
Abstract
Introduction
The goal of implant treatment is the formation of a direct bone–implant interface contact.
Purpose
This study aimed to evaluate the possibilities of immediate loading treatment for edentulous patients rehabilitated with mandibular and maxillary overdentures.
Material and methods
A literature review using the PubMed and BIREME databases between the periods of 1977 and 2011 was performed.
Results
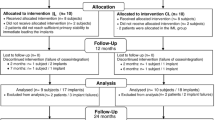
From an initial yield of 218 titles, 78 articles were selected for text analysis, finally resulting in 23 studies (16 prospective, 6 prospective randomized, and 1 prospective multicenter) that met the inclusion criteria.
Conclusion
The immediate loading protocol through which the implants are subjected to occlusal function immediately after their placement was introduced to overcome this limitation.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Since the first publications by Brånemark and colleagues [1], one of the most important paradigms, both for submerged and nonsubmerged implants, for adequate osseointegration of dental implants has been the absence of loading until osseointegration has occurred, with a waiting period ranging from 3 to 6 months [1, 2].
In recent years, an increasing interest toward shortening of time between implant placement and implant loading has been observed [2–25]. The immediate loading was introduced to reduce the bone healing waiting time [3]. This protocol is characterized by the placement of an interim fixed prosthesis after implant insertion.
The results of recent studies on early and immediate loading of implants supporting multiple-unit fixed restorations indicated that such loading protocol may also be successfully used with removable dentures [4, 5]. When the immediate loading protocol is used, it is suggested that splinting the implants immediately after placement may avoid micromotions that could have a negative impact on the osseointegration process [6].
This systematic review aimed to address the use of immediate loading overdentures (intervention) to rehabilitate edentulous patients (patients), taking into consideration the following aspects (comparisons): (1) maxillary and mandibular immediate loading and (2) implant survival, analyzing the results and making recommendations (outcomes), according to the population, intervention, comparisons, and outcomes (PICO) study design.
Materials and methods
A systematic literature search was conducted using the combined MeSH terms (“overdenture”) and (“immediate implant loading” or “implant-supported overdentures”) and (“clinical study” or “comparative study” or “outcome assessment” or “epidemiologic studies” or “intervention studies” or “patient satisfaction”) in the Medical Literature Analysis and Retrieval System Online databases between the periods 1977 and 2012. In vitro studies, case reports, and literature review studies were included. Non-English language articles and studies focusing on another type of oral rehabilitation were excluded.
The PICO format [26] was used to define a clear clinical question in comparative clinical studies involving completely edentulous patients (P) requiring immediate loading in overdentures (I), maxillary or mandibular overdenture (C), and success of immediate loading for rehabilitation of complete edentulous outcomes (O).
The search strategy was complemented by hand searching in the following peer-reviewed journals: International Journal of Oral & Maxillofacial Implants, Clinical Implant Dentistry and Related Research, Journal of Prosthetic Dentistry, Clinical Oral Implants Research, Clinical Oral Investigations, Journal of Oral Implantology, and The International Journal of Prosthodontics.
Results
From an initial yield of 218 titles, 78 articles were selected for text analysis, finally resulting in 23 studies (16 prospective, 6 prospective randomized, and 1 prospective multicenter) that met the inclusion criteria (Table 1).
Discussion
In 1997, a study [7] published a 10-year longitudinal study of 1,618 implants used to anchor complete dentures and an implant success rate of 76 and 99 % was found on the maxillae and mandible, respectively. Authors claimed that the osseointegration, term used to characterize the integration between implant and bone, is dependent on a two-stage surgical protocol. This protocol was developed to reduce the risk of infection, to avoid the mucosa growing toward implant apex, and to minimize the risks of early and unfavorable loads under the implant, reducing implant motion during the initial healing phase which could induce implant encapsulation by a fibrous tissue [1, 2].
Based on the biological and technological concepts from that time, the authors [1] recommended a healing period with occlusal load absence from 3 to 4 months for mandibular implants and from 5 to 6 months for maxillary implants.
The implant success is initially related to the surgical technique, primary stability, and absence of bacterial contamination on the implant [27]. The lack of mechanical trauma or overloads and peri-implantitis is also necessary [28]. The oral hygiene maintenance to remove bacterial plaque around the implant is required for the long-term success of implants [6]. Because of high success rate of dental implants, this treatment has become an accepted clinical reality [2, 4–25, 29–31].
Primary stability and absence of early loading of dental implants have been considered for years as a sine qua non condition to allow osseointegration of dental implants. The waiting time for osseointegration to occur is exhaustive and discomfort for the patient. However, the idea not to load early was empirically based and not experimentally ascertained. It is therefore justifiable to question whether this healing period is an absolute requirement to obtaining osseointegration or if, under certain circumstances, this period can be shortened without jeopardizing osseointegration and long-term results. In particular, it should be demonstrated whether or not any kind of movement transmitted to the implants during the early phases of integration can compromise the long-term results or if there is a threshold below which micromovements may not compromise osseointegration [1, 2].
Initial studies of immediate loading, with a primary goal of a direct bone–implant contact, have been proposed for overdentures in patients who are completely edentulous [2, 4–25]. These studies have shown encouraging results. In 1986, Babbush et al. [32] described a technique of immediately loading titanium plasma-sprayed implants placed in the mandibular symphysis with an overdenture. The implants were rigidly splinted with a metal bar, and the denture was relined with a soft liner within 2 to 3 days after the surgery. The final prosthesis with the clips was placed 2 weeks later. The authors reported a cumulative failure rate of 12 % after 8 years of follow-up. Since then, several studies have focused on both fixed and removable immediately loaded implant-supported prostheses in patients who are completely edentulous, and high success rates comparable with conventionally loaded implants have been reported (Table 1) [2, 4–25]. The success rates of subperiosteal dental implants have been disputed [33]. Minimal documented evidence of the predictability of these devices has lessened the benefits that the implant offers for patients with severely atrophic mandibles [34, 35].
Although there is a lack of consensus on the definition of loading, some authors refer to immediate loading when the period of time between implant placement and prosthesis insertion is less than 48 h. However, delayed loading consists of loading an implant-supported prosthesis after a healing period ranging from 3 to 6 months [36, 37].
In the protocol of one-surgical stage, primary stability is an essential prerequisite for early loading. Some factors affect the implant’s primary stability, including bone density, implant design, surgical technique, insertion torque, and instrumentation protocol. Among these parameters, the insertion torque has not been fully analyzed yet. The insertion torque value depends on the implant’s surface, design, and screw thread geometry [38].
The measurement of implant stability can be performed by using resonance frequency technique [39]. The values of resonance frequency are related to the implant stability into the bone [40]. Sennerby and Meredith [41] used the resonance frequency to investigate the implant stability in the anterior region of the mandible, and no change on implant stability values were observed within the 3 months of healing period. This result confirms the idea of using immediate loading in mandibular implants. However, in the presence of poor quality and quantity bone and overloads, implants subjected to immediate loading may be at risk of failure [23].
Some indicate that thresholds between 25 and 45 Ncm of insertion torque are necessary to prevent critical implant micromovements [42]. Others found that values above 32 Ncm would be an indication of primary stability [38].
The necessity of splinting the implants is a questionable factor in overdenture rehabilitation. Some authors stated that the use of splinted implants after surgery is a prerequisite to obtain success in immediate loading overdentures [2, 43]. The use of bar to splint the implants is an effective method to avoid axial rotation and micromovement of immediately loaded implants and, consequently, loss of osseointegration [44, 45]. However, the effectiveness of splinting immediate loading implants to keep the osseointegration should be revised [46] since some studies have demonstrated that nonsplinting implants subjected to immediate loading can be osseointegrated [47, 48].
According to Goiato et al. [38] and Ochiai et al. [49], the splinting of implants by using a bar created greater stress on the implants and supporting tissues when compared to unsplinted implants (i.e., o-ring system). Although the use of o-ring attachment system reduced the stress concentration on the peri-implant bone tissue, the use of other types of attachments systems is not unfeasible.
We believe that in case of immediate loading of overdentures, it is important to reduce the stress on the peri-implant region to achieve primary stability. Therefore, the use of o-ring system is more indicated, owing to its lower stress distribution to the implant region.
In order to reduce the cost of overdenture treatment, the use of one implant to retain mandibular complete dentures provided adequate function to the patient, even in the case of immediate loading implants [18, 19, 25]. Regarding maxillary overdentures, further studies are required [4]. In the maxilla, the bone height, bone quality, and presence of anatomic structures such as maxillary sinus and nasal cavity should be observed during implant insertion. Different from the manbibular bone, the maxillary bone presents a thinner cortical bone and a less dense trabecular bone which induces lower primary stability of implants placed on the maxilla. The clinical success of immediate loading of superior overdentures depends on the implant placement region and implant length. The decision about immediate loading of maxillary overdentures should be carefully evaluated [4, 16, 19, 47] since longitudinal clinical studies on this issue are limited.
The use of immediate loading overdentures over two lower implants should become the treatment of choice for individuals who have a fully edentulous mandible [5, 6, 9–11, 13, 15–18, 20–23]. The resonance frequency of the initial and late stability of implants used to retain the overdenture under immediate loading is an alternative for obtaining retention and stability in treatments involving conventional complete dentures, where two implants are enough to retain the overdenture satisfactorily [5, 6, 9–11, 13, 15–18, 20–23].
According to the present study, the use of immediate loading implants to retain overdentures is a predictable treatment option, even in the case of single implants when its splinting is not possible. Nevertheless, there is no doubt about the necessity of good quality and quantity bone to provide enough primary stability of the implant, resulting in a high level of implant insertion torque so that the abutments are placed with a lower torque than the insertion torque of the implant. In patients with good periodontal health, who have no infections at the implant site as well as balanced occlusion, and who have nonparafunctional habits, a predictable planning treatment can be designed based on radiographs, computed tomography scan, and surgical guides.
Conclusion
According to the review, it was concluded that the success of immediate loading for rehabilitation of complete edentulous arches with overdentures has increased. In general, the studies have demonstrated high predictability for rehabilitation of mandibular complete edentulous arches with immediate loading overdentures, mainly when the implants are placed in the symphysis area regardless of implant number. The maxillary rehabilitation with immediately loaded overdentures is questionable due to lack of longitudinal studies in literature.
References
Brånemark PI, Hansson BO, Adell R et al (1977) Osseointegrated implants in the treatment of the edentulous jaw. Experience from a 10-year period. Scand J Plast Reconstr Surg 16:1–132
Chipasco M, Gatti C (2003) Implant-retained mandibular overdentures with immediate loading: a 3- to 8-year prospective study on 328 implants. Clin Implant Dent Relat Res 5:29–38
Kammeyer G, Proussaefs P, Lozada J (2002) Conversion of a complete denture to a provisional implant-supported, screw-retained fixed prosthesis for immediate loading of a completely edentulous arch. J Prosthet Dent 87:473–476
Jemt T, Chai J, Harnett J et al (1996) A 5-year prospective multicenter follow-up report on overdentures supported by osseointegrated implants. Int J Oral Maxillofac Implants 11:291–298
Roynesdal AK, Amundrud B, Hannaes HR (2001) A comparative clinical investigation of 2 early loaded ITI dental implants supporting an overdenture in the mandible. Int J Oral Maxillofac Implants 16:246–251
Payne AG, Tawse-Smith A, Duncan WD et al (2002) Conventional and early loading of unsplinted ITI implants supporting mandibular overdentures. Clin Oral Implants Res 13:603–609
Romeo E, Chiapasco M, Lazza A et al (2002) Implant-retained mandibular overdentures with ITI implants. Clin Oral Implants Res 13:495–501
Rungcharassaeng K, Lozada JL, Kan JYK, Kim JS, Campagni WV, Munoz CA (2002) Peri-implant tissue response of immediately loaded, threaded, HA-coated implants: 1-year results. J Prosthet Dent 7:173–181
Tawse-Smith A, Payne AG, Kumara R, Thomson WM (2002) Early loading of unsplinted implants supporting mandibular overdentures using a one-stage operative procedure with two different implant systems: a 2-year report. Clin Implant Dent Relat Res 4:33–42
Stricker A, Gutwald R, Schmelzeisen R, Gellrich NG (2004) Immediate loading of 2 interforaminal dental implants supporting an overdenture: clinical and radiographic results after 24 months. Int J Oral Maxillofac Implants 19:868–872
Turkyilmaz I, Tözüm TF, Tumer C, Ozbek EN (2006) A 2-year clinical report of patients treated with two loading protocols for mandibular overdentures: early versus conventional loading. J Periodontol 77(12):1998–2004
Assad AS, Hassan SA, Shawky YM, Badawy MM (2007) Clinical and radiographic evaluation of implant-retained mandibular overdentures with immediate loading. Implant Dent 16:212–223
de Smet E, Duyck J, Sloten J, Jacobs R, Naert I (2007) Timing of loading—immediate, early, or delayed—in the outcome of implants in the edentulous mandible: a prospective clinical trial. Int J Oral Maxillofac Implants 22:580–594
Stephan G, Vidot F, Noharet R, Mariani P (2007) Implant-retained mandibular overdentures: a comparative pilot study of immediate loading versus delayed loading after two years. J Prosthet Dent 97:138S–145S
Turkyilmaz I, Tumer C (2007) Early versus late loading of unsplinted TiUnite surface implants supporting mandibular overdentures: a 2-year report from a prospective study. J Oral Rehabil 34:773–780
Alfadda SA, Attard NJ, David LA (2009) Five-year clinical results of immediately loaded dental implants using mandibular overdentures. Int J Prosthodont 22(4):368–373
Attard NJ, Diacono M (2010) Early loading of fixture original implants with mandibular overdentures—a preliminary report on a prospective study. Int J Prosthodont 23(6):507–512
Kronstrom M, Davis B, Loney R, Gerrow J, Hollender L (2010) A prospective randomized study on the immediate loading of mandibular overdentures supported by one or two implants: a 12-month follow-up report. Int J Oral Maxillofac Implants 25(1):181–188
Liddelow GJ, Henry PJ (2010) The immediately loaded single implant-retained mandibular overdenture: a 36-month prospective study. Int J Prosthodont 23(1):13–21
Roe P, Kan JY, Rungcharassaeng K, Lozada JL (2011) Immediate loading of unsplinted implants in the anterior mandible for overdentures: 3-year results. Int J Oral Maxillofac Implants 26(6):1296–1302
da Silva RJ, Semprini M, da Silva CH, Siéssere S, Chimello DT, Bataglion C, Savaris C, Regalo SC (2012) Resonance frequency analysis of overdenture retainer implants with immediate loading. Gerodontology 29:e408–e412
Büttel AE, Gratwohl DA, Sendi P, Marinello CP (2012) Immediate loading of two unsplinted mandibular implants in edentulous patients with an implant-retained overdenture: an observational study over two years. Schweiz Monatsschr Zahnmed 122(5):392–397
Gadallah AA, Youssef HG, Shawky YM (2012) A comparative study between early occlusal loading at 1 and 6 weeks in implant-retained mandibular overdentures. Implant Dent 21(3):242–247
Mangano C, Mangano FG, Shibli JA, Ricci M, Perrotti V, d’Avila S, Piattelli A (2012) Immediate loading of mandibular overdentures supported by unsplinted direct laser metal-forming implants: results from a 1-year prospective study. J Periodontol 83(1):70–78
El-Sheikh AM, Shihabuddin OF, Ghoraba SM (2012) A prospective study of early loaded single implant-retained mandibular overdentures: preliminary one-year results. Int J Dent 2012:236409
Needleman IG (2002) A guide to systematic reviews. J Clin Periodontol 29:6–9
Ntounis A, Petropoulou A (2010) A technique for managing and accurate registration of periimplant soft tissues. J Prosthet Dent 104:276–279
Maltz D, Rosenberg ES (1991) Implant overdentures—a simple solution. Compendium 12:820, 822, 824–826
Goodacre CJ, Kan JY, Rungcharassaeng K (1999) Clinical complications of osseointegrated implants. J Prosthet Dent 81:537–552
Becker W, Becker BE, Hujoel P (2000) Retrospective case series analysis of the factors determining immediate implant placement. Compend Contin Educ Dent 21:805–808, 810–811, 814
Cehreli MC, Akça K (2004) Narrow-diameter implants as terminal support for occlusal three-unit FPDs: a biomechanical analysis. Int J Periodontics Restorative Dent 24:513–519
Babbush CA (1986) Titanium plasma spray screw implant system for reconstruction of the edentulous mandible. Dent Clin North Am 30:117–130
James RA (1983) Subperiostal implant design based on peri-implant tissue behavior. NYJD 53:407–413
Minichetti JC (2003) Analysis of HA-coated subperiosteal implants. J Oral Implantol 3:111–116
James RA, Lozada JL, Truitt PH et al (1988) Subperiosteal implants. J Calif Dent Assoc 16:10–14
Ganeles J, Wismeijer D (2004) Early and immediately restored and loaded dental implant for single-tooth and partial-arch applications. Int J Oral Maxillofac Implants 19:92–102
Bogaerde LV, Pedretti G, Dellacassa P et al (2003) Early function of splinted implants in maxillas and posterior mandibles using Brånemark system machined-surface implants: an 18-month prospective clinical multicenter study. Clin Implan Dent Relat Res 5:21–28
Goiato MC, Pellizzer EP, dos Santos DM et al (2009) Clinical viability of immediate loading of dental implants: part I—factors for success. J Craniofac Surg 20:2139–2142
Meredith N, Cawley P, Alleyne D (1994) The application of modal vibration analysis to study bone healing in vivo. J Dent Res 73:793
Meredith N, Book K, Friberg B et al (1997) Resonance frequency measuraments of implants stability in vivo: a cross-sectional and longitudinal study of resonance frequency measuraments on implant in edentulous and partially dentate maxilla. Clin Oral Implants Res 8:226–233
Sennerby L, Meredith N (1998) Resonance frequency analysis: measuring implant stability and osseointegration. Compendium 19:493–504
Neugebauer J, Weinländer M, Lekovic V et al (2009) Mechanical stability of immediately loaded implants with various surfaces and designs: a pilot study in dogs. Int J Oral Maxillofac Implants 24:1083–1092
Lozada JL, Tsukamoto N, Farnos A, Kan J, Rungcharassaeng K (2000) Scientific rationale for the surgical and prosthodontic protocol for immediately loaded root form implants in the completely edentulous patient. J Oral Implantol 26:51–58
Molly L (2006) Bone density and primary stability in implant therapy. Clin Oral Implants Res 17:125–135
Del Fabbro M, Testori T, Francetti L et al (2006) Systematic review of survival rates for immediately loaded dental implants. Int J Periodontics Restorative Dent 26:249–263
Schnitman PA (1997) Ten-year results for Brånemark implants immediately loaded with fixed prostheses at implant placement. Int I Oral Maxillofac Implants 12:495–503
Glauser R, Rée A, Lundgren A, Gottlow J et al (2001) Immediate occlusal loading of Brånemark implants applied in various jawbone regions: a prospective, 1-year clinical study. Clin Implant Dent Relat Res 3:204–213
Calvo MP, Muller E, Garg AK (2000) Immediate loading of titanium hexed screw-type implants in the edentulous patient: case report. Implant Dent 9:351–357
Ochiai KT, Williams BH, Hojo S et al (2004) Photoelastic analysis of the effect of palatal support on various implant-supported overdenture designs. J Prosthet Dent 91:421–427
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Goiato, M.C., Bannwart, L.C., Pesqueira, A.A. et al. Immediate loading of overdentures: systematic review. Oral Maxillofac Surg 18, 259–264 (2014). https://doi.org/10.1007/s10006-013-0421-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10006-013-0421-6