
Abstract
Cognitive models of social anxiety [Clark and Wells, Social phobia: Diagnosis, assessment, and treatment, Guilford Press, New York, 1995], diagnostic criteria and studies on adult samples suggest that both an overestimation of bodily anxiety symptoms and psychophysiological abnormalities play an important role in social anxiety. To date, less is known about such a perception bias and physiological characteristics in children and adolescents with social anxiety. We performed a systematic review of the literature in the electronic databases Medline, PsycINFO, and PSYNDEX. Additional studies were identified by hand search using the ancestry approach. We identified 1,461 studies, screened their titles and abstracts, viewed 94 papers, and included 28 of these. Study samples were heterogeneous and consisted of socially phobic, high socially anxious, shy and test anxious children and adolescents. Regarding a biased perception, most studies in the review suggest that bodily symptoms of anxiety were overestimated by children and adolescents across the social anxiety spectrum when compared with control groups. An elevated psychophysiological reactivity to social stress was present in samples of high social anxiety, shyness, and test anxiety. In clinical samples with social phobia, by contrast, no differences or an even lower physiological responding compared with healthy control groups were reported. In addition, some evidence for a chronic psychophysiological hyperarousal was found across all sample types. The results are discussed with regard to current models of social anxiety, psychophysiological theories, and treatment implications.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Anxiety disorders in children and adolescents are among the most prevalent psychiatric disorders; in this age group, between 10 and 20 % of youths are affected by anxiety symptoms that require treatment [2, 3]. Further, high anxiety in children often leads to a significant impairment in daily life and poses a high risk to a normal social-emotional development during childhood and youth [4, 5]. The most common anxiety disorder in children and adolescents is social phobia (SP) with lifetime prevalence rates of up to 12.1 % [6]. In the Diagnostic Statistical Manual of Mental Disorders (DSM-IV [7],Footnote 1 SP is defined as an excessive, irrational fear of social or performance situations due to the expectation that others will scrutinize the person’s actions. The average age of onset for high social anxiety and SP is early to mid-adolescence [8, 9], but SP occurs even in children as young as 8 years [10]. Thus, important developmental steps can be compromised, leading to negative lifelong trajectories. Due to the early onset of SP, the investigation of samples of socially anxious children or adolescents is of particular interest to understand how this disorder develops and aggravates over time.
Focus and structure of the current review
For the understanding of social anxiety and SP, physiological arousal and bodily anxiety symptoms are of particular interest. Cognitive models of clinical social anxiety (e.g. Clark and Wells [1]) assume that bodily anxiety symptoms—in particular their biased perception and misinterpretation—are involved in the maintenance of social anxiety. Results from studies on adults support the importance of bodily anxiety symptoms in social anxiety, especially their overestimation (e.g. [11–16]). Further, a bodily hyperarousal in social situations is also part of the diagnostic criteria for SP. According to the DSM-IV, individuals with SP frequently experience physiological symptoms of anxiety such as sweating and palpitations in feared social or performance situations [7]. The International Classification of Diseases (ICD-10 [17]) requires an abnormal physiological reactivity (e.g. blushing or sweating) to social situations for a diagnosis of the disorder. Importantly, the above-mentioned physiological and perceptional processes underlie strong developmental influences during childhood and youth [18–22]. Thus, results from studies on adults with high social anxiety may not be valid for younger populations and a look on investigations that focus on children and adolescents is indicated. To our knowledge, no systematic review or meta-analysis investigating bodily anxiety symptoms and their perception in socially anxious children and adolescents has been published so far. One recent systematic review covered the related topic of pharmacological challenge in childhood panic and social anxiety but did not include response to social stress, perception of bodily symptoms, or autonomic functioning [23].Footnote 2 Other reviews regarding bodily anxiety symptoms in social anxiety only focus on the adult literature (e.g. [14]).
Hence, this review addresses the two lead questions: First, do socially anxious children and adolescents overestimate bodily symptoms, as suggested by the results from adult literature? In response to this question, we mainly review studies using self-report data. Second, are socially anxious children and adolescents characterized by objectively measurable physiological abnormalities? This second questions qualifies the first one in that subjective perception could only be considered as biased if no corresponding physiological alteration would be observed. Reviewed studies included measures of the autonomic nervous system and the neuroendocrine system. Before investigating these two questions, we briefly introduce the key theoretical models of social anxiety as well as associated subclinical manifestations and associated empirical findings. We also briefly introduce autonomic and endocrine measures.
Forms of social anxiety
Beside the investigation of clinical SP samples, a common approach is the study of extreme groups of children and adolescents with a broad spectrum of both clinical social anxiety (SP) and non-clinical social anxiety (high social anxiety, test anxiety, or shyness). These different types of social anxiety are characterized by correlating symptoms and by the core symptom of social anxiety: the fear of negative evaluation by others [27, 28]. This has led some researchers to view different forms of social anxiety as points on a severity continuum (see also the social anxiety continuum [27, 28]. While one extreme of the continuum marks subclinical types of shyness and high social anxiety, the other extreme marks clinical SP. The further the continuum extends, the stronger is the severity of symptoms and the impairments that are caused by them in daily life. As a consequence, the study of samples of children with a broad spectrum of social anxiety may help to understand how social anxiety develops and what factors are involved in its aggravation over time [29]. Beside symptom severity, social anxiety can also be differentiated by its generalization across situations, or put differently, by the number of situations during which social fears manifest. For example in the DSM-IV, SP can be classified as either specific SP or generalized SP, depending on if symptoms are present in only one special type of situation (e.g. social speaking) or in almost all social situations (e.g. social interactions with peers and social performance situations). On the background of the ongoing debate whether different subtypes of social anxiety are qualitatively different or merely different points on a severity/generality continuum we opted to widen our review to include studies not only of clinical SP, but also of subclinical shyness, high social anxiety, and test anxiety. Hence, beside children and adolescents with generalized and simple SP, we also focus on samples with other forms of social anxiety such as test anxiety, shyness, or high social anxiety.
Research question 1: The subjective side—does a biased attention for bodily symptoms of anxiety exist in socially anxious children and adolescents?
Physiological symptoms of anxiety play a prominent role in cognitive models of adult SP (e.g. [1, 30]). The attention to—and misinterpretation of—internal physiological arousal has been identified as one key maintenance factor: when entering a social situation, socially anxious individuals are assumed to be concerned about the visibility of bodily anxiety symptoms (blushing, sweating, trembling) because they interpret such visibility as a failure (e.g. “If others see how much I blush, I embarrass myself”). As a consequence, socially anxious individuals focus their attention on their bodily responses, thereby elevating awareness and perceived strength of such responses. Perception of strong bodily anxiety symptoms, in turn, further amplifies the current fear about symptom visibility and thereby anxiety level. To make this worse, cognitive capacities bound by inward attention reduce the resources remaining for an adequate coping with the current social situation. Possibly due to these mechanisms, socially anxious individuals are sometimes perceived as less friendly and responsive by others, making social rejection more likely [1]. In adult samples, strong empirical evidence indeed points to the existence of a perception bias for physiological arousal in both clinical and subclinical social anxiety (e.g. [11–16]).
When does such biased perception of bodily symptoms develop? Clearly, a prerequisite for this symptom is the development of a general concept of bodily arousal and its visibility. Developmental studies indicate that interoceptive processes during childhood and adolescence may differ from those found in adult populations and previous research suggests that emotional reasoning—the ability to make inferences from bodily sensations and to link them to specific emotions—is limited and still under development during youth [22, 31]. Testing this question in a community sample of children aged 8 to 12 years, with varying levels of trait anxiety, Muris et al. [22] found that children did make use of information about bodily arousal in rating the degree of dangerousness of several written social scenarios. However, contrary to results from adult samples (e.g. [32]), children with high trait anxiety did not differ from a low anxiety group in their use of bodily information (e.g. racing heart) for the evaluation of the level of script danger when objective information about situational danger was present. Hence, anxious children may associate bodily anxiety symptoms less closely with the evaluation of situational danger than adults. Since trait anxiety must not be equated with social anxiety, this study illustrates the need for age-specific investigations in social anxiety.
Research question 2: The objective side—Autonomic and endocrine system and their alteration in social anxiety
As pointed out above, diagnostic criteria for clinical social anxiety include a physiological hyperreactivity to social stress in these individuals. Both ICD-10 and DSM-IV describe that to fulfill the diagnosis of SP patients must show an abnormal physiological reactivity (e.g. blushing or sweating) to social stress. In addition to these diagnostic criteria, cognitive models of social anxiety likewise assume an actual physiological hyperreactivity to social stress. For example, the prominent cognitive model of SP by Clark and Wells [1] postulates that beside a subjective perception bias for bodily anxiety symptoms, socially anxious individuals may also experience an actual rise in physiological arousal, which may lead to blushing or sweating during social stress.
In the context of social-evaluative stress and anxiety, two physiological systems regulate the organism’s coping reaction: the hypothalamus–pituitary–adrenal system (HPA-axis) with its end product cortisol and the autonomic nervous system (ANS). Particularly in more enduring stress situations, the hypothalamic production of corticotropinreleasing hormone (CRH) rises, which stimulates the pituitary release of adrenocorticotropin hormone (ACTH) and, as a consequence, cortisol is secreted into the bloodstream by the adrenal cortex [33]. This steroid hormone enables the body to adjust to threatening situations and provides energy for bodily reactions: Cortisol influences metabolic processes and has anti-inflammatory and immunosuppressive effects [34]. But the HPA-axis is active during resting conditions, too, and follows a circadian rhythm. Cortisol can be assessed in the saliva and is, therefore, a popular non-invasive index of HPA-axis activity.
In contrast to the rather slow response of the HPA-axis, the ANS allows for fast and flexible adaptation of a large number of effector organs (e.g. heart, blood vessels, sweat palms) to stress. Common indicators of ANS activity are heart rate (HR), blood pressure, skin conductance level (SCL), and other parameters (for an overview of ANS parameters see Kreibig [35]). The ANS comprises a sympathetic and a parasympathetic branch, which are often antagonistic in their interaction of dually innervated organs (e.g. the heart) but can also operate in different modes of reciprocal, coupled, or uncoupled activation [36]. Generally spoken, while an activation of the sympathetic nervous systems leads to an increase in physiological arousal (e.g. increase of HR), the activation of the parasympathetic part leads to physiological inhibition (e.g. decrease of HR). When facing an anxiety provoking situation, the ANS ideally enables the organism for a swift physiological coping through an increase in sympathetic/decrease in parasympathetic control. After a stressful event, the ANS quickly returns to an energy efficient state (sympathetic decrease/increased parasympathetic inhibition), thereby preserving the organism’s long-term homeostasis [37]. There are also several reciprocal neural connections between superior structures of the HPA-axis and the ANS which regulate the interaction of these systems in short-term and long-term stress reactions. Excitatory and inhibitory neural pathways, like serotonin or opioid peptides, regulate the two systems simultaneously [33].
Numerous studies have assessed objective parameters of psychophysiological responding to social stress in SP adult samples, however, without yielding a coherent picture. While one group of studies found higher levels of HR before and during stress [16, 38], increased sympathetic and parasympathetic responding to social situations in female SPs or diagnostic subgroups [13, 39], in other studies autonomic parameters did not differ between SPs and healthy controls [12, 40]. Studies on endocrine abnormalities in SP adults have yielded similar inconsistent results [41, 42]. Thus, from these studies, to date it remains mostly unclear to what extent SP adults may differ from non-anxious individuals in their autonomic and endocrine responses.
Similar to cognitive and perceptional processes, developmental factors must be taken into account when investigating autonomic and endocrine characteristics of childhood psychopathology. For example, empirical evidence points to an altered stress-related HPA- axis functioning with age: A study by Gotthardt et al. [18] showed larger cortisol stress responses in older subjects, and a study by Kudielka et al. [19] reported positive correlations between cortisol baseline levels and age which might be a sign for a higher basal HPA-axis activation with advanced age. Further, some authors argue that the resilience of HPA-axis functioning declines with age as older people seem to show higher cortisol responses to stimulation and a prolonged recovery after stress [43]. Furthermore, the circadian rhythm appears to advance with age and diurnal amplitudes seem to flatten [44, 45]. Regarding the ANS, studies have found evidence that cardiovagal autonomic control, which is the central integration of afferent inputs and generation of efferent vagal outflow [46], declines with age in adult subjects. A study by Lenard et al. [20] found that from infancy to young adulthood, cardiovagal autonomic function appears to improve—with a peak level in adolescence, which could be a result of maturation of neural mechanisms. The authors investigated four age groups of healthy subjects, ranging from 7 to 10 years, from 11 to 14 years, from 15 to 18 years, and from 19 to 22 years. From group 1 to 3, the efficiency of central integrative mechanisms more than doubled. Thus, the increased efficiency of neural integrative mechanisms seems to compensate the stiffening of the carotid artery, and the ANS becomes more efficient throughout adolescence.
With these aspects in mind we will outline our search strategy and investigate the literature with particular focus on subjective and objective markers of bodily sensation in relation to social anxiety in children and adolescence.
Method
Search strategy
Studies were collected through a systematic computer-based literature search in the electronic databases Medline, PsycINFO, and PSYNDEX. Search terms can be seen in Table 1.
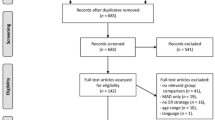
Additionally, a hand search was conducted using the ancestry approach [47]: references of the identified articles were scanned for additional studies meeting inclusion criteria (see below). Procedure and results are depicted in Fig. 1. Data search and data extraction were performed by the first and the last author, respectively.

Process and results of the literature search
Inclusion criteria
Only published peer-reviewed original journal articles in English about physiological aspects of socially anxious children and adolescents from the age of 6 to 18 years were included since SP typically has its onset in middle childhood [9]. Participants in the included studies were either diagnosed with SP according to DSM criteria or selected for high social anxiety, high shyness, or test anxiety using standardized measures.Footnote 3 In the included studies, various parameters were assessed for sympathetic and parasympathetic arousal.
Results
Included studies
In this review, 28 studies were included: 9 studies investigating SP samples, 6 studies investigating samples with test anxiety, and 13 studies investigating samples with high social anxiety or high shyness. The publication dates of the studies ranged from 1967 to 2012, with 80 % of the studies published between 1990 and 2012. The textually reviewed but still excluded studies (66) did not meet inclusion criteria in various ways. Many of these studies (49) did not focus on social anxiety—for example, in these studies, children and adolescents with internalizing symptoms or different anxiety disorders were examined with regard to physiological aspects, but studies did not report results specifically for social anxiety. Other studies (6) did only use self-report measures for the measurement of bodily symptoms. Some other studies (11) were theoretical works or non-published dissertations. Due to the lack of comparable data, we did not conduct a formal meta-analysis but summarized studies qualitatively. Table 2 shows the corresponding details on sample, sample size, age range, design, and the main results. For significant effects involving group, we calculated standardized effect sizes according to Cohen [50]. For studies with a correlational design, Pearson’s r was reported.Footnote 4
Discussion
Research question 1: Biased perception of bodily anxiety symptoms
We identified seven studies that investigated both subjective experience of physiological arousal and objective physiological arousal (measured by instruments or by observer ratings). All seven studies found that socially anxious children and adolescents overestimated their bodily symptoms of anxiety when compared with non-anxious controls during social-evaluative stress, while no actual group differences in physiological arousal were found (e.g. [51, 60, 71, 75]). The consistency of this result was striking: a biased perception (overestimation) was found in studies across the whole social anxiety spectrum including SP, test anxiety, high social anxiety and high shyness (e.g. [51, 60, 71, 75]). Effect sizes, if reported, ranged from medium to large effects (f = 0.30 to f = 0.99).
For example, in a study by Anderson et al. [51], SP adolescents, who had to give a speech and engage in a conversation with an unfamiliar person, reported higher subjective arousal than healthy controls during the anxiety-provoking tasks, but no group differences in HR or blood pressure emerged. Further, such biased perception seems to manifest early in social anxiety and possibly prior to the onset of fully blown SP: In a study by Miers et al. [71], high socially anxious children and adolescents aged 9–17 reported a higher HR and sweatier palms than low socially anxious children in a speech task in the absence of actual group differences in HR or SCL. Since social fears were not formally assessed by a clinical interview, it remains unclear how many children in this study fulfilled the SP diagnosis. Interestingly, socially anxious children not only to overestimated their bodily arousal, but also took an outside perspective on their appearance and worried more than their non-anxious peers about symptom visibility to others [75], which is a central claim of the Clark and Wells model [1]. Accordingly, the exaggerated perception of bodily arousal may result from a heightened self-monitoring and the extensive worry that others might notice how anxious one is. Importantly, biased symptom perception and worry about visibility are separable aspects. We have previously reported that group differences in biased symptom perceptions between SP children and controls were reduced when statistically controlling for group differences in worry about their visibility [75].
Generally, these findings of consistently overestimated bodily symptoms are in keeping with the general idea that Clark and Wells’ [1] theoretical model of SP might be applicable to children and youth. With regard to subjective indicators, the bulk of findings reviewed so far support the assumption that an overestimation of bodily symptoms is already present in socially anxious children and adolescents—and thus mirror the adult literature (e.g. [11–16]) despite differences in cognitive-emotional development. As such it is likely that this factor is involved in the development and maintenance of social fears. However, there is also evidence that points to potential differences between socially anxious children and adults. For example, contrary to findings in samples of SP adults, high socially anxious children did not feel more anxious when a bogus HR feedback was made public to unknown observers as reported by Schmitz et al. [75]. This is also inconsistent with the cognitive model by Clark and Wells [1], which assumes that the visibility of a bodily anxiety symptom causes increased anxiety because it could lead to negative evaluation by others. Possibly, developmental differences account for this inconsistency. As mentioned above, a study by Muris, Merckelbach, and van Spauwen [22] suggested that children, as opposed to adults, may focus mainly on the most salient information when judging dangerous situations. As the ability for emotional reasoning is still developing during childhood [31], interoceptive information, like HR feedback, could be less relevant for children than for adults.
Research question 2: less anxiety severity is associated with heightened autonomic and endocrine responding
We identified 26 studies that assessed autonomic and endocrine abnormalities in children and adolescents with social anxiety. In clinical samples with the diagnosis of SP, most studies failed to find an autonomic or endocrine hyperreactivity to social-evaluative stress. For example, in a study by Anderson et al. [52], 158 13- to 17-year-old adolescents gave a speech in front of an unknown audience. No differences in HR reactivity between SP adolescents, high socially anxious adolescents, and healthy controls emerged. Regarding endocrine reactivity, only one out of three studies found a higher endocrine reactivity of SPs compared with a healthy control group [91]. In this study, 6- to 12-year-old SP children and healthy controls had to complete a modified Trier Social Stress Test (TSST, [92]). SP children showed an elevated cortisol response as compared with healthy controls. However, two more studies failed to find an endocrine hyperreactivity in SP groups using a similar task [25, 93].
More evidence for a psychophysiological hyperreactivity was found in samples of children and adolescents with other subforms of social anxiety. A pattern of autonomic hyperreactivity was mostly present in samples of children and adolescents with test anxiety and high social anxiety or shyness [58, 68, 73]. For example, Beidel [58] found a higher HR reactivity during a vocabulary test and a public reading task in test anxious children compared with non-test anxious children. Further, in a study by Matthews et al. [68], a greater increase in HR and systolic blood pressure was correlated with higher social anxiety in adolescents during a social-evaluative speaking task. Likewise, most evidence for an endocrine hyperreactivity was found in subclinical social anxiety. Granger et al. [26] found that cortisol reactivity was correlated with social withdrawal, social anxiety, and socially inhibited behavior during a parent–child conflict discussion task. In a further study by Granger et al. [66], increasing social anxiety over a period of 6 months was associated with higher subsequent HPA-reactivity to a similar stressor.
Related to this, similar findings have been reported from adult social anxiety: For example, Levin et al. [94] compared the reactions of adult patients with generalized SP to adult patients with specific SP and healthy controls during a ten-minute speech. Patients with less generalized SP exceeded other patients in HR elevation prior to and during the speech, although generalized patients reported more subjective anxiety during the speech. Several other studies have yielded similar results: patients with subtypes (e.g. circumscribed speech phobia or public speaking phobia) of SP seem to show higher autonomic reactivity than patients with generalized SP [39, 95, 96]. As some authors argue that test anxiety is a form of specific SP (e.g. [97]), this could fit our results.
While many studies failed to find autonomic or endocrine hyperreactivity to stress in SP samples, we also found studies which report a blunted instead of an increased autonomic/endocrine reactivity in SP. This pattern was found in two studies with SP children [93]. In a study by Schmitz et al. [56], SP children showed a lower parasympathetic reactivity and a slower HR recovery than healthy controls when confronted with the TSST. Interestingly, similar results were also found in two studies with test anxious children [58, 61]. For example, Darley and Katz [61] exposed test anxious and non-anxious children to a cognitive task and varied the instruction given for the task (test instruction vs. game instruction). While HR generally accelerated in reaction to the test instruction and decelerated in reaction to the game instruction, in test anxious children these effects were dampened, suggesting autonomic inflexibility. Another study by Beidel [58] also found a slower recovery (post task) of HR in test anxious children compared with non-test anxious children. This finding is in keeping with previous studies on anxiety disordered and high-risk children and adolescents (e.g. [98–101]), and fits the results of a meta-analysis by Chida and Hamer [102], which found a lower ANS reactivity and slower recovery in anxious adults.
Interestingly, in the present review, several studies scattered across the different subpopulations of social anxiety report that social anxiety may be associated with an autonomic and endocrine hyperarousal during baseline and/or recovery phases and in the absence of social stress. This seems to be true for children and adolescents with SP [56, 93], test anxiety [58], and high social anxiety/shyness [68, 73]. Likewise, a tonic hyperarousal (especially concerning an elevated HR) has been found in samples across the whole anxiety spectrum, including very young children at risk for the development of anxiety [99], children and adolescents with internalizing symptoms [98], and children and adolescents with various anxiety disorders [100, 101]. Similarly, in adult samples, a tonic autonomic and endocrine hyperarousal has frequently been found [107]. Thus, chronic hyperarousal seems to be prevalent across different types of anxiety.
Developmental aspects of physiological responding in social anxiety
Children and adolescents with subclinical social fears evidenced heightened physiological reactivity, while clinical samples showed either no differential phasic (stressor related) effects or even attenuated/slowed autonomic and endocrine reactivity/recovery. This appears counterintuitive at first sight since diagnostic systems suggested increasing responses with increasing severity. Instead, our results suggest that flexibility of the physiological systems decreases as social fears become more severe and, therefore, less physiological reactivity could be a marker of increased psychopathology. This idea would fit well with current theories that link anxiety disorders to a restricted autonomic flexibility [103–107]. These theories emphasize that adaptive reactions to stressors depend on autonomic flexibility, and such flexibility—as opposed to rigidity—is considered functional and adaptive. Interestingly, according to this view, strong stress responses would be considered healthy and adaptive—rather than pathological—if they are subsequently followed by a similarly swift recovery and return to baseline. Such autonomic flexibility is thought to capitalize mainly on the parasympathetic branch of the ANS with it fast innervation though the vagus nerve [108]. A lower parasympathetic activity is thought to be connected to anxiety symptoms, including a dysfunctional attention focus, behavioral inflexibility, and reduced abilities for emotion regulation [106, 107]. A tonically elevated arousal could withdraw attention from important external cues and thus increase feelings of anxiety [56].
A developmental perspective must also be taken when explaining differences between findings in adults and findings in children and adolescents. Recent longitudinal studies on autonomic and endocrine parameters in high-risk samples suggest that dysfunctional cognitive-emotional development can to some extent be predicted by abnormal physiological profiles at younger ages. A recent study by Badanes et al. [109] showed an association of low cortisol with both family risk and internalizing symptoms in children and supported the idea that low cortisol might be a risk factor for the development of internalizing symptoms. In a large prospective cohort study of Dutch adolescents [110], signs of reduced autonomic flexibility predicted anxiety levels 2 years later in adolescent girls. Thus, reduced autonomic flexibility might represent a risk factor for anxiety. Interestingly, findings of normal or even blunted psychophysiological stress responses in children/adolescence with severe social anxiety seem to parallel the adult literature: many studies failed to find psychophysiological differences between socially anxious and non-anxious individuals [11, 12, 14, 40] or describe blunted responding [111]. Hence, in adults, social fears seem to be dominated by cognitive symptoms and subjective hyperreactivity to social stressors without an enhanced autonomic or endocrine reactivity. A psychophysiological hyperresponding seems to be confined to subclinical social anxiety in children/youth (e.g. [58, 68, 73]). Interestingly, such a higher physiological arousal seems to be present very early in development (aged 1–3) as suggested by the results of Kagan and colleagues [99] on samples of children with high levels of Behavioral Inhibition. Behavioral Inhibition in children, which is an early risk factor for SP (see also [112]), seems already to be associated with physiological abnormalities like a heightened HR and cortisol reactivity [99].
Thus, physiological differences between individuals with mild to moderate socials fears and non-anxious controls may vanish in the transition from childhood to adulthood, which could relate to a maturation of the ANS and the HPA-axis. For example, a study by Lenard et al. [20] found that with increasing age, autonomic functions seem to improve. Hence it is conceivable that physiological regulation improves from childhood to adulthood which could also dissolve autonomic and endocrine differences between anxious and non-anxious individuals. In clinical SP, however, a lower physiological reactivity seems to be stable from youth to adulthood, probably owing to the higher stability and severity of impairment.
When taking a closer look at the developmental perspective of perception bias, the current literature suggests that also cognitive biases may be predictive for the development and aggravation of social anxiety: in a cohort-sequential longitudinal study by Miers et al. [113], developmental trajectories of social anxiety in a nonclinical sample aged 9–21 years were examined. Adolescents who followed a high social anxiety trajectory were characterized by higher levels of self-reported negative interpretations and self-focused attention. Thus, physiological and cognitive variables—including distorted awareness and interpretation of bodily anxiety symptoms—may predict the course of social anxiety and are thus important risk factors for social anxiety symptoms in young adulthood.
Clinical implications
Our finding of consistently overestimated bodily symptoms bears implications for the treatment and prevention of social anxiety in children and adolescents. For example, different procedures could be applied to correct biased perceptions of bodily arousal. Through biofeedback, group role play or video feedback methods, beliefs about the own appearance during social situations could be modified and the alleged visibility of bodily symptoms could be falsified. In socially anxious adults, video feedback has already proven to be effective [114–116]: For example, in a study by Rapee and Haymann [114], socially anxious adults rated their performance in a speech more positively and more consistent with ratings by independent observers after seeing a video recording of their performance.
Psychoeducational components regarding bodily arousal could be included in the treatment of social anxiety in children and adolescents. The experience of bodily symptoms during social-evaluative situations should be normalized and reframed. This is often done by describing physiological activation, like an elevated HR, as a very common response to social stressors that is usually not visible to others (“What you feel is not always what others see”) and that is highly functional (“Bodily arousal gives you energy”, cf. [51]). In order to reduce the heightened self-focused attention on bodily symptoms in social situations, some form of attentional training might be beneficial. Socially anxious children and adolescents could learn to allocate their attention to external stimuli instead of concentrating on internal symptoms. In socially anxious adults with the core fear of showing bodily symptoms, an attentional training, which directs attention to external factors, has already proven to be effective (“task concentration training” [117]). For children with different kinds of anxiety disorders, computer-based attention bias modification has been found to reduce anxiety symptoms and severity [118]. As a biased perception of bodily anxiety symptoms seems to exist already in high-risk children, prevention methods should be applied. High-risk children might be educated in public health programs and school-based interventions. A less close coupling between social anxiety and bodily anxiety symptoms during childhood as suggested by Schmitz et al. [75] may underline the need for early cognitive-behavioral interventions in socially anxious children targeting a biased perception of bodily anxiety symptoms while there still is a less close associations between social anxiety and a misperception of bodily anxiety symptoms.
Limitations of the included studies and future directions
The following limitations may apply. Although we are confident that our database search and hand search identified most of the published studies to date, we did not systematically search for unpublished studies (“gray literature”). On the one hand, this posits a danger to our results, as significant results could be overrepresented in the literature review (“publication bias” or “file drawer problem”). Statistically significant results are more likely to be published, while studies with non-significant results often remain unpublished in researchers’ file drawers [119]. On the other hand, inclusion of unpublished studies, which did not undergo or pass peer review, could reduce the quality of the literature review. Still, it needs to be considered that more non-significant results could still be hidden.
The results of the included studies in this review were diverse and partly inconsistent. Studies concerning the first research question—the perception bias—have been more consistent than studies concerning the second research question—physiological effects. Thus, psychophysiological results seem to be more variable and method-dependent. First, this might be due to power issues, as some studies had very limited power to detect small to medium effects [e.g. 61]. Second, the assessed age groups in the studies’ samples varied across and sometimes within studies between a range of 7–18 years (with a focus on 10–12 years), which is troublesome because of age-related changes in autonomic functioning and cognitive development as reviewed above (see also Wilhelm et al. [120] for review). Thus, future studies should compare groups in a narrow age range in multiple age cohorts across late childhood and adolescence. Third, experimental tasks varied considerably between studies and were partially not uniformly well validated. Only few studies used standardized social-evaluative stressors like the TSST [92] which has the clear advantage of being fairly standardized, intensely researched in adults, and designed to allow HPA-axis assessment. Fourth, even if a standardized stressor was applied, the intensity of the stressor differed. For example, a study by van West et al. [91] found a higher endocrine reactivity of SPs compared with a healthy control group, using a shortened TSST [92], while another study by Krämer et al. [93] failed to find an endocrine hyperreactivity in an SP group using the complete TSST. Very high stressor intensity might mask group difference due to ceiling effects. Fifth, related to this, motivational theories [121, 122] suggest that very high perceived task difficulty could result in motivational disengagement, particularly in anxious individuals, which could account for normal or even blunted physiological stress responding (as in Schmitz et al. [56]). Sixth, measurement-wise, most studies focused on only a few autonomic parameters, such as HR (50 %), thereby capturing only some aspects of the multifaceted nature of autonomic functioning and ignoring important aspects of autonomic functioning such as autonomic flexibility. In our review, physiological differences between the groups emerged more often when a detailed and broad autonomic assessment was conducted [55, 56, 69]. Seventh, the temporal resolution of physiological assessments varied between the studies—some studies took measurements only during baseline and during stress conditions (e.g. [51]), while other studies went more into detail, investigating parameters under baseline, stress, and recovery conditions (e.g. [56]). A more detailed temporal assessment may improve our understanding of autonomic processes in childhood and adolescent social anxiety. In particular, studies on a perception bias in childhood social anxiety assessed physiological parameters only during baseline and stress and mostly looked only on HR, which could explain why these studies found no physiological differences between the groups.
From our findings, it remains mostly unclear whether a biased perception or autonomic and endocrine disturbances are cause or consequence of social anxiety since most studies used a cross-sectional design and participants were already affected by social anxiety at the time of the studies. Only a few studies in the current review utilized a longitudinal design: for example, a study by Schiefelbein and Susman [72] found that a greater increase in baseline cortisol across one year predicted higher social anxiety in girls at the end of their study, suggesting endocrine changes precede increased anxiety. Likewise, Granger [66] found that increasing social anxiety over a period of 6 months was associated with higher subsequent HPA-reactivity to a stressor. More longitudinal studies and prospective designs, e.g. examining high-risk samples of children from mothers with the diagnosis of SP, are needed to understand the exact role which autonomic and endocrine factors play in the development of psychopathology and how specific they are for particular disorders [104].
Last, some characteristics of anxiety disorders which have been replicated in the laboratory several times do not hold when investigated in an ambulatory context [123]. Ambulatory assessment studies are needed to examine whether the observed group differences are specific for the experimental situation or whether they generalize to naturally occurring stressors.
Methodological approach of the current review
Due to the heterogeneity of included studies, we chose to perform a review but did not perform a meta-analysis. A substantial advantage of literature reviews above meta-analyses is that a broader and more complete view can be given. Our systematic review allowed us to be more inclusive than a formal meta-analysis. Thus, studies from a number of different populations and tasks could be included without a restrictive focus on a set of comparable dimensions. This was done to generate hypotheses and future directions for this young research field. Here we reviewed studies from two research fields, biased perception and physiological arousal. We believe that the simultaneous presentation of both fields is utterly important: when looking solely on studies investigating a perceptional bias in socially anxious children and adolescents, one could get the impression that social anxiety is mainly characterized by a heightened subjective awareness of physiological arousal, but not by actual group differences in bodily parameters. However, when including physiological studies into this view, the picture becomes more complete since it shows autonomic and endocrine differences in subgroups of social anxiety. Without the consideration of the two related research fields, these differences could be overlooked and social anxiety may be understood as a mainly cognitive phenomenon.
Conclusions
Overall, in this review, we found evidence for a biased perception of bodily anxiety symptoms in socially anxious children and adolescents: Socially anxious children and adolescents overestimated their physiological arousal in most studies. An elevated psychophysiological reactivity (ANS and HPA-axis) was present only in test anxiety and high social anxiety/shyness, while we found some evidence for a blunted physiological responding or no differences in clinical SP. The issue of chronic hyperarousal needs further study in ambulatory designs. As studies were heterogeneous, more research is needed to determine the role of bodily anxiety symptoms in socially anxious children and adolescents.
Notes
DSM-5 will state almost unchanged criteria.
As items of standardized questionnaires measuring high social anxiety and high shyness are often very similar (e.g. SASC-R [48] and RCBS [49], example item SASC-R: “I feel shy around kids I don’t know” example item RCBS: “I feel tense when I’m with people I don’t know well”), these concepts will be considered almost equivalent in this review.
According to Cohen [50], d = 0.2 indicates a small effect, d = 0.5 indicates a medium effect, and d = 0.8 indicates a large effect. Regarding the effect size f, f = 0.10 indicates a small effect, f = 0.25 indicates a medium effect, and f = 0.40 indicates a large effect [50]. Regarding Pearson’s r, according to Cohen [50], r = 0.10 is a small effect, r = 0.30 is a medium effect and r = 0.50 is a large effect.
References
Clark DM, Wells A (1995) A cognitive model of social phobia. In: Heimberg RG, Liebowitz MR, Hope DA et al. (eds) Social phobia: Diagnosis, assessment, and treatment. Guilford Press, NY, pp 69–93
Albano AM, Chorpita BF, Barlow DH (2003) Childhood anxiety disorders. In: Mash EJ, Barkley RA et al. (eds) Child psychopathology (2nd ed.). Guilford Press, NY, pp 279–329
Cartwright-Hatton S, Hodges L, Porter J (2003) Social anxiety in childhood: the relationship with self and observer rated social skills. J Child Psychol Psychiatry 44(5):737–742
La Greca AM, Lopez N (1998) Social anxiety among adolescents: linkages with peer relations and friendships. J Abnorm Child Psychol 26(2):83–94
Bittner A, Egger HL, Erkanli A et al (2007) What do childhood anxiety disorders predict? J Child Psychol Psychiatry 48(12):1174–1183. doi:10.1111/j.1469-7610.2007.01812.x
Ruscio AM, Brown TA, Chiu WT et al (2008) Social fears and social phobia in the USA: results from the National Comorbidity Survey Replication. Psychol Med 38(1):15–28. doi:10.1017/S0033291707001699
American Psychiatric Association (1994) Diagnostic and statistical manual of mental disorders: DSM-IV-TR, 4th edn. American Psychiatric Association, Washington
Kessler RC, Berglund P, Demler O et al (2005) Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the national comorbidity survey replication. Arch Gen Psychiatry 62(6):593–602
Wittchen H, Fehm L (2003) Epidemiology and natural course of social fears and social phobia. Acta Psychiatrica Scandinavica 108(Suppl417):4–18
Beidel DC, Turner SM, Morris TL (1999) Psychopathology of childhood social phobia. J Am Acad Child Adolesc Psychiatry 38(6):643–650
Eckman PS, Shean GD (1997) Habituation of cognitive and physiological arousal and social anxiety. Behav Res Ther 35(12):1113–1121
Edelmann RJ, Baker SR (2002) Self-reported and actual physiological responses in social phobia. Br J Clin Psychol 41(1):1–14
Grossman P, Wilhelm FH, Kawachi I et al (2001) Gender differences in psychophysiological responses to speech stress among older social phobics: congruence and incongruence between self-evaluative and cardiovascular reactions. Psychosom Med 63(5):765–777
Mauss IB, Wilhelm FH, Gross JJ (2004) Is there less to social anxiety than meets the eye? Emotion experience, expression, and bodily responding. Cogn Emot 18(5):631–662
Mulkens S, de Jong PJ, Dobbelaar A et al (1999) Fear of blushing: fearful preoccupation irrespective of facial coloration. Behav Res Ther 37(11):1119–1128
Gerlach AL, Mourlane D, Rist F (2004) Public and private heart rate feedback in social phobia: a manipulation of anxiety visibility. Cogn Behav Ther 33(1):36–45
World Health Organization (1993) ICD-10. International statistical classification of diseases and related health problems, 10th revision. World Health Organization, Geneva
Gotthardt U, Schweiger U, Fahrenberg J et al (1995) Cortisol, ACTH, and cardiovascular response to a cognitive challenge paradigm in aging and depression. Am J Physiol 268(4 Pt 2):R865–R873
Kudielka BM, Buske-Kirschbaum A, Hellhammer DH et al (2004) HPA axis responses to laboratory psychosocial stress in healthy elderly adults, younger adults, and children: impact of age and gender. Psychoneuroendocrinology 29(1):83–98
Lenard Z, Studinger P, Mersich B et al (2004) Maturation of cardiovagal autonomic function from childhood to young adult age. Circulation 110(16):2307–2312. doi:10.1161/01.CIR.0000145157.07881.A3
Puliafico AC, Kendall PC (2006) Threat-related attentional bias in anxious youth: a review. Clin Child Fam Psychol Rev 9(3–4):162–180. doi:10.1007/s10567-006-0009-x
Muris P, Merckelbach H, van Spauwen I (2003) The emotional reasoning heuristic in children. Behav Res Ther 41(3):261–272
Garcia de Miguel B, Nutt DJ, Hood SD et al (2012) Elucidation of neurobiology of anxiety disorders in children through pharmacological challenge tests and cortisol measurements: a systematic review. J Psychopharmacol 26(4):431–442. doi:10.1177/0269881110372818
Kallen VL, Tulen JHM, Utens EMWJ et al (2008) Associations between HPA axis functioning and level of anxiety in children and adolescents with an anxiety disorder. Depress Anxiety 25(2):131–141. doi:10.1002/da.20287
Martel FL, Hayward C, Lyons DM et al (1999) Salivary cortisol levels in socially phobic adolescent girls. Depress Anxiety 10(1):25–27
Granger DA, Weisz JR, Kauneckis D (1994) Neuroendocrine reactivity, internalizing behavior problems, and control-related cognitions in clinic-referred children and adolescents. J Abnorm Psychol 103(2):267–276
Herbert JD, Hope DA, Bellack AS (1992) Validity of the distinction between generalized social phobia and avoidant personality disorder. J Abnorm Psychol 101(2):332–339
Holt CS, Heimberg RG, Hope DA (1992) Avoidant personality disorder and the generalized subtype of social phobia. J Abnorm Psychol 101(2):318–325
Cicchetti D (2006) Development and psychopathology. In: Cicchetti D, Cohen DJ (eds) Developmental psychopathology, Vol 1: Theory and method, 2nd edn. John Wiley & Sons Inc, Hoboken, pp 1–23
Rapee RM, Heimberg RG (1997) A cognitive-behavioral model of anxiety in social phobia. Behav Res Ther 35(8):741–756. doi:10.1016/S0005-7967(97)00022-3
Muris P, Mayer B, Vermeulen L et al (2007) Theory-of-mind, cognitive development, and children’s interpretation of anxiety-related physical symptoms. Behav Res Ther 45(9):2121–2132
Arntz A, Rauner M, van den Hout M (1995) ‘If I feel anxious, there must be danger’: ex-consequentia reasoning in inferring danger in anxiety disorders. Behav Res Ther 33(8):917–925
Tsigos C, Chrousos GP (2002) Hypothalamic-pituitary-adrenal axis, neuroendocrine factors and stress. J Psychosom Res 53(4):865–871
Kaltsas GA, Chrousos GP (2007) The neuroendocrinology of stress. In: Cacioppo JT, Tassinary LG, Berntson GG et al. (eds) Handbook of psychophysiology (3rd ed.). Cambridge University Press, NY, pp 303–318
Kreibig S (2010) Autonomic nervous system activity in emotion. a review. Biol Psychol 84(3):394–421
Berntson GG, Cacioppo JT, Quigley KS et al (1994) Autonomic space and psychophysiological response. Psychophysiology 31(1):44–61
McEwen BS, Wingfield JC (2010) What is in a name? Integrating homeostasis, allostasis and stress. Horm Behav 57(2):105–111. doi:10.1016/j.yhbeh.2009.09.011
Gerlach AL, Wilhelm FH, Gruber K et al (2001) Blushing and physiological arousability in social phobia. J Abnorm Psychol 110(2):247–258
Hofmann SG, Newman MG, Ehlers A et al (1995) Psychophysiological differences between subgroups of social phobia. J Abnorm Psychol 104(1):224–231
Heiser NA, Turner SM, Beidel DC et al (2009) Differentiating social phobia from shyness. J Anxiety Disord 23(4):469–476
Beaton EA, Schmidt LA, Ashbaugh AR et al (2006) Low salivary cortisol levels among socially anxious young adults: preliminary evidence from a selected and a non-selected sample. Personality Individ Differ 41(7):1217–1228
van Veen JF, van Vliet IM, DeRijk RH et al (2008) Elevated alpha-amylase but not cortisol in generalized social anxiety disorder. Psychoneuroendocrinology 33(10):1313–1321
Seeman TE, Robbins RJ (1994) Aging and hypothalamic-pituitary-adrenal response to challenge in humans. Endocr Rev 15(2):233–260
Sherman B, Wysham C, Pfohl B (1985) Age-related changes in the circadian rhythm of plasma cortisol in man. J Clin Endocrinol Metab 61(3):439–443
Deuschle M, Gotthardt U, Schweiger U et al (1997) With aging in humans the activity of the hypothalamus-pituitary-adrenal system increases and its diurnal amplitude flattens. Life Sci 61(22):2239–2246
Kaushal P, Taylor JA (2002) Inter-relations among declines in arterial distensibility, baroreflex function and respiratory sinus arrhythmia. J Am Coll Cardiol 39(9):1524–1530
Mullen B (2003) Advanced BASIC meta-analysis, 2nd. Lawrence Erlbaum, Mahwah
La Greca AM, Stone WL (1993) Social Anxiety Scale for Children—Revised: factor structure and concurrent validity. J Clin Child Psychol 22(1):17–27. doi:10.1207/s15374424jccp2201_2
Cheek JM, Buss AH (1981) Shyness and sociability. J Pers Soc Psychol 41(2):330–339. doi:10.1037/0022-3514.41.2.330
Cohen J (1988) Statistical power analysis for the behavioral sciences, 2nd edn. L. Erlbaum Associates, Hillsdale
Anderson ER, Hope DA (2009) The relationship among social phobia, objective and perceived physiological reactivity, and anxiety sensitivity in an adolescent population. J Anxiety Disord 23(1):18–26. doi:10.1016/j.janxdis.2008.03.011
Anderson ER, Veed GJ, Inderbitzen-Nolan HM et al (2010) An evaluation of the applicability of the tripartite constructs to social anxiety in adolescents. J Clin Child Adolesc Psychol 39(2):195–207. doi:10.1080/15374410903532643
Beidel DC (1991) Social phobia and overanxious disorder in school-age children. J Am Acad Child Adolesc Psychiatry 30(4):545–552. doi:10.1097/00004583-199107000-00003
Essex MJ, Klein MH, Slattery MJ et al (2010) Early risk factors and developmental pathways to chronic high inhibition and social anxiety disorder in adolescence. Am J Psychiatry 167(1):40–46. doi:10.1176/appi.ajp.2009.07010051
Krämer M, Seefeldt WL, Heinrichs N et al (2011) Subjective, autonomic, and endocrine reactivity during social stress in children with social phobia. J Abnorm Child Psychol. doi:10.1007/s10802-011-9548-9
Schmitz J, Krämer M, Tuschen-Caffier B et al (2011) Restricted autonomic flexibility in children with social phobia. J Child Psychol Psychiatry 52(11):1203–1211
van West D, Claes S, Sulon J et al (2008) Hypothalamic-pituitary-adrenal reactivity in prepubertal children with social phobia. J Affect Disord 111(2–3):281–290
Beidel DC (1988) Psychophysiological assessment of anxious emotional states in children. J Abnorm Psychol 97(1):80–82
Beidel DC (1991) Determining the reliability of psychophysiological assessment in childhood anxiety. J Anxiety Disord 5(2):139–150
Beidel DC, Turner MW, Trager KN (1994) Test anxiety and childhood anxiety disorders in African American and White school children. J Anxiety Disord 8(2):169–179
Darley SA, Katz I (1973) Heart rate changes in children as a function of test versus game instructions and test anxiety. Child Dev 44(4):784–789
Kondas O (1967) Reduction of examination anxiety and ‘stage-fright’ by group desensitization and relaxation. Behav Res Ther 5(4):275–281
Tennes K, Kreye M (1985) Children’s adrenocortical responses to classroom activities and tests in elementary school. Psychosom Med 47(5):451–460
Cartwright-Hatton S, Tschernitz N, Gomersall H (2005) Social anxiety in children: social skills deficit, or cognitive distortion? Behav Res Ther 43(1):131–141. doi:10.1016/j.brat.2003.12.003
Dietrich A, Riese H, van Roon AM et al (2009) Temperamental activation and inhibition associated with autonomic function in preadolescents. The TRAILS study. Biol Psychol 81(1):67–73. doi:10.1016/j.biopsycho.2009.02.002
Granger DA, Weisz JR, McCracken JT et al (1996) Reciprocal influences among adrenocortical activation, psychosocial processes, and the behavioral adjustment of clinic-referred children. Child Dev 67(6):3250–3262
Klimes-Dougan B, Hastings PD, Granger DA et al (2001) Adrenocortical activity in at-risk and normally developing adolescents: individual differences in salivary cortisol basal levels, diurnal variation, and responses to social challenges. Dev Psychopathol 13(3):695–719
Matthews KA, Manuck SB, Saab PG (1986) Cardiovascular responses of adolescents during a naturally occurring stressor and their behavioral and psychophysiological predictors. Psychophysiology 23(2):198–209
Mezzacappa E, Tremblay RE, Kindlon D et al (1997) Anxiety, antisocial behavior, and heart rate regulation in adolescent males. J Child Psychol Psychiatry 38(4):457–469
Miers AC, Blöte AW, Bokhorst CL et al (2009) Negative self-evaluations and the relation to performance level in socially anxious children and adolescents. Behav Res Ther 47(12):1043–1049. doi:10.1016/j.brat.2009.07.017
Miers A, Blöte A, Sumter S et al (2011) Subjective and objective arousal correspondence and the role of self-monitoring processes in high and low socially anxious youth 2(4):531–550
Schiefelbein VL, Susman EJ (2006) Cortisol levels and longitudinal cortisol change as predictors of anxiety in adolescents. J Early Adolesc 26(4):397–413
Schmidt LA, Fox NA, Schulkin J et al (1999) Behavioral and psychophysiological correlates of self-presentation in temperamentally shy children. Dev Psychobiol 35(2):119–135
Schmidt LA, Santesso DL, Schulkin J et al (2007) Shyness is a necessary but not sufficient condition for high salivary cortisol in typically developing 10-year-old children. Personality Individ Differ 43(6):1541–1551
Schmitz J, Blechert J, Krämer M et al (2012) Biased perception and interpretation of bodily anxiety symptoms in childhood social anxiety. J Clin Child Adolesc Psychol 41(1):92–102. doi:10.1080/15374416.2012.632349
Silverman WK, Albano AM (1996) Anxiety disorders interview schedule for DSM-IV. Child version. Psychological Corp, San Antonio
Shaffer D, Fisher P, Dulcan MK et al (1996) The NIMH Diagnostic Interview Schedule for Children Version 2.3 (DISC-2.3): description, acceptability, prevalence rates, and performance in the MECA study. Methods for the epidemiology of child and adolescent mental disorders study. J Am Acad Child Adolesc Psychiatry 35(7):865–877
Schneider S (2009) Kinder-DIPS. Diagnostisches Interview bei psychischen Störungen im Kindes- und Jugendalter, 2nd edn. Springer, Berlin
Kaufman J, Birmaher B, Brent D et al (1997) Schedule for affective disorders and schizophrenia for school-age children-present and lifetime version (K-SADS-PL): initial reliability and validity data. J Am Acad Child Adolesc Psychiatry 36(7):980–988. doi:10.1097/00004583-199707000-00021
Achenbach TM (1991) Child behavior checklist/4-18. Dept. of Psychiatry, University of Vermont, Burlington
Rowe DC, Plomin R (1977) Temperament in early childhood. J Pers Assess 41(2):150–156. doi:10.1207/s15327752jpa4102_5
Hartman C (2000) Dutch translation of the early adolescent temperament questionnaire internal report. University Medical Center Groningen, The Netherlands
Wolpe J, Lang PJ (1964) A fear survey schedule for use in behaviour therapy. Behav Res Ther 2:27–30
Jesness C (1988) Jesness inventory of adolescent personality. Multi-Health Systems, North Tonawanda
La Greca A (1988) Development and validation of the social anxiety scale for children: Reliability and concurrent validity. J Clin Child Psychol 17:84–91
Melfsen S, Florin I (1997) Ein Fragebogen zur Erfassung sozialer Angst bei Kindern (SASC-R-D). Kindheit und Entwicklung 6(4):224–229
Spielberger CD (1986) Preliminary manual for the state-trait personality inventory (STPI). Select Pr, San Rafael
Hodapp V (1991) Das Prüfungsängstlichkeitsinventar TAI-G: eine erweiterte und modifizierte Version mit vier Komponenten. Zeitschrift für Pädagogische Psychologie/German J Educ Psychol 5(2):121–130
Sarason SB, Davidson NK, Lighthall F et al (1958) A test anxiety scale for children. Child Dev 29(1):105–113
Achenbach TM (1991) Manual for the Youth Self-Report and 1991 Profile. University of Vermont, Department of Psychiatry, Burlington
van West D, Claes S, Sulon J et al (2008) Hypothalamic-pituitary-adrenal reactivity in prepubertal children with social phobia. J Affect Disord 111(2–3):281–290. doi:10.1016/j.jad.2008.03.006
Kirschbaum C, Pirke K, Hellhammer DH (1993) The “Trier social stress test”—A tool for investigating psychobiological stress responses in a laboratory setting. Neuropsychobiology 28(1–2):76–81
Krämer M, Seefeld W, Heinrichs N, Tuschen-Caffier B, Schmitz J, Wolf O, Blechert J (2012) Subjective, autonomic, and endocrine reactivity during social stress in children with social phobia. J Abnorm Child Psychol, 40(1):95–104
Levin AP, Saoud JB, Strauman T et al (1993) Responses of ‘generalized’ and ‘discrete’ social phobics during public speaking. J Anxiety Disord 7(3):207–221
Boone ML, McNeil DW, Masia CL et al (1999) Multimodal comparisons of social phobia subtypes and avoidant personality disorder. J Anxiety Disord 13(3):271–292
Heimberg RG, Hope DA, Dodge CS et al (1990) DSM-III-R subtypes of social phobia. Comparison of generalized social phobics and public speaking phobics. J Nerv Ment Dis 178(3):172–179
McDonald AS (2001) The prevalence and effects of test anxiety in school children educational psychology. Educ Psychol 21(1):89–101. doi:10.1080/01443410020019867
El-Sheikh M, Harger J, Whitson SM (2001) Exposure to interparental conflict and children’s adjustment and physical health: the moderating role of vagal tone. Child Dev 72(6):1617–1636
Kagan J, Reznick JS, Snidman N (1988) Biological bases of childhood shyness. Science 240(4849):167–171
Monk C, Kovelenko P, Ellman LM et al (2001) Enhanced stress reactivity in paediatric anxiety disorders: implications for future cardiovascular health. Int J Neuropsychopharmacol 4(2):199–206. doi:10.1017/S146114570100236X
Yeragani VK, Rao KA, Pohl R et al (2001) Heart rate and QT variability in children with anxiety disorders: a preliminary report. Depress Anxiety 13(2):72–77
Chida Y, Hamer M (2008) Chronic psychosocial factors and acute physiological responses to laboratory-induced stress in healthy populations: a quantitative review of 30 years of investigations. Psychol Bull 134(6):829–885. doi:10.1037/a0013342
Thayer JF, Lane RD (2000) A model of neurovisceral integration in emotion regulation and dysregulation. J Affect Disord 61(3):201–216
Beauchaine T (2001) Vagal tone, development, and Gray’s motivational theory: toward an integrated model of autonomic nervous system functioning in psychopathology. Dev Psychopathol 13(2):183–214
Porges SW (1995) Orienting in a defensive world: mammalian modifications of our evolutionary heritage a polyvagal theory. Psychophysiology 32(4):301–318
Porges SW (2007) The polyvagal perspective. Biol Psychol 74(2):116–143
Friedman BH (2007) An autonomic flexibility-neurovisceral integration model of anxiety and cardiac vagal tone. Biol Psychol 74(2):185–199
Porges SW (1992) Vagal tone: a physiologic marker of stress vulnerability. Pediatrics 90(3):498–504
Badanes LS, Watamura SE, Hankin BL (2011) Hypocortisolism as a potential marker of allostatic load in children: Associations with family risk and internalizing disorders. Develop Psychopathol 23:881–896. doi:10.1017/S095457941100037X
Greaves-Lord K, Tulen J, Dietrich A et al (2010) Reduced autonomic flexibility as a predictor for future anxiety in girls from the general population: the TRAILS study. Psychiatry Res 179(2):187–193. doi:10.1016/j.psychres.2009.04.014
Pujol J, Giménez M, Ortiz H et al (2013) Neural response to the observable self in social anxiety disorder. Psychol Med 43(04):721–731. doi:10.1017/S0033291712001857
Chronis-Tuscano A, Degnan KA, Pine DS et al (2009) Stable Early maternal report of behavioral inhibition predicts lifetime social anxiety disorder in adolescence. J Am Acad Child Adolesc Psychiatry 48(9):928–935
Miers AC, Blöte AW, Rooij M et al (2013) Trajectories of Social anxiety during adolescence and relations with cognition, social competence, and temperament. J Abnorm Child Psychol 41(1):97–110. doi:10.1007/s10802-012-9651-6
Rapee RM, Hayman K (1996) The effects of video feedback on the self-evaluation of performance in socially anxious subjects. Behav Res Ther 34(4):315–322
Harvey AG, Clark DM, Ehlers A et al (2000) Social anxiety and self-impression: cognitive preparation enhances the beneficial effects of video feedback following a stressful social task. Behav Res Ther 38(12):1183–1192. doi:10.1016/S0005-7967(99)00148-5
Kim H, Lundh L, Harvey A (2002) The enhancement of video feedback by cognitive preparation in the treatment of social anxiety. A single-session experiment. J Behav Ther Exp Psychiatry 33(1):19–37
Bögels SM (2006) Task concentration training versus applied relaxation, in combination with cognitive therapy, for social phobia patients with fear of blushing, trembling, and sweating. Behav Res Ther 44(8):1199–1210. doi:10.1016/j.brat.2005.08.010
Eldar S, Apter A, Lotan D et al (2012) Attention bias modification treatment for pediatric anxiety disorders: a randomized controlled trial. Am J Psychiatry 169(2):213–220
Easterbrook PJ, Berlin JA, Gopalan R et al (1991) Publication bias in clinical research. Lancet 337(8746):867–872
Wilhelm FH, Schneider S, Friedman BH (2006) Psychophysiological assessment. In: Hersen M (ed) Clinician’s handbook of child behavioral assessment. Elsevier Academic Press, San Diego, pp 201–231
Brehm JW, Self EA (1989) The intensity of motivation. Annu Rev Psychol 40(1):109–131. doi:10.1146/annurev.ps.40.020189.000545
Richter M, Friedrich A, Gendolla GHE (2008) Task difficulty effects on cardiac activity. Psychophysiology 45(5):869–875. doi:10.1111/j.1469-8986.2008.00688.x
Pfaltz MC, Michael T, Grossman P et al (2009) Respiratory pathophysiology of panic disorder: an ambulatory monitoring study. Psychosom Med 71(8):869–876
Conflict of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Siess, J., Blechert, J. & Schmitz, J. Psychophysiological arousal and biased perception of bodily anxiety symptoms in socially anxious children and adolescents: a systematic review. Eur Child Adolesc Psychiatry 23, 127–142 (2014). https://doi.org/10.1007/s00787-013-0443-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00787-013-0443-5