
Abstract
The validity of the DSM-IV subtypes is a recurring diagnostic debate in attention deficit/hyperactivity disorder (ADHD). Laboratory measures, such as the test of everyday attention for children (TEA-Ch) can help us address this question. TEA-Ch is a test battery covering different aspects of everyday attention relating to selective and sustained attention and attentional control. The aim of the current study was to investigate whether this instrument can differentiate between combined (ADHD-C) and inattentive subtype (ADHD-I) of ADHD. Subjects were recruited from a multidisciplinary ADHD outpatient unit and tested free of medication. Sixty-four children with a diagnosis of ADHD were included (38 with ADHD-C; 26 with ADHD-I). The control group was 76 children recruited from primary and secondary schools. Children with ADHD performed worse than controls on 6 out of 9 TEA-Ch subtests. However a regression analysis revealed that TEA-Ch subtests made only a marginal contribution to the correct classification of ADHD, once the effects of IQ and age are controlled. Confirmatory factor analysis in our ADHD group demonstrated that the three factor structure achieved a poor fit. More detailed analysis suggested that inferior performance on the tasks designed to test vigilance was not the result of deficient-sustained attention. ADHD-C and ADHD-I showed very few differences across tasks. In conclusion, our results provided not much support for the value of the ADHD-C and ADHD-I distinction in predicting difficulties in everyday attention.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Attention deficit/hyperactivity disorder (ADHD) is one of the most prevalent psychiatric conditions of childhood, and is characterized by pervasive behavioral symptoms of hyperactivity, impulsivity and/or inattention. As a result of these symptoms, children with ADHD are often impaired in a wide range of daily activities, such as learning, social and emotional functioning [21]. Following the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR) ADHD has three subtypes: ADHD predominantly inattentive subtype (ADHD-I), ADHD predominantly hyperactive/impulsive subtype (ADHD-H) and ADHD combined subtype (ADHD-C) [1]. Discriminant validity and utility of these three subtypes of ADHD continued to be questioned [2, 5, 7, 9, 17, 18, 24, 31].
On a neuropsychological level, evidence for a different cognitive profile in ADHD-I and ADHD-C is not compelling. Barkley postulated a model of ADHD in which only ADHD-C and ADHD-H, but not ADHD-I, was associated with executive function (EF) deficits, such as response inhibition, visual working memory, planning, cognitive flexibility and verbal fluency [3, 4]. A relatively consistent finding is that problems with inhibition are linked with ADHD-C. However, this is contradicted by other studies that demonstrated problems in inhibitory control are not only exclusive to ADHD-C, but also found in ADHD-I. Likewise, some studies found more problems in the broader EF domain in ADHD-C than in ADHD-I, but other studies failed to replicate this [10, 15, 18, 20, 26]. Interestingly, most of the limited number of studies failed to find significant differences between ADHD-C and ADHD-I on measures of selective, sustained or divided attention. One study found that on a test of vigilance, performance of ADHD-C deteriorated faster than that of ADHD-I [8], suggesting a specific deficit in sustained attention for ADHD-C (but see [33]).
In the present study, we used a relatively new battery assessing different aspects of attention, as a neuropsychological research tool in ADHD. The test of everyday attention for children (TEA-Ch) was developed as a modification of the test of everyday attention (TEA) [22]. The development of the TEA-Ch was model-based and theory-driven, built as it was on the tripartite model of attention proposed by Posner and Peterson [28].
On the face of it ADHD should be related to deficits on a number of subscales of the TEA-Ch. A limited number of studies have addressed this issue [12, 14, 22, 32] (for a review of these studies, see Table 1). In all of these studies, significant differences were found between children with ADHD and normal controls on some subtests, although the pattern across studies was inconsistent. There were major methodological differences between these studies that might account for this lack of consistency. These included the number of subjects, the selection of subtests of TEA-Ch used, the choice to use normal or clinical controls and the extent to which medication status use was properly controlled. Therefore, at present, it is difficult to draw firm conclusions about aspects of everyday attention in ADHD as measured with the TEA-Ch. In addition, some open questions remain, such as whether subtype differences are present on the TEA-Ch.
The main aim of the current study was to investigate differences between ADHD-C and ADHD-I in terms of aspects of everyday attention and to extend the analyses of previous studies by comparing subjects with ADHD and normal developing controls on all TEA-Ch subtests. To this end, we implemented the full range of the TEA-Ch attentional items in a large, well characterized, clinically evaluated sample of children with ADHD.
Methods
Subjects
140 (Age M = 10.19 year; SD = 2.85, range = 6–16) ADHD (n = 64; ADHD-C n = 38; ADHD-I n = 26) and control children (n = 76) took part in the study. The ADHD cases were seen in our polyclinic of the university hospital and received a formal ADHD diagnosis, based on the criteria of the DSM-IV-TR. The diagnosis was based on parent interview with the Schedule for Affective Disorders and Schizophrenia for School-Age Children, Present Version (K-SADS-P) [16]. Pervasiveness of symptoms was required with the attention subscale of the teacher report form above the 95th percentile. An ADHD diagnosis required evidence of impairment in two settings (i.e. home and school). The control group was recruited from several regular primary and secondary schools, and were also participants in a large developmental study. No participants had a history of prematurity (PML ≤ 36 weeks), head trauma or any neurological and/or psychiatric disorder according to their parents. Exclusion criteria for all subjects were neurological problems, IQ < 80, treatment with psycho stimulants within 48 h prior to testing. Table 2 presents characteristics separately by clinical diagnostic group. The study protocol is approved by the Committee of Medical Ethics of the University Hospitals of Leuven, and assent was obtained for children and informed consent for adolescents and their parents.
Instruments
Psychiatric evaluation
The K-SADS-P is a semi-structured diagnostic interview for children and adolescents aged 6–18 years, based on DSM-IV-TR diagnostic criteria [16]. The symptoms are coded as present or absent. It covers all the most frequent psychiatric disorders in childhood and adolescence. In the present study, symptoms of ADHD, oppositional defiant disorder and conduct disorder were assessed for all children. For other psychiatric conditions, the screening questions were used first and only the full criterion list was applied further if the screening was positive.
Neuropsychological measures
WISC-III
Intelligence was evaluated with the Dutch adaptation of the Wechsler Intelligence Scale for Children (WISC-III) [19]. The WISC-III comprises five verbal and five non-verbal subtests, and yields separate scores for verbal IQ (VIQ), non-verbal or performance IQ (PIQ), and full-scale IQ (FSIQ).
TEA-Ch
The Dutch adaptation of the TEA-Ch was administered to all subjects [23]. The subtests of the TEA-Ch are thought to measure selective attention (Sky Search and Map Mission) divided and sustained attention (Score!, Sky Search DT, Score!DT, Walk, Don’t Walk and Code Transmission), and attentional control (Creature Counting and Opposite Worlds). The standardization sample consisted of Dutch speaking children between the ages of 6 and 16 years. Confirmatory factor analysis (CFA) in this population replicated the original three factor structure. Most TEA-Ch subtests show adequate to strong test–retest reliability. Although the TEA-Ch consists of 9 subtests, there are 10 scores used in the analysis.
Sky Search
The child must rapidly and accurately circle paired ‘spaceship’ stimuli presented amid unpaired distracters. In the control condition, the child has to circle paired stimuli on a page without any distractors. Subtracting the control condition from the test condition provides an attention score, based on the speed and accuracy, independent of the influence of motor efficiency.
Map Mission
The child has to circle each appearance of a specific symbol on a detailed city map within 1 min. The dependent variable is the number of correct responses.
Score!
Participants silently count the number of target tones they hear on a CD. There are 10 trials, with tones ranging in number from 9 to 15 and presented at varying intervals. The dependent variable is the total of the correctly counted trials.
Sky Search Dual Task (DT)
The child simultaneously performs the Sky Search and Score! tasks. A measure of dual-task decrement is calculated, which consists of the performance decrement conferred by the dual-task load, relative to the participant’s performance on the visual search task alone.
Score! Dual Task (DT)
The child listens for an animal name distractor in a tape recorded ‘news broadcast’ while simultaneous counting of audio-taped tones (Score!). The dependent variable is the total number of correct answers for both tasks.
Walk, Don’t Walk
Go-tones are presented at a regular pace with a no-go tone that occurs unpredictably within the sequence of go-signals. On go-signals, the subject has to mark the footprint on a path (“walk”). On the no-go-tone, the subject has to withhold marking the footprint (“don’t walk”). The dependent measure is the number of times the subject successfully withholds the response to the no-go signal (maximum score of 20).
Code Transmission
The child listens for 12 min to an audiotaped recording of single digit numbers presented at 2-s intervals and has to respond with the number that precedes the occurrence of all double five-digit sequences. There are 40 target presentations and the score is the number of correct responses.
Creature Counting
Children count ‘creatures’ aligned along a path. Counting is regulated by printed arrows. Arrows pointing up indicate the need to count upward, ‘down’ pointing arrows signify a shift to counting down. The dependent measure is the total number of correct trials and the total time needed for the correct trials.
Opposite Worlds
This task consists of two conditions: a control (‘same world’) and an attentional control (‘opposite worlds’) condition. In the ‘same world’, the child has to read out digits 1 and 2 that are displayed in a mixed, quasi-random array. In the ‘opposite worlds’, participants are asked to say the opposite for each digit. The difference between the mean time needed to complete the ‘opposite worlds’ trials and the mean time needed to complete the ‘same world’ trials is the dependent variable.
The TEA-Ch consists of five tasks designed to measure sustained attention. However, the standard scoring of these tasks does not allow the assessment of whether there is a differential decrement in attention across the task session, implied by the concept of sustained attention deficit. In the current paper, therefore, if a significant effect was found on one of these tasks we also analyzed the pattern of change over time.
Analysis
First, univariate ANCOVAs were performed for the nine subtests of the TEA-Ch. Age and total IQ were entered as covariates into the analyses. To control for multiple testing, we used the conservative Bonferroni’s correction (=α/number of comparisons): This was adjusted to α = 0.005 (9 subtests, but 10 comparisons). If a significant effect of group emerged then post hoc comparisons, using the Bonferroni’s post hoc test, were performed. A binary logistic regression analysis was performed to identify which, if any, tests made independent contributions to differentiating ADHD cases from controls. Both age and IQ were included in these analyses by regressing them on test scores and then using the standardized residual as the predictor in the model. Repeated measures, with age and FSIQ as covariates, were conducted for the analysis of the performance on the ‘sustained’ attention tasks, with section as the within-subject variable. CFAs were performed to determine whether the three factor structure of the TEA-Ch could be replicated in our control and ADHD samples. In line with the theoretical recommendations [6], several fit indices were used to assess the model fit: χ2, χ2/df (CMIN/df), root mean square error approximation (RMSEA), the goodness-of-fit index, the adjusted goodness-of-fit (AGFI) and the comparative fit index (CFI). A statistical non-significant χ2 value and a CMIN/df ≤ 3 indicate an acceptable model. Values of RMSEA up to 0.08, GFI and CFI > 0.90, and AGFI > 0.85 indicate proper fit. All statistical procedures were carried out using the SPSS-16 statistical package and Lisrel 8.71 for CFA.
Results
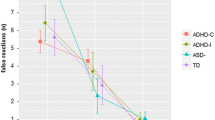
The analysis with α-set at P = 0.05 threshold revealed seven differences on six subtests between ADHD and control groups (Creature Counting: accuracy and speed, Code Transmission, Map Mission, Score!, Score!DT and Walk, Don’t Walk). Correcting for multiple tests reduced this to just two subtests: Creature Counting (accuracy and speed) and Code Transmission (see Table 3). The six subtests for which there was a significant effect of group were included as predictors in a logistic regression model. In the first model, we used scores uncorrected for age and IQ. 76.7% of subjects were correctly classified [χ2(7, n = 120) = 41.45, P < 0.001]. Two test scores contributed significantly to this model: Code Transmission [Wald χ2 (1) = 4.16, P = 0.04, odds ratio = 0.90] and Creature Counting accuracy [Wald χ2 (1) = 4.12, P = 0.04, odds ratio = 0.67]. When age was controlled, the percentage correct classification was 73.3% [χ2(7, n = 120) = 39.38, P < 0.001]. One additional variable contributed significantly to the model: Map Mission [Wald χ2 (1) = 5.77, P = 0.02, odds ratio = 0.55], Code Transmission [Wald χ2 (1) = 4.67, P = 0.03, odds ratio = 0.49] and Creature Counting accuracy [Wald χ2 (1) = 4.23, P = 0.04, odds ratio = 0.51]. When age and IQ were controlled, the percentage correct classification dropped to 69.2% [χ2(7, n = 120) = 26.11, P < 0.001]. Only one score contributed significantly to the model: Map Mission [Wald χ2 (1) = 4.23, P = 0.04, odds ratio = 0.64]. There was a significant difference between ADHD-C and ADHD-I for the subtest Creature Counting (accuracy but not speed). For the subtest Code Transmission, no significant difference between ADHD-C and ADHD-I was found. Both groups performed significantly worse than the control group. Furthermore, there was no differential effect of time on task suggesting that differences between ADHD children and controls are not due to sustained attention deficits. CFA in the control sample shows for most fit indices that the three-factor structure achieved a mediocre fit [χ2 = 32.86 (24), P > 0.05; CMIN/df = 1.46; RMSEA = 0.073 (0.0; 0.13); GFI = 0.91; AGFI = 0.82; CFI = 0.88]. In contrast, CFA shows for all indices that the three-factor structure in our ADHD group achieved a poor fit [χ2 = 39.71 (24), P < 0.05; CMIN/df = 1.88; RMSEA = 0.11 (0.042; 0.17); GFI = 0.86; AGFI = 0.73; CFI = 0.81].
Discussion
The aim of the present study was to investigate whether differences exist in everyday aspects of attention for children with ADHD-C and ADHD-I, and whether each of these groups differs from controls without ADHD. Once adjusted for multiple testing children with ADHD were found to perform worse on two subtests: Creature Counting (accuracy and speed) and Code Transmission. For four other tasks, a marginally significant effect was apparent: Map Mission, Score!, Score!DT and Walk, Don’t Walk. The results of the logistic regression analysis illustrated that there is not much evidence that these subtests made independent contributions to differentiating ADHD cases from controls. Therefore, the diagnostic utility of the TEA-Ch for the clinical assessment of ADHD is limited. In addition, considering the three-factor structure of the TEA-Ch our results demonstrate an inconsistent picture of subtests that differentiate between ADHD and controls. Effects were seen on at least one, but never all tasks loading on a factor: selective attention (Map Mission, but not Sky Search), sustained attention (Score!, Score!DT, Walk, Don’t Walk, Code Transmission, but not Sky Search DT) and attentional control (Creature Counting, but not Opposite Worlds). To some extent, this may be explained by the presence of ceiling effects for some tasks (e.g. Sky Search: more than 50% of subjects obtained a score above 18; [22]). The results of our CFAs suggest that the factor structure of the TEA-Ch is different in the control and ADHD groups. As far as subtype differences are concerned, effects were seen only on one of the two tasks measuring attentional control (Creature Counting). Furthermore, ADHD-C performed significantly worse than ADHD-I for accuracy and not speed. ADHD-I and control children perform equally well on Creature Counting. Although this finding suggests a selective deficit in attentional control in ADHD-C, we did not find a significant effect on another subtest measuring attentional control, Opposite Worlds. Why should this be the case? There are some fundamental differences in the underlying mechanism needed for good performance on the two tasks. Opposite Worlds can be considered as a Stroop-like task. Interference control suppressing the dominant response of reading what you see (say 2 when you see 1) is essential for good performance on this task. Two recent meta-analyses revealed that Stroop interference deficits cannot be found consistently in ADHD [30, 34]. The absence of a group effect on Opposite Worlds is in keeping with these studies. Good performance on Creature Counting requires that one can switch between two cognitive sets. Two classic neuropsychological measures, Wisconsin Card Sort Test [11] and trail making test [29] have been extensively used to assess set shifting in ADHD. A recent meta-analysis study reported moderate effect sizes for ADHD on these tests (d = 0.46 and 0.55, respectively) [35]. No differences between ADHD-C and ADHD-I were observed on these measures. Despite the fact that Creature Counting relies on set shifting and one cannot exclude other cognitive functions as being implicated. Indeed, it remains unclear whether switching is a separate operation or is the culmination of other cognitive processes, such as working memory, task activation, or response suppression. Application of more refined paradigms in ADHD and its subtypes are warranted to clarify this issue. The TEA-Ch is constructed to assess everyday aspects of attention, but at least three subtests (Creature Counting, Opposite Worlds and Walk, Don’t Walk) rely also on EF. According to the hypothesis of Barkley one could expect that ADHD-C will perform worse on all three tasks in comparison with ADHD-I. However, our results do not suggest that ADHD-C is characterized by a generalized EF deficit.
Both ADHD-C and ADHD-I performed significantly worse on Code Transmission. A more detailed analysis of the results indicated that neither ADHD-C nor ADHD-I demonstrated a more pronounced vigilance decrement than the control group as a function of time on task. This indicates that there is no problem with sustained attention in the ADHD patient group, but potentially a problem with alerting/arousal [25, 27, 28]. However, for this task, the participants need not only to stay alert, but also have to keep the last three numbers in mind. Our results do not allow us to say whether arousal or working memory problems or an interaction of both are at the origin of the problems ADHD children encounter on this task.
The study had a number of limitations. Our sample was heterogeneous. We did not exclude children with ADHD and co-morbid disorders because a sample of children with pure ADHD and no co-morbid conditions would be unrepresentative of the clinical population. When children with co-morbid conditions were removed from the analysis, our pattern of findings remained unaffected. Unfortunately, sample size limitations make it difficult to further explore the impact of specific co-morbid problems. In the present study, we used the DSM-IV-TR guidelines to define ADHD subtypes. Recent research on the Sluggish Cognitive Tempo (SCT) type suggest that individuals with SCT may constitute a purer form of the ADHD-I subtype that is categorically different from the ADHD-C type [24]. However, a categorical approach using DSM-IV-TR or SCT criteria can be questioned, on the grounds that symptom threshold and ‘purity’ of subtypes are unresolved issues. Therefore, some authors argue that the possibility of finding differences between ADHD-C and ADHD-I is limited by using the DSM-IV-TR criteria [13].
From a clinical point of view, this study provides further evidence against the discriminant validity of ADHD-C and ADHD-I subtypes as defined by DSM-IV-TR. Children with ADHD, irrespective of subtypes demonstrated some problems on the TEA-Ch. The authors of the TEA-Ch caution that the TEA-Ch is not diagnostic of a psychiatric/behavioral disorder. The results of our logistic regression analysis confirm that the TEA-Ch cannot be used in isolation to diagnose ADHD. In addition, our results suggest one should be cautious when interpreting the scores of the TEA-Ch on a number of grounds. We did not replicate the three-factor structure in our ADHD group. Furthermore, poor performance on code transmission did not seem to be the result of problems with sustained attention. From this final perspective, our results support the evidence that children with ADHD do not demonstrate problems with sustained attention.
References
American Psychiatric Association (2000) Diagnostic and statistical manual of mental disorders (4th Ed. Text Revision). Author, Washington, DC
Baeyens D, Roeyers H, Walle JV (2006) Subtypes of attention-deficit/hyperactivity disorder (ADHD): distinct or related disorders across measurement levels? Child Psychiatry Hum Dev 36:403–417
Barkley RA (1997) ADHD and the nature of self control. Guilford Publisher, New York
Barkley RA (1997) Behavioral inhibition, sustained attention, and executive functions: constructing a unifying theory of ADHD. Psychol Bull 121:65–94
Barkley RA, Cook EH, Diamond A, Zametkin A, Thapar A, Teeter A et al (2002) International consensus statement on ADHD—January 2002. Clin Child Family Psychol Rev 5:89–111
Bollen KA, Long JS (1993) Testing structural equation models. Sage, Newbury Park
Carlson CL, Tamm L, Gaub M (1997) Gender differences in children with ADHD, ODD, and co-occurring ADHD/ODD identified in a school population. J Am Acad Child Adolesc Psychiatry 36:1706–1714
Collings RD (2003) Differences between ADHD inattentive and combined types on the CPT. J Psychopathol Behav Assess 25:177–189
Gaub M, Carlson CL (1997) Behavioral characteristics of DSM-IV ADHD subtypes in a school-based population. J Abnorm Child Psychol 25:103–111
Geurts HM, Verte S, Oosterlaan J, Roeyers H, Sergeant JA (2005) ADHD subtypes: do they differ in their executive functioning profile? Arch Clin Neuropsychol 20:457–477
Heaton RK, Chelune GJ, Talley JL, Kay GG, Curtis G (1993) Wisconsin card sorting test (WCST) manual, revised and expanded. Psychological Assessment Resources, Odessa
Heaton SC, Reader SK, Preston AS, Fennell EB, Puyana OE, Gill N, Johnson JH (2001) The test of everyday attention for children (TEA-Ch): patterns of performance in children with ADHD and clinical controls. Child Neuropsychol 7:251–264
Hinshaw SP (2001) Is the inattentive type of ADHD a separate disorder? Clin Psychol Sci Pract 8:498–501
Hood J, Baird G, Rankin PM, Isaacs E (2005) Immediate effects of methylphenidate on cognitive attention skills of children with attention-deficit-hyperactivity disorder. Dev Med Child Neurol 47:408–414
Houghton S, Douglas G, West J, Whiting K, Wall M, Langsford S, Powell L, Carroll A (1999) Differential patterns of executive function in children with attention-deficit hyperactivity disorder according to gender and subtype. J Child Neurol 14:801–805
Kaufman J, Birmaher B, Brent D, Rao U, Flynn C, Moreci P, Williamson D, Ryan N (1997) Schedule for affective disorders and schizophrenia for school-age children-present and lifetime version (K-SADS-PL): initial reliability and validity data. J Am Acad Child Adolesc Psychiatry 36:980–988
King C, Young D (1982) Attentional deficits with and without hyperactivity: teacher and peer perceptions. J Abnorm Child Psychol 10:483–496
Klorman R, Hazel-Fernandez LA, Shaywitz SE, Fletcher JM, Marchione KE, Holahan JM et al (1999) Executive functioning deficits in attention-deficit/hyperactivity disorder are independent of oppositional defiant or reading disorder. J Am Acad Child Adolesc Psychiatry 38:1148–1155
Kort W, Schittekatte M, Dekker PH, Verhaeghe P, Compaan EL, Bosmans M, Vermeir G (2005) Nederlandse bewerking van de WISC-III: handleiding en Verantwoording. Harcourt Test Publisher, Amsterdam
Lockwood KA, Marcotte AC, Stern C (2001) Differentiation of attention-deficit/hyperactivity disorder subtypes: application of a neuropsychological model of attention. J Clin Exp Neuropsychol 23:317–330
Lollar DJ (2008) Function, impairment, and long-term outcomes in children with ADHD and how to measure them. Pediatr Ann 37:6–28
Manly T, Anderson V, Nimmo-Smith I, Turner A, Watson P, Robertson IH (2001) The differential assessment of children’s attention: the test of everyday attention for children (TEA-Ch), normative sample and ADHD performance. J Child Psychol Psychiatry 42:1065–1081
Manly T, Roberston IH, Anderson V, Nimmo-Smith I (2004) Handleiding van de test of everyday attention for children, Nederlandse vertaling. Harcourt Test Publishers, Amsterdam
Milich R, Balentine AC, Lynam DR (2001) ADHD combined type and ADHD predominantly inattentive type are distinct and unrelated disorders. Clin Psychol Sci Pract 8:463–488
Nigg JT (2006) What causes ADHD? Understanding what goes wrong and why. Guilford Publications, New York
Nigg JT, Blaskey LG, Huang-Pollock CL, Rappley MD (2002) Neuropsychological executive functions and DSM-IV ADHD subtypes. J Am Acad Child Adolesc Psychiatry 41:59–66
Parasuraman R, Warms JS, See JE (1998) Brain systems of vigilance. In: Parasuraman R (ed) The attentive brain. MIT Press, Cambridge, pp 221–256
Posner MI, Petersen SE (1990) The attention system of the human brain. Annu Rev Neurosci 13:25–42
Reitan RM, Wolfson D (1985) The Halstead–Reitan neuropsychological test battery. Neuropsychology Press, Tucson
Schwartz K, Verhaeghen P (2008) ADHD and Stroop interference from age 9 to age 41 years: a meta-analysis of developmental effects. Psychol Med 38:1607–1616
Skansgaard EP, Burns GL (1998) Comparison of DSM-IV ADHD combined and predominantly inattention types: convergent and discriminant validity between teacher ratings and direct observations of inattentive, hyperactivity/impulsivity, slow cognitive tempo, oppositional defiant, and overt conduct disorder symptoms. Child Fam Behav Ther 20:1–14
Sutcliffe PA, Bishop DVM, Houghton S (2006) Sensitivity of four subtests of the test of everyday attention for children (TEA-Ch) to stimulant medication in children with ADHD. Educ Psychol 26:325–337
van der Meere J, Wekking E, Sergeant J (1991) Sustained attention and pervasive hyperactivity. J Child Psychol Psychiatry 32:275–284
van Mourik R, Oosterlaan J, Sergeant JA (2005) The Stroop revisited: a meta-analysis of interference control in AD/HD. J Child Psychol Psychiatry 46:150–165
Willcutt EG, Doyle AE, Nigg JT, Faraone SV, Pennington BF (2005) Validity of the executive function theory of attention-deficit/hyperactivity disorder: a meta-analytic review. Biol Psychiatry 57:1336–1346
Acknowledgments
The authors thank all participants, parents and their schools for their willing collaboration. We thank Joke Dillen and Elsbeth Kenens for assistance with data collection and Katrien Verstraeten for assistance with the confirmatory factor analyses.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Lemiere, J., Wouters, H., Sterken, C. et al. Are children with ADHD predominantly inattentive and combined subtypes different in terms of aspects of everyday attention?. Eur Child Adolesc Psychiatry 19, 679–685 (2010). https://doi.org/10.1007/s00787-010-0105-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00787-010-0105-9