
Abstract
Objectives
To evaluate the postoperative sensitivity of restorations with self-adhesive resin composite (SAC) (Vertise Flow (VER)/Kerr) compared with conventional resin composite with self-etching adhesive (Filtek Z250 (Z250)/3M ESPE; Clearfil SE Bond (CSEB)/Kuraray).
Materials and methods
A randomized, controlled, double-blind, split-mouth, two-arm clinical trial was conducted. Twenty-seven volunteers with third molars indicated for extraction received two deep class I restorations, one with each material. Postoperative sensitivity was measured at 24 h and 15 or 30 days after the restorative procedures using a visual analog scale (VAS). When present, information on the characteristics of the pain was also collected. The data were submitted to the McNemar test (α = 0.05).
Results
Regardless of the time intervals, the postoperative sensitivity was observed in 52% and 48% of the CSEB and VERT groups, respectively (p = 1.000). When the evaluation periods were analyzed, the 15-day evaluation presented the highest occurrence of pain, but of mild intensity, in both groups. All patients with sensitivity reported that the pain was localized and of short duration.
Conclusion
Self-adhesive resin composite Vertise Flow and conventional resin composite with a self-etching bonding agent promoted similar response regarding postoperative sensitivity in deep class I cavities. When postoperative sensitivity was present, mild pain was observed, especially after 15 days of the restorative procedure, which decreased over time.
Clinical relevance
Postoperative sensitivity to self-adhesive resin composite (SAC) restorations in deep cavities was comparable with that of conventional restorations with a self-etching bonding agent.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Simplification of the restorative procedure has always been a clinical aim, not only to reduce the number of operative procedures but also to decrease the number of possible errors from multiple steps. Adequate acid etching in dentin and ideal moisture for monomeric penetration, complete elimination of solvents, and depletion of unprotected collagen fibers are some of the problems that can occur during the bonding procedures [1, 2]. Self-adhesive restorative materials have been developed to simplify and minimize those problems which can, therefore, reduce postoperative sensitivity [1].
The self-adhesive resin composite (SAC) acts simultaneously as a self-etching adhesive and a flowable resin, thus eliminating the acid etching step and separate application of a bonding agent [3, 4]. The bonding mechanism to the dental structure comes from the presence of acidic monomers such as glycerol phosphate dimethacrylates (GPDM), carboxylic methacrylates (for example, 4-MET) or phosphate ethyl methacrylates (BMEP). The acidity varies from mild (GPDM, pH = 1.9) to ultra-mild (4-MET, pH = 3–4) which renders the self-conditioning of the substrate penetrating through the smear layer to form a submicrometer-thick hybrid layer [5]. Hydroxyethyl methacrylate (HEMA) is added to increase the wettability of the material on the dentin surface, and the adhesiveness occurs through micromechanical interlocking and chemical bonding to the calcium ions present in the dentine [6].
Limited information is available on the clinical performance of SACs [7]. Two studies evaluated the postoperative sensitivity of these materials with evaluations immediately after the restorative procedure, after 1 week or after longer observation periods (6, 12, 24 months) [8, 9]. The postoperative sensitivity is from the activation of nerve fibers by external stimuli after the restorative procedure [10, 11]. It is characterized by an acute pain that can last for days or weeks and disappears when the stimulus is removed [10]. Adequate bonding and seal are essential to prevent postoperative sensitivity, which leads to restoration failure [12].
Therefore, this study is aimed at evaluating the postoperative sensitivity of restorations with SAC (Vertise Flow/Kerr) compared with conventional resin composite with self-etching adhesive (Filtek Z250/3M ESPE and Clearfil SE Bond/Kuraray). The null hypothesis tested was that no difference would be found regarding the postoperative sensitivity between restorative techniques.
Materials and methods
Study design
A randomized, controlled, double-blind, split-mouth, two-arm clinical trial was conducted. This study was approved by the Ethics and Research Committee of the Universidade of Pernambuco (1.879.562) and registered by the Brazilian Registry of Clinical Trials (ReBEC) (RBR-5ggyf5).
Population and sample size
Twenty-seven volunteers were recruited at the Buco-Maxillofacial Surgery and Traumatology Service of the Dental School, Universidade de Pernambuco (FOP/UPE), PE, Brazil. Participants were aged between18 and 40 years (mean 25.92 years) and of both sexes. A total of fifty-four third molars with an indication of extraction were included.
Eligibility criteria
The study inclusion criteria were (1) two third molars indicated for extraction for orthodontic reasons; (2) healthy teeth without caries, score “0” according to the International Caries and Assessment System (ICDAS); (3) complete root development; and (4) fully erupted teeth.
Teeth without pulpal vitality or with altered pulpal vitality demonstrated using cold sensitivity tests, percussion, or palpation; the presence of pulpal calcification; and the impossibility of isolation with rubber dam were excluded.
Randomization, allocation, and blinding
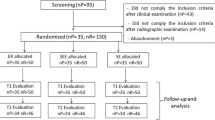
A total of 54 restorations in 27 volunteers were performed by the same operator (Fig. 1). Each participant received two restorations according to the experimental groups (Table 1). The restorative procedure followed the sequence of quadrants (upper right, upper left, lower left, lower right). For the choice of restorative material, a simple randomization scheme was used immediately before the bonding procedures. A researcher who was not involved in the clinical and evaluation procedures chose the restorative material to be used, by tossing a coin, where “tails” would represent the self-adhesive resin composite group (VERT), and “heads” the teeth restored using the conventional technique with prior bonding procedure (CSEB). Patients and evaluators were not aware of the type of material used for each tooth.

A flowchart of the study
Clinical procedure
Cavity preparation
One previously calibrated operator performed all restorations. Before the restorative procedure, a periapical and a bite-wing radiograph was made. In order to standardize the cavity preparation depth (1 mm from the roof of the pulp chamber), the distance from the occlusal surface to the roof of the pulp chamber was used for measuring with the radiograph. Anesthesia was done with 2% mepivacaine with epinephrine 1:100,000 (DFL, Rio de Janeiro, RJ, Brazil), followed by tooth prophylaxis with pumice/water slurry.
For cavity preparation, a long pear-shaped carbide bur (no. 245, KG Sorensen, Barueri, Brazil) was used with a high-speed handpiece with intermittent movements and abundant air/water spray. A groove was made in each bur to serve as a “stop,” limiting the depth of the preparation (1 mm from the roof of the pulp chamber). The mesiodistal extension of the cavity comprised 1/3 of the intercuspal distance. Each bur was only used once.
After preparing the cavity, another bite-wing radiograph was made to confirm the cavity depth. Rubber dam isolation was done, and the cavities were disinfected with a 0.12% chlorhexidine solution. Randomization (coin-tossing) was then performed.
Restorative procedure
The restorative materials were applied according to the manufacturers’ instructions (Table 1). All photoactivation procedures were performed with halogen light (Ultralux, Dabi Atlante, Ribeirão Preto, SP, Brazil) at a power density of 800 mW/cm2, previously measured with a radiometer.
After restoration placement, the occlusal contacts were evaluated with marking paper. The finishing and polishing were performed in the same session. Initially, a flame-shaped fine diamond rotary instrument (no. 3118F, KG Sorensen) was used at high speed under abundant air/water spray and intermittent movement. Afterward, the restoration was polished with rubber points in decreasing order of abrasiveness using a low-speed handpiece (Microdont, São Paulo, SP, Brazil). Both restorations were done during the same clinical appointment.
Postoperative tooth sensitivity
Postoperative sensitivity was evaluated at 24 h and 15 and 30 days after the restorative procedure. Information on the presence of pain was collected (present or absent). If present, the characteristics of the pain were recorded: the localization of pain (localized or diffuse), the type of stimulus (triggered or spontaneous), the duration of pain (short or prolonged), its frequency (intermittent or continuous), and intensity of pain (mild, moderate or severe). Thermal stimulation (refrigerant spray Endo-Ice) was used to evaluate the type of stimulus. The pain intensity was recorded with the visual analog scale (VAS). The VAS consists of a 100-mm line divided into equal intervals of 10 mm, where 0 represents “absence of pain” and 100 “severe pain.” The results of VAS were classified as mild (0–30 mm), moderate (40–70 mm), or severe pain (> 70 mm).
After each evaluation period, the patients had the tooth extracted as previously recommended.
Statistical analysis
For the age variable, the data were analyzed descriptively through the mean, standard deviation, and median. For the categorical variables, absolute and relative frequencies (percentage) were calculated. Restorative techniques were compared with the McNemar test, considering a 5% margin of error. The IBM SPSS software (Statistical Package for the Social Science, version 23) was used for data entry and statistical analysis.
Results
Two patients with 4 third molars were excluded after enrollment because of lost to follow-up. The remaining 50 third molars of 25 patients (56% male vs. 44% female) were included (Table 2). Regardless of the time intervals, postoperative sensitivity was observed in 52% and 48% of the CSEB and VERT groups, respectively. No differences were observed between the postoperative sensitivity of the studied groups (p = 1.000) regardless of the time intervals (Table 3).
None of the characteristics related to pain sensitivity, localization, type of stimulus, duration, frequency, and intensity demonstrated statistical differences between groups (Table 3). Regarding the type of stimulus, triggered pain corresponded to 92.3% of the CSEB group and 91.7% of the VERT group. As for pain intensity, most was considered mild for both VERT (75%) and CSEB (76.9%). Moderate pain was observed in the CSEB (23.1%), and severe pain (8.3%) was only observed in VERT. No statistical differences were observed between groups. All patients who had postoperative sensitivity reported that the pain was localized and of short duration with both materials.
When the evaluation period was considered for both VERT and CSEB groups, the 15-day time point presented the highest pain occurrence (87.5%) of mild intensity (Table 4). On the 30th day, the CSEB group presented higher pain percentages (33.3%) when compared with those of VERT (22.2%), also of mild intensity. However, the Fisher exact test found significant differences between evaluation periods only for the VERT group (p = 0.023).
Discussion
The null hypothesis tested was not rejected as no differences were observed between the restorative materials studied. The frequency of postoperative sensitivity after restorative procedures has been reported between 33 and 47%, with a higher prevalence in posterior teeth and class II restorations [13,14,15,16]. This range is consistent with our results (48% to 52%). The characteristics that participants described more commonly were intensity (moderate pain), duration (short), and type (provoked) [17]. The results found in our study disagreed only in the evaluation of pain intensity, which was mild.
When the evaluation periods were analyzed, the highest means of postoperative sensitivity were found in the first 15 days for both materials, decreasing considerably up to 30 days. Independent of the restorative materials used, the higher sensitivity intensity in this period was also a result of the trauma generated during cavity preparation, the cavities’ depth (with only 1 mm of remaining dentin occlusal to the pulp chamber), and the participant’s threshold and the subjectivity of each individual’s pain. The polymerization shrinkage of the resin composite may also contribute to postoperative sensitivity from the stresses generated at the adhesive interface [16]. The shrinkage can lead to incompletely sealed margins, increasing the occurrence of microleakage [15, 18]. Self-adhesive materials do not remove the smear layer, reducing the communication to the pulp tissue via dentin tubules and, consequently, substantially reducing the potential for postoperative sensitivity caused by the incomplete impregnation of the resinous monomers in the demineralized dentin [3, 13]. Vichi et al. [19] showed that the SACs had lower microleakage potential when compared with that of conventional resin composites. The authors speculated that the presence of hydrophilic monomers increased the hygroscopic expansion of these materials, which could improve the marginal seal. However, the hydrophilicity may facilitate network plasticization, enhance biofilm formation, and increase the degradation of the resin composite [5, 20].
The clinical performance of these materials has been evaluated in noncarious cervical lesions compared with a nanohybrid resin composite with a separate bonding agent. After 6 months, 27 of 40 restorations with SAC were not clinically acceptable after loss of retention. The clinical success of SACs was 33% compared with the 100% success of the conventional nanohybrid resin composite [21]. SAC was also evaluated as a pit fissure sealant for 24 months [22]. A 62.9% retention rate was observed when compared with 95.7% for conventional flowable resin composite. The short follow-up period of the present study could have favored the good retention rates of SAC. Pinna et al. [23] evaluated the use of SAC in patients with dentin hypersensitivity compared with Universal Dentine Sealant, Clearfil Protect Bond, and Flor-Opal Varnish. After a 12-week follow-up period, all treatments decreased dental hypersensitivity, with no differences among them.
The age range in this study (18 to 40 years) was similar to that in previous studies that evaluated postoperative sensitivity after restorative procedures [24, 25]. Patient age is an important factor, as the dentinal tubules are partially or completely obliterated in older patients due to increased peritubular dentin production [26]. In the present study, the same participant received both experimental treatments. The split-mouth clinical study model allows the analysis of the test and control groups under the same conditions, thus increasing statistical efficiency and decreasing the number of participants needed for the study [27].
Many methods have been used to evaluate pain intensity, including the verbal rating scale (VRS), numeric rating scale (NRS), and visual analog scale (VAS). All these scales have shown to be valid and reliable [28]. Notwithstanding, VAS has been the most commonly used method to evaluate postoperative sensitivity in clinical studies [29,30,31].
Although 48 to 52% of participants reported postoperative sensitivity, most experienced mild intensity, decreasing with time. A meticulous operative procedure with these restorative materials by following the manufacturer’s instructions could have favored a proper seal of the dentinal tubules, thus reducing dentin permeability and, therefore, postoperative sensitivity [15].
Conclusion
Self-adhesive resin composite Vertise Flow and conventional resin composite with a self-etching bonding agent promoted similar response regarding postoperative sensitivity in deep class I cavities. When postoperative sensitivity was present, mild pain was observed in about half the participants; this decreased over time.
References
Ferracane JL (2011) Resin composite state of the art. Dent Mater 27:29–23
Miyazaki M, Tsujimoto A, Tsubota K, Takamizawa T, Kurokawa H, Platt JA (2014) Important compositional characteristics in the clinical use of adhesive systems. J Oral Sci 56:1–9
Rahimian-imam S, Ramazani N, Fayazi MR (2015) Marginal microleakage of conventional fissure sealants and self-adhering flowable composite as fissure sealant in permanent teeth. J Dent (Tehran) 12:430–435
Radovic I (2008) Self-adhesive resin cements: a literature review. J Adhes Dent 10:251–258
Maas MS, Alania Y, Natale LC, Rodrigues MC, Watts DC, Braga RR (2017) Trends in restorative composites research: what is in the future? Braz Oral Res 31:e55
Shafiei F, Saadat M (2016) Micromorphology and bond strength evaluation of adhesive interface of a self-adhering flowable composite resin-dentin: effect of surface treatment. Microsc Res Tech 79:403–407
Sachdeva P, Goswami M, Singh D (2016) Comparative evaluation of shear bond strength and nanoleakage of conventional and self-adhering flowable composites to primary teeth dentin. Contemp Clin Dent 7:32631
Celik EU, Kucukyilmaz E, Savas S (2015) Effect of different surface pre-treatment methods on the microleakage of two different self-adhesive composites in class V cavities. Eur J Paediatr Dent 16:33–38
Sabbagh J, Dagher S, El Osta N, Souhaid P (2017) Randomized clinical trial of a self-adhering flowable composite for class I restorations: 2-year results. Int J Dent 2017:5041529
Berkowitz GS et al (2009) Postoperative hypersensitivity in class I resin-based composite restorations in general practice: interim results. Compend Contin Educ Dent 30:356–363
Davidovic L, Radovic I, Krunic J (2014) Prevention of postoperative sensitivity in composite restorations. Serbian Dent J 61:84–92
Oz FD, Kutuk ZB, Ozturk C, Soleimani R, Gurgan S (2019) An 18-month clinical evaluation of three different universal adhesives used with a universal flowable composite resin in the restoration of non-carious cervical lesions. Clin Oral Investig 23:1443–1452
Porto ICCM (2012) Post-operative sensitivity in direct resin composite restorations: clinical practice guidelines. IJRD 1:1–12 Available from: http://jrdindia.org/ver2/app/upload/review1.pdf
Uneromi M et al (2001) Composite resin restoration and postoperative sensitivity: clinical follow-up in an undergraduate program. J Dent 29:7–13
Casselli DSM, Martins LRM (2006) Postoperative sensitivity in class I composite resin restorations in vivo. J Adhes Dent 8:53–58
Reis A, Loguercio AD, Schroeder M, Luque-Martinez I, Masterson D, Maia LC (2015) Does the adhesive strategy influence the post-operative sensitivity in adult patients with posterior resin composite restorations? A systematic review and metaanalysis. Dent Mater 31:1052–1067
Yousaf A, Aman N, Manzoor MA, Shah JÁ, Dilrasheed (2014) Postoperative sensitivity of self etch versus total etch adhesive. J Coll Physicians Surg Pak 24:383–386
Moosavi H, Maleknejad F, Sharifi M, Ahrari F (2015) A randomized clinical trial of the effect of low-level laser therapy before composite placement on postoperative sensitivity in class V restorations. Lasers Med Sci 30:1245–1249
Vichi A, Margvelashvili M, Goracci C, Papacchini F, Ferrari M (2013) Bonding and sealing ability of a new self-adhering flowable composite resin in class I restorations. Clin Oral Investig 17:1497–1506
Wei YJ, Silikas N, Zhang ZT, Watts DC (2011) Hygroscopic dimensional changes of self-adhering and new resin-matrix composites during water sorption/desorption cycles. Dent Mater 27:259–266
Çelik EU, Aka B, Yilmaz F (2015) Six-month clinical evaluation of a self-adhesive flowable composite in noncarious cervical lesions. J Adhes Dent 17:361–368
Kucukyilmaz E, Savas S (2015) Evaluation of different fissure sealant materials and flowable composites used as pit-and-fissure sealants: a 24-month clinical trial. Pediatric Dentistry. Pediatr Dent 37:468–473
Pinna R, Bortone A, Sotgiu G, Dore S, Usai P, Milia E (2015) Clinical evaluation of the efficacy of one self-adhesive composite in dental hypersensitivity. Clin Oral Investig 19:1663–1672
Saba K, Maxood A, Abdullah S, Riaz A, Din SU (2018) Comparison of frequency of post operative sensitivity in amalgam restorations using copal varnish and dentin adhesive liner. J Ayub Med Coll Abbottabad 30:163–166
Hirani RT, Batra R, Kapoor S (2018) Comparative evaluation of postoperative sensitivity in bulk fill restoratives: a randomized controlled trial. J Int Soc Prev Community Dent 8:534–539
Mjor IA (2009) Dentin permeability: the basis for understanding pulp reactions and adhesive technology. Braz Dent 20:316
Hickey D, Sharif O, Janjua F, Brunton PA (2016) Bulk dentine replacement versus incrementally placed resin composite: a randomized controlled clinical trial. J Dent 46:1822
Skovlund E, Breivik H (2016) Analysis of pain-intensity measurements. Scand J Pain 13:123124
Wang L, Magalhães AC, Francisconi-dos-Rios LF, Calabria MP, Araújo DFG, Buzalaf MAR, Pereira JC (2016) Treatment of dentin hypersensitivity using nano-hydroxyapatite pastes: a randomized three-month clinical trial. Oper Dent 41:93–101
Ravishankar P, Viswanath V, Archana D, Keerthi V, Dhanapal S, Lavanya Priya KP (2018) The effect of three desensitizing agents on dentin hypersensitivity: a randomized, split-mouth clinical trial. Indian J Dent Res 29:51–55
Yaylali IE, Kurnaz S, Tunca YM (2018) Maintaining apical patency does not increase postoperative pain in molars with necrotic pulp and apical periodontitis: a randomized controlled trial. J Endod 44:335–340
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
ESM 1
(PDF 106 kb)
Rights and permissions
About this article

Cite this article
de Oliveira, N.G., Lima, A.S.L.C., da Silveira, M.T. et al. Evaluation of postoperative sensitivity in restorations with self-adhesive resin: a randomized split-mouth design controlled study. Clin Oral Invest 24, 1829–1835 (2020). https://doi.org/10.1007/s00784-019-03046-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-019-03046-0