of studies after the qualitative analysis was 27, thus, 13 of the 40 original articles were excluded. Figure 1 shows the flow diagram with all phases of the review process, including identification, screening, eligibility, and included studies.

PRISMA flow diagram of the review process
The results of studies are described in Table 2, including study period, country, study type, N (number of patients), age, source of information, type of maxillofacial trauma, etiology, male/female ratio, and quality score.
Data synthesis
Figures 2, 3, 4, 5, and 6 show the estimated proportion/prevalence of maxillofacial trauma resulting from different etiologies among children and adolescents. The combined prevalence of RTA was 34% (95% CI, 25–44) among the 27 studies. This represents the most common cause of maxillofacial trauma in children and adolescents (14 of the 27 included studies). Falls were the second leading cause of maxillofacial trauma (11 of 27), and only one study [27] did not report the number of falls. The combined prevalence was 31% (CI 95%, 25–37). Violence was the third mechanism, showing a pooled prevalence of 11% (CI 95%, 4–19). Only one study did not report events of violence [42]. The last mechanism was sports (4%; 95% CI, 3–5), and none of the studies presented sports as the first cause of maxillofacial trauma in children and adolescents.

Estimated proportion/prevalence (ES) of maxillofacial trauma resulting from RTC among children and adolescents. The prevalence in the individual studies is represented by squares, through which the horizontal lines represent the 95% CIs. The diamond at the bottom represents the pooled prevalence from these studies

Estimated proportion/prevalence (ES) of maxillofacial trauma resulting from falls among children and adolescents. The prevalence in the individual studies is represented by squares, through which the horizontal lines represent the 95% CIs. The diamond at the bottom represents the pooled prevalence from these studies

Estimated proportion/prevalence (ES) of maxillofacial trauma resulting from violence among children and adolescents. The prevalence in the individual studies is represented by squares, through which the horizontal lines represent the 95% CIs. The diamond at the bottom represents the pooled prevalence from these studies

Estimated proportion/prevalence (ES) of maxillofacial trauma resulting from sports among children and adolescents. The prevalence in the individual studies is represented by squares, through which the horizontal lines represent the 95% CIs. The diamond at the bottom represents the pooled prevalence from these studies

Estimated proportion/prevalence (ES) of maxillofacial trauma resulting from other etiologies among children and adolescents. The prevalence in the individual studies is represented by squares, through which the horizontal lines represent the 95% CIs. The diamond at the bottom represents the pooled prevalence from these studies
Eight studies [9, 23, 39, 42, 45, 46, 48, 50] did not report the number of sport-related events. Other mechanisms obtained combined prevalence of 4% (95% CI, 2–8). Ten studies [8–10, 14, 23, 39, 42, 46–48] did not report prevalence for other mechanisms. When the study region was considered, it was observed that the frequency of traffic accidents is higher in Africa and Asia and lower in Europe (which presents higher prevalence of falls). For violence events, North America, Africa, and South America regions exhibited the highest proportions. Sports and “others” were similar considering the etiology distribution.
Quality assessment
The quality of studies was evaluated using an adapted NOS, which identified four studies with the highest score [46–48, 54]. All other studies received a score of 3 according to NOS (adapted). The main points not reported in articles are related to item “sample loss.”
Heterogeneity
Differences among studies were assessed for each continent. For all etiologies, the heterogeneity observed was considerably high, even stratified by world region. It could be observed for RTA that Europe, North America, and South America presented the largest confidence interval range, as can be observed by the diamond size (Fig. 2). Falls exhibited the highest variability in Europe, showing large diamond size (Fig. 3). The violence variation was considerable more evident in North America, as can be observed in Fig. 4, and sports showed the lowest diamond size and lower variability in all studies (Fig. 5).
Other study characteristics
The period of each study was variable. However, most of them were conducted from 2000 to 2010. The distribution of studies according to the continents was the following: five from North America [23, 44, 46–48], five from South America [25, 52–55], six from Europe [1, 3, 7, 49–51], two from Africa [9, 39], and nine from Asia [8, 10, 14, 24, 40–44].
Almost all studies were retrospective, and only one multicenter research had a prospective design [7]. There was no standard for age group, and some authors considered children those aged >12 years. Most studies were conducted based on National Data Banks [45, 46, 48] and presented a large sample size. The male/female ratio was not so discrepant and ranged from 1.5:1 to 3.5:1.
Most articles included performed descriptive statistical analysis, but four studies [45, 46, 48, 49] consider logistic regression analysis for data. All 27 studies included evaluated maxillofacial fractures, and nine [1, 3, 14, 24, 25, 41, 50, 53, 55] of them added information on soft tissue injury. Table 2 shows the complete information of characteristics mentioned above and presents the quality score (stars) of each study.
Discussion
A total of 27 studies remained after the qualitative analysis, including 402,339 patients. The first point to consider is that RTA represents the main cause of maxillofacial trauma among children and adolescents. As can be observed in Fig. 2, in all continents, the total prevalence was higher than 20%. In fact, in Africa and Asia, the pooled prevalence for road accidents, which involves motor vehicle, motorcycle, bicycles, and pedestrians, was higher than 40%. This reflects the alarming situation of road traffic injuries in Africa, which was reported by the World Health Organization in the document: “Road Safety in the WHO African Region: The Facts 2013.”
According to WHO [56], the Africa region showed the highest fatality rates, an incredible rate of 27.8 deaths per 100,000 inhabitants during 2010. A curious fact is that although Africa shows the highest traffic-death rates, it remains the least motorized of the six world regions. It is important to consider that in Africa, pedestrian, cyclists, persons riding two- or three-wheeled vehicles and young men are the populations most at risk for RTA; however, little has been done to increase the space and safety for these group; in addition, the law supporting road traffic is insufficient and inadequate.
In our review, road traffic accidents in Africa obtained an estimated prevalence proportion of 61% (CI 95%, 53–69), the highest one. In terms of maxillofacial trauma, both studies included in the review [9, 39] reported only fractures. It should be considered that RTA in Africa is more expressive in adolescents than in children, once when children grow up and became more independent, the risk of injuries related to high-velocity events increases, especially when motorcycles and vehicles are used [9]. On the other hand, young children are more likely to be affected by falls and running over [39].
The second region with the highest RTA prevalence was Asia. The combined prevalence was 41% (CI 95%, 32–50). Similarly to Africa, this continent presented, according to WHO document: “Road Safety Status in the WHO South-East Asia Region,” the rate of 18.5 deaths per 100,000 inhabitants during 2010 [57]. On the other hand, Europe had the lowest prevalence of road accidents in this review, 26% (95% CI, 5–54). This result is not surprising, since this region showed a ratio with 9.3 deaths per 100,000 inhabitants due to traffic accidents [58]. This is true for some European regions, mainly in western countries. The European studies included in this review were conducted only on the western coast, so, it is possible that the number of children and adolescents victims of maxillofacial trauma due to road accidents is greater than the results presented here.
The “European Facts and Global Status Report on Road Safety 2015” of WHO explained some reasons why Europe achieved a reduction in road traffic injuries: “Laws and practices on key risk factors such as reduction of speed appropriate to road type, drinking-driving, use of seat belts, motorcycle helmets, and child restraints have reduced the risk of road traffic injuries” [58]. None of these factors can alone resolve the problem of road traffic accidents, but together they can change this reality in many other regions of the world.
A recent review of maxillofacial fractures in the last 30 years, including all age groups, concluded that RTA is the most important mechanism worldwide, mainly in Africa and Asia, which is in agreement with the present systematic review for the young population. On the other hand, North America, Brazil, and Europe have shown a tendency to decrease RTA, which is partially explained by the more severe traffic laws [27].
The results regarding the prevalence of maxillofacial trauma due to RTA presented considerable variation in some regions of the world, notably in Europe, North America, and South America. It must be considered that the study by Ferreira [51], a Portuguese study, had a great influence of the combined prevalence for the Europe region due to its high proportion (62%) compared with other European studies. However, this number is lower compared with the numbers in the past. Since 1994, Portugal Legislation has become compulsory the use of seat belts for the front passenger and the use of child restraints. After these measures to improve traffic safety, a decrease in the number of traffic accidents has been observed [51].
After road traffic accidents, the next most relevant etiology of maxillofacial trauma in children and adolescents corresponds to falls. It was observed that Europe and South America showed the same estimated proportion of 42%; however, the confidence interval was wider for Europe, which is explained by the influence of two studies [49, 51], which showed low prevalence of maxillofacial trauma due to falls.
Falls are an important cause of maxillofacial injuries in the first years of life when the child has a great uncertainty of motion and does not have good coordination [7]. In addition, school-aged children have low center of gravity, which can contribute to the lack of coordination [59], making them more susceptible to injuries. In the adolescent population, a decrease in the incidence of falls and an increase in the occurrence of other mechanisms such as fights and sports, as well as RTA can be observed [23]. According to the included studies, which showed etiology stratified for children and adolescents, a clear tendency of falls in childhood and increased incidence of RTA in adolescents can be observed. This is an important key to maxillofacial trauma prevention in children, mainly in schools, home, and playground, which is the most common places frequented by children. Parents or caregivers should be aware to avoid events or risks of falls during the first decade of life.
Violence was the third most important etiology of maxillofacial trauma in children and adolescents. Violence includes fights, assaults, weapons and firearms. The two world regions with the highest prevalence of violence are North America (19%; CI 95%, 4–41) and South America (12%; CI 95%, 5–20). In the USA, violence is considered an important cause of maxillofacial fractures in the overall population. Roden [60] pointed out this fact in a Level 1 Trauma Center study. According to the author, from 2005 to 2010, violence resulted by assaults was the second leading cause of facial fractures.
Children are less affected by community violence when compared with adolescents, but as they grow up and increase social interaction, they become more exposed to situations that could result in fights and other risk factors. Domestic violence is still a serious problem for children health. In Brazil, for years, children, women, and older adults were the groups that most suffered from domestic violence [61]. Unfortunately, studies do not report if violence events are related to family or community, once this information is not commonly used in the data bank of hospitals.
Sports events were the fourth mechanism of maxillofacial trauma among children and adolescents. Eight studies did not report the number of maxillofacial trauma due to sports. The highest prevalence of this mechanism was observed in the only multicenter study conducted by Boffano [7]. The prevalence was 27% (95% CI, 19–36). Other etiologies reported in studies were pooled on the category “others” and includes animal bites, domestic accident, play, and other.
One difficulty in the analyses of children and adolescents is the definition of the age group considered child or adolescent. Generally, based on pediatric area, a child is supposed to have 12 years or less, and an adolescent to have between 12 and 18 years. However, studies included in this review considered ages of 13, 15, 16, 17, and 18 years as the pediatric/children population. Therefore, it is essential to standardize the age groups in order to facilitate further study comparisons.
The male/female ratio among studies was not as high as can be observed for the adult population. It seems that in the pediatric population, differences between males and females are less evident than in adults, and so the distribution is more similar. Some African and Asian studies have already reported ratios, including adult population of 11.1:1 [62], 7.7:1 [63], 7.6:1 [64], 7.5:1 [65], and 4.9:1 [66] of cases of facial fractures. A review of Nigerian studies conducted by Adeyemo [67] revealed that in this country, the major cause of injuries in population is RTA and the male/female ratio was incredibly high in some studies (16.9:1 [15] and 24:1 [68]).
Only two studies reported data from more than one hospital [7, 24]. Obviously, the three studies that used National Data Banks are also from several hospitals. The use of more than one source of information is important to help with a better description of how trauma mechanisms are distributed among regions. The study of the etiology of maxillofacial trauma in children and adolescents is predominantly performed in hospitals based on medical records, which means the production of retrospective data. It is widely recognized in literature the limitations regarding secondary data.
A study performed by Boffano [7] used a prospective design, and the number of patients analyzed was not as great as in other studies included in this review, which is justifiable due to difficulties to perform longitudinal studies. It is evident that more prospective analyses about maxillofacial trauma in children and adolescents are needed. This could improve the quality of research information since data would be collected at the moment of hospital attendance by researchers involved.
Another fact is the great heterogeneity among studies, regardless of regions analyzed. Heterogeneity is not related to differences among methods, once their designs are very similar. Differences are possibly explained by disparities in the sample size. Therefore, a random model effect was used in order not to overestimate the final proportion. In this sense, the squares of each study on plots have the same size.
The quality assessment showed, in general, sufficient score according to NOS (adapted), which is compatible with the subjective analysis performed by each reviewer. After the discussion about the quality assessment, it was clear that the studies are not so different regarding their methodologies, which means that heterogeneity should be carefully interpreted.
Although our study is a unique contribution to literature, it has some limitations and biases. The most important biases include the difference in classifications of causes of injuries, as well as the victim’s age. Another limitation is related to the fact that only English language articles published from 2006 to 2015 were included.
Nonetheless, this study represents the first complete review of the maxillofacial trauma etiology among young people and summarizes the best literature evidence of the past 10 years. The proportion meta-analysis has proved to be a useful tool and allowed us estimating the proportion/prevalence of maxillofacial trauma resulting from different etiologies among children and adolescents.
The findings highlight the importance of public awareness regarding etiology and preventative measures for maxillofacial trauma around the word. Multicenter, prospective epidemiological studies should be conducted in order to make improvements in this field.
Conclusions
Based on the results of our review, it was concluded that:
-
1.
Similarly to the adult population, road traffic accidents represent a burden for the young population and remain for years as a challenge for public health;
-
2.
Special attention should be given to Africa and Asia, which presented the highest prevalence of road accidents;
-
3.
Falls are also a frequent cause of maxillofacial trauma, especially for schoolchildren;
-
4.
Violence, such as assaults, fights, weapons, and firearms was more evident in the Americas.
References
Kotecha S, Scannell J, Monaghan A, Williams RW (2008) A four year retrospective study of 1,062 patients presenting with maxillofacial emergencies at a specialist paediatric hospital. Br J Oral Maxillofac Surg 46:293–296. doi:10.1016/j.bjoms.2007.11.011
Meir JD, Tollefson TT (2010) Pediatric facial trauma. Curr Opin Otolaryngol Neck Surg 16:555–561. doi:10.1097/MOO.0b013e3283169321
Kidd AJ, Beattie TF, Campbell-Hewson G (2010) Facial injury pattern in a UK paediatric population aged under 13 years. Emerg Med J 27:603–606. doi:10.1136/emj.2009.075127
Morris C, Kushner GM, Tiwana PS (2012) Facial skeletal trauma in growing patient. Oral Maxillofac Surg Clin North Am 24:351–364. doi:10.1016/j.coms.2012.05.005
Bregagnolo LA, Bregagnolo JC, Silveira F, Bérgamo A, Santi LN, Watanabe MG (2013) Oral and maxillofacial trauma in Brazilian children and adolescents. Braz Dent J 24:397–401. doi:10.1590/0103-6440201302227
Yang RT, Li Z, Li ZB (2014) Maxillofacial injuries in infants and preschools: a 2.5-year study. J Craniofac Surg 25:964–967. doi:10.1097/SCS.0000000000000760
Boffano P, Roccia F, Zavattero E, Dediol E, Uglešić V, Kovačič Z et al (2015) European maxillofacial trauma (EURMAT) in children: a multicenter and prospective study. Oral Surg Oral Med Oral Pathol Oral Radiol 119:499–504. doi:10.1016/j.oooo.2014.12.012
Li Z, Li ZB (2008) Characteristic changes of pediatric maxillofacial fractures in China during the past 20 years. J Oral Maxillofac Surg 66:2239–2242. doi:10.1016/j.joms.2007.12.032
Ogunlewe MO, James O, Ladeinde AL, Adeyemo WL (2006) Pattern of paediatric maxillofacial fractures in Lagos, Nigeria. Int J Paediatr Dent 16:358–362. doi:10.1111/j.1365-263X.2006.00757.x
Karim T, Khan AH, Ahmed SS (2010) Trauma of facial skeleton in children: an Indian perspective. Indian J Surg 72:232–235. doi:10.1007/s12262-010-0056-x
Muñante-Cárdenas JL, Olate S, Aspirino L, de Albergaria Barbosa JR, de Moraes M, Moreira RW (2011) Pattern and treatment of facial trauma in pediatric and adolescent patients. J Craniofac Surg 22:1251–1255. doi:10.1097/SCS.0b013e31821c696c
Rottgers SA, Decesare G, Chao M, Smith DM, Cray JJ, Naran S et al (2011) Outcomes in pediatric facial fractures: early follow-up in 177 children and classification scheme. J Craniofac Surg 22:1260–1265. doi:10.1097/SCS.0b013e31821c6ab7
Vyas RM, Dickinson BP, Wasson KL, Roostaeian J, Bradley JP (2008) Pediatric facial fractures: current national incidence, distribution, and health care resource use. J Craniofac Surg 19:339–349. doi:10.1097/SCS.0b013e31814fb5e3
Kumaraswamy SV, Madan N, Keerthi R, Singh DS (2009) Pediatric injuries in maxillofacial trauma: a 5 year study. J Maxillofac Oral Surg 8:150–153. doi:10.1007/s12663-009-0037-4
Adekeye EO (1980a) The pattern of fractures of the facial skeleton in Kaduna, Nigeria: a survey of 1,447 cases. Oral Surg Oral Med Oral Pathol 49:491–495. doi:10.1016/0030-4220(80)90068-7
Brasileiro BF, Passeri LA (2006) Epidemiological analysis of maxillofacial fractures in Brazil: a 5-year prospective study. Oral Surg Oral Med Oral Pathol Oral Radiol 102:28–34. doi:10.1016/j.tripleo.2005.07.023
Haug RH, Foss J (2000) Maxillofacial injuries in the pediatric patient. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 90:126–134. doi:10.1067/moe.2000.107974
Hogg NJ, Stewart TC, Armstrong JE, Girotti MJ (2000) Epidemiology of maxillofacial injuries at trauma hospital in Ontario, Canada, between 1992 and 1997. J Trauma 49:425–432
Oji C (1998) Fractures of the facial skeleton in children: a survey of patients under the age of 11 years. J Craniomaxillofacial Surg 26:322–325. doi:10.1016/S1010-5182(98)80062-0
Ugboko VI, Odusanya SA, Fagade OO (1998) Maxillofacial fractures in a semi-urban Nigerian teaching hospital. Int J Oral Maxillofac Surg 27:286–289. doi:10.1016/S0901-5027(05)80616-2
Shaikh ZS, Worral SF (2002) Epidemiology of facial trauma in a sample of patients aged 1–18 years. Injury 33:669–671. doi:10.1016/S0020-1383(01)00201-7
Zimmerman CE, Troulis MJ, Kaban LB (2006) Pediatric facial fractures: recent advances in prevention, diagnosis and management. Int J Oral Maxillofac Surg 35:2–13. doi:10.1016/j.ijom.2005.09.014
Grunwaldt L, Smith DM, Zuckerbraun NS, Naran S, Rottgers SA, Bykowski M (2011) Pediatric facial fractures: demographics, injury patterns, and associated injuries in 772 consecutive patients. Plast Reconstr Surg 128:1263–1271. doi:10.1097/PRS.0b013e318230c8cf
Rahman RA, Ramali R, Rahman NA, Hussaini HM, Idrus SM, Hamid AL (2007) Maxillofacial trauma of pediatric patients in Malaysia: a retrospective study from 1999 to 2001 in three hospitals. Int Pediatr Otorhinolaryngol 71:929–936. doi:10.1016/j.ijporl.2007.03.003
Scariot R, de Oliveira IA, Passeri LA, Rebellato NL, Müller PR (2009) Maxillofacial injuries in a group of Brazilian subjects under 18 years of age. J Appl Oral Sci 17:195–198. doi:10.1590/S1678-77572009000300012
Weihsin H, Thadani S, Agrawal M, Tailor S, Sood R, Langalia A, Patel T (2014) Causes and incidence of maxillofacial injuries in India: 12-year retrospective study of 4437 patients in a tertiary hospital in Gujarat. Br J Oral Maxillofac Surg 52:693–696. doi:10.1016/j.bjoms.2014.07.003
Boffano P, Kommers SC, Karagozoglu KH, Forouzanfar T (2014) Aetiology of maxillofacial fractures: a review of published studies during the last 30 years. Br J Oral Maxillofac Surg 52:901–906. doi:10.1016/j.bjoms.2014.08.007
Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 6:1–6. doi:10.1371/journal.pmed.1000097
Higgins JP, Green S (2011) Cochrane Handbook for Systematic Reviews of Interventions version 5.1.0. The Cochrane Collaboration. http://handbook.cochrane.org/. Accessed 12 Feb 2015
Akobeng AK (2005) Principles of evidence based medicine. Arch Dis Child 90:837–840. doi:10.1136/adc.2005.071761
Boudin F, Nie JY, Bartlett JC, Grad R, Pluye P, Dawes M (2010) Combining classifiers for robust PICO element detection. BMC Med Inform Decis Mak 2010:10–29. doi:10.1186/1472-6947-10-29
Maia LC, Antonio AG (2012) Systematic reviews in dental research. A guideline. J Clin Pediatr Dent 37:117–124
Wells GA, Shea B, O’Connell D, Peterson J, Welch V, Losos M, Tugwell P (2011) The Newcastle-Ottawa (NOS) for assessing the quality of nonrandomized studies in meta-analyses. http://www.ohri.ca/programs/clinical_epidemiology. Accessed 2 Jan 2016
Hermont AP, Oliveira PA, Martins CC, Paiva SM, Pordeus IA, Aud SM (2014) Tooth erosion and eating disorders: a systematic review and meta-analysis. PLoS One 9:1–15. doi:10.1371/journal.pone.0111123
DerSimonian R, Laird N (1986) Meta-analysis in clinical trials. Control Clin Trials 7:177–188. doi:10.1016/0197-2456(86)90046-2
Freeman MF, Tukey JW (1950) Transformations related to the angular and square root. Ann Math Stat 21:607–611
Nyaga VN, Arbyn M, Aerts M (2014) Metaprop: a Stata command to perform meta-analysis of binomial data. Arch Public Health 72:39. doi:10.1186/2049-3258-72-39
Higgins JP, Thompson SG, Deeks JJ, Altman DG (2003) Measuring inconsistency in meta-analyses. BMJ 327:557–560. doi:10.1136/bmj.327.7414.557
van As AB, van Loghem AJ, Biermans BF, Douglas TS, Wieselthaler N, Naidoo S (2006) Causes and distribution of facial fractures in a group of South African children and the value of computed tomography in their assessment. Int J Oral Maxillofac Surg 35:903–906. doi:10.1016/j.ijom.2006.07.008
Arvind RJ, Narendar R, Kumar PD, Venkataraman S, Gokulanathan S (2013) Maxillofacial trauma in Tamil Nadu children and adolescents: a retrospective study. J Pharm Bioallied Sci 5:33–35. doi:10.4103/0975-7406.113290
Quing-Bin Z, Zhao-Qiang Z, Dan C, Yan Z (2013) Epidemiology of maxillofacial injury in children under 15 years of age in southern China. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 115:436–441. doi:10.1016/j.oooo.2012.04.026
Singhal R, Singh V, Bhagol A, Agrawal A, Kumar P (2013) Pediatric maxillofacial injuries—if a new look is required? Int J Pediatr Otorhinolaryngol 77:1333–1336. doi:10.1016/j.ijporl.2013.05.028
Ymamoto K, Matsusue Y, Horita S, Murakami K, Sugiura T, Kirita T (2013) Maxillofacial fractures in children. J Craniofac Surg 24:153–157. doi:10.1097/SCS.0b013e3182646506
Zhou HH, Ongodia D, Liu Q, Yang RT, Li ZB (2013) Incidence and pattern of maxillofacial fractures in children and adolescents: a 10 years retrospective cohort study. Int J Pediatr Otorhinolaryngol 77:494–498. doi:10.1016/j.ijporl.2012.12.017
Imahara SD, Hopper RA, Wang J, Rivara FP, Klein MP (2008) Patterns and outcomes of pediatric facial fractures in the United States: a survey of the National Trauma Data Bank. J Am Coll Surg 207:710–716. doi:10.1016/j.jamcollsurg.2008.06.333
Allareddy V, Itty A, Maiorini E, Lee MK, Rampa S, Allaredy V, Nalliah RP (2014) Emergency department visits with facial fractures among children and adolescents: an analysis of profile and predictors of causes of injuries. J Oral Maxillofac Surg 72:1756–1765. doi:10.1016/j.joms.2014.03.015
Hoppe IC, Kordahi AM, Paik AM, Lee ES, Granick MS (2014) Examination of life-threatening injuries in 431 pediatric facial fractures at a level 1 trauma center. J Craniofac Surg 25:1825–1828. doi:10.1097/SCS.0000000000001055
Soleimani T, Greathouse ST, Bell TM, Fernandez SI, O’Neil J, Flores RL (2015) Epidemiology and cause-specific outcomes of facial fracture in hospitalized children. J Craniomaxillofac Surg 43:1979–1985. doi:10.1016/j.jcms.2015.10.008
Thóren H, Iso-Kungas P, Lindgvist C, Törnwall J (2009) Changing trends in causes and patterns of facial fractures in children. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 107:318–324. doi:10.1016/j.tripleo.2008.09.024
Aren G, Sepet E, Pinar Erdem A, Tolgay CG, Kuru S, Ertekin C, Güloğlu R, Aren A (2013) Predominant causes and types of orofacial injury in children seen in the emergency department. Ulus Travma Acil Cerrahi Derg 19:246–250. doi:10.5505/tjtes.2013.75688
Ferreira PC, Barbosa J, Amarante JM, Carvalho J, Rodrigues AG, Silva ÁC (2015) Associated injuries in pediatric patients with facial fractures in Portugal: analysis of 1416 patients. J Craniomaxillofac Surg 43:437–443. doi:10.1016/j.jcms.2015.01.008
Chrcanovic BR, Abreu MH, Freire-Maia SLN (2010) Facial fractures in children and adolescents: a retrospective study of 3 years in a hospital in Belo Horizonte, Brazil. Dent Traumatol 26:262–270. doi:10.1111/j.1600-9657.2010.00887.x
Cavalcanti AL, Assis KM, Cavalcante JR, Xavier AF, Aguiar YP (2012) Maxillofacial traumatisms in children and adolescents in Campina Grande, Brazil. Brazilian Research in Pediatric Dentistry and Integrated Clinic 12:439–445. doi:10.4034/PBOCI.2012.123.22
Nardis Ada C, Costa SA, da Silva RA, Kaba SC (2013) Patterns of paediatric facial fractures in hospital of São Paulo, Brazil: a retrospective study of 3 years. J Craniomaxillofac Surg 41:226–229. doi:10.1016/j.jcms.2012.09.005
Collao-González C, Carrasco-Labra A, Sung-Hsieh HH, Cortés-Araya J (2014) Epidemiology of pediatric facial trauma in Chile: a retrospective study of 7,617 cases in 3 years. Med Oral Patol Oral Cir Bucal 19:99–105. doi:10.4317/medoral.19035
World Health Organization (2013a) Road safety in the WHO African region: the facts 2013. http://www.afro.who.int/. Accessed 2 Jan 2016
World Health Organization (2013b) Road safety status in the WHO South-East Asia region 2013. http://www.searo.who.int/. Accessed 3 Jan 2016
World Health Organization (2015) European facts and Global status report on road safety 2015. http://www.euro.who.int/. Accessed 7 Jan 2016
Santschi M, Echavé V, Laflamme S, McFadden N, Cyr C (2005) Seat-belt injuries in children involved in motor vehicle crashes. Can J Surg 48:373–376
Roden KS, Tong W, Surrusco M, Schockley WW, Aalst V, Hultman CS (2012) Changing characteristics of facial fractures treated at a regional, level 1 trauma center, from 2005 to 2010: an assessment of patient demographics, referral patterns, etiology of injury, anatomic location, and clinical outcomes. Ann Plast Surg 68:461–466. doi:10.1097/SAP.0b013e31823b69dd
Minayo MC (2007) The inclusion of violence in the health agenda: historical trajectory. Cien Saude Colet 11:375–383. doi:10.1590/S1413-81232006000200015
Al Ahmed HE, Jaber MA, Abu Fanas SH, Karas M (2004) The pattern of maxillofacial fractures in Sharjah, United Arab Emirates: a review of 230 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 98:166–170. doi:10.1016/S1079210404001039
Kamulegeya A, Lakor F, Kabenge K (2009) Oral maxillofacial fractures seen at a Ugandan tertiary hospital: a six-month prospective study. Clinics 64:843–848. doi:10.1590/S1807-59322009000900004
Fasola AO, Obiechina AE, Arotiba JT (2001) An audit of midfacial fractures in Ibadan, Nigeria. Afr J Med Med Sci 30:183–186
Olasoji HO, Tahir A, Bukar A (2002) Jaw fractures in Nigerian children: an analysis of 102 cases. Cent Afr J Med 48:109–112
Chandra Shekar BR, Reddy C (2008) A five-year retrospective statistical analysis of maxillofacial injuries in patients admitted and treated at two hospitals of Mysore city. Indian J Dent Res 19:304–308
Adeyemo WL, Ladeinde AL, Ogunlewe MO, James O (2005) Trends and characteristics of oral and maxillofacial injuries in Nigeria: a review of the literature. Head Face Med 1:1–9. doi:10.1186/1746-160X-1-7
Adekeye EO (1980b) Fractures of the zygomatic complex in Nigeria patients. J Oral Surg 38:596–599
Acknowledgements
The authors are grateful to the Fundação de Amparo à Pesquisa de Minas Gerais (FAPEMIG).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest statement
Author KGNB has received research grants from Fundação de Amparo à Pesquisa de Minas Gerais (FAPEMIG). The authors declare that they have no conflict of interest.
Role of the funding source
Research grants had no influence on study design, data collection and analysis, decision to publish, or manuscript preparation.
Ethical approval
Ethical approval does not apply for being a review article. Studies included were in accordance with the ethical research principles.
Informed consent
Informed consent does not apply for being a review article. Studies included were in accordance with the ethical research principles.
Rights and permissions
About this article

Cite this article
Barbosa, K.G.N., de Macedo Bernardino, Í., d’Avila, S. et al. Systematic review and meta-analysis to determine the proportion of maxillofacial trauma resulting from different etiologies among children and adolescents. Oral Maxillofac Surg 21, 131–145 (2017). https://doi.org/10.1007/s10006-017-0610-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10006-017-0610-9