
Abstract
Objectives
The aims of this retrospective longitudinal study were to present the incidence of external apical root resorption (EARR) in the maxillary anterior teeth of patients with complete unilateral cleft lip and palate (CUCLP) and to evaluate the influence of orthodontic treatment variables on the development of EARR.
Material and methods
Forty-one patients with CUCLP participated in the study. Orthopantomograms (OPGs), taken before (T2) treatment with multiband orthodontic appliances (MBA), and periapical radiographs (PAs) of the maxillary anterior teeth taken at the end (T3) of orthodontic treatment (OT) were assessed for EARR.
Results
The incidence of EARR at T3 (97.6%) was considerably higher than at T2 (51.2%). Central incisors and canines on the cleft side showed a significantly higher score (p < 0.01, p < 0.05 respectively) of EARR in comparison to the same group of teeth on the non-cleft side. Preexisting EARR and abnormal root morphology were identified as predisposing factors for EARR.
Conclusions
Patients with CUCLP treated with MBA have higher incidence of EARR on the maxillary anterior teeth of the cleft side. Severe EARR is rather rare but more often seen on central incisors of the cleft side.
Clinical relevance
As most of the patients with cleft lip and palate undergo a challenging and long-term OT with MBA, it is of importance to identify the predisposing factors related to the special anatomical features of the bone and teeth located in the cleft area, as well as the special OT needs of these patients.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
External apical root resorption (EARR) is a common undesirable and unpredictable adverse effect of orthodontic treatment (OT) [1,2,3,4,5,6]. A general agreement is that EARR develops in a certain degree in every orthodontic patient. However, clinical manifestations of EARR in patients subjected to OT under the same regimens vary highly [6]. These interindividual variations seem to indicate the existence of an individual predisposition and a multifactorial etiology [7]. Fortunately, most of the EARR induced after an OT are minor and of no clinical significance [8, 9]. Despite that it is well known how an EARR develops in a cellular or histochemical level, it remains unclear which patients are at a higher risk of developing severe resorptions. Studies on the relationship between patient-related factors and EARR are controversial. Most studies, for example, have found no correlation between sex and EARR [10,11,12,13,14], while others report more severe lesions in female patients [15,16,17,18,19]. Patient’s age [12], endocrinological disorders (like hypothyroidism [15, 20,21,22,23], and estrogen reduced levels [24]) and nutritional factors that influence the bone metabolism, such as calcium (Ca) or vitamin D deficiency [25], have also been associated to EARR. One of the most commonly investigated metabolic factors for its effects on EARR are prostaglandins. Previously published studies have supported an increased incidence of EARR after local or systemic administration of prostaglandin E2 (PGE2) [26, 27]. Contrarily, fluoride [28, 29], thyroxine [6, 29], steroids [29], or the simultaneous administration of PGE2 and thyroxine have a protective effect over the development of EARR in animals [27]. Nevertheless, recently published studies found no association between vitamin D deficiency [30], or after administration of PGE2 and Ca and increased incidence of EARR [31].
Further patient-related oral factors predisposing to EARR are preexisting lesions [15, 32], abnormal root morphology [11, 19, 33, 34], and previous trauma [34,35,36,37], especially when trauma was associated with signs of EARR before OT [38]. According to other researchers though, dental trauma was not identified as a risk factor for EARRs associated to orthodontic tooth movement (OTM) [39]. Endodontically treated teeth [2, 40, 41] and those with incomplete root formation [42] seem to have a protective effect over EARR.
When different orthodontic techniques were compared, such as standard edgewise and straight-wire technique [37], aligner, and multiband orthodontic appliances (MBA) [43] or even when different types of brackets were used (e.g., conventional vs. self-ligating brackets), no variation in the EARR was found [14, 44,45,46]. Contrarily, the type of wires used (heavy rectangular steel wires) [47], the use of intermaxillary (class II or anterior vertical) elastics [48], the amount of OTM [49], the force level [50], and overall the duration of the treatment [7, 14, 15, 49, 51, 52] seem to play an important role in the development of this pathology. Finally, yet importantly, certain oral habits (e.g., lip or tongue posture or dysfunction) are also predisposing factors discussed extensively in the existing literature [2, 14, 15, 17, 37, 53,54,55].
Cleft lip and palate (CLP) is the most common orofacial anomaly. The orthodontist has a challenging role in different developmental stages in the management of patients with CLP. Patients with complete unilateral cleft and palate (CUCLP) are usually characterized by an asymmetric and constricted maxillary arch, maxillary midline deviation, inadequate bone, and soft tissue deficiency along the cleft area. Teeth adjacent to the cleft are often ectopic, missing, tipped into the cleft, rotated, or impacted and usually have a special root morphology [56]. All previously mentioned factors result in a more complex OT and subsequently in many cases in a longer treatment duration. Therefore, it is of fundamental importance to evaluate the incidence, severity, and predisposing factors of EARRs in these patients.
To our knowledge, there are only a few studies [36, 56,57,58,59,60] which have presented the possible risk factors and incidence of EARR in patients with CLP treated with orthodontic appliances. Therefore, the main purpose of this study was to investigate EARR of the upper incisors and canines in patients with CUCLP and to evaluate the influence of several patient- and treatment-related variables on its development.
Material and methods
Sample and registration method
The records of 193 patients with different forms of cleft lip and palate (CLP) treated between 1978 and 1997 in the Charité – Universitätsmedizin Berlin were examined. Patients with CUCLP were selected and those with incomplete records were omitted. A total of 41 patients (22 boys, 19 girls) with CUCLP were finally included in this retrospective longitudinal study. Cleft laterality, sex distribution, and diagnostic records available at the different treatment times (T1: start of interceptive OT, T2: start of treatment with MBA, and at T3: completion of OT) are presented in Fig. 1. Patients’ age at T2, as well as the treatment duration with MBA (T2–T3) and total OT time (T1–T3) are presented in Table 1.

Data provided: selection pool for eligible patients, patients with CUCLP included in the study, and patients’ distribution according to sex and cleft laterality. CLP cleft lip and palate, n: number of patients, CUCLP complete unilateral cleft lip and palate, T1 beginning of interceptive orthodontic treatment, OPG orthopantomogram, T2 beginning of treatment with multiband orthodontic appliances (MBA), T3 end of orthodontic treatment
The inclusion criteria for the present study were as follows:
Caucasian ethnic background
All patients were treated with secondary alveolar bone graft (SABG)
No associated congenital malformations, syndromes, or mental deficiency
Defined orthodontic and surgical treatment protocol of the Charité – Universitaetsmedizin Berlin, Campus Mitte (Table 2)
Well-documented OT, including registration of the employed devices, as well as material, size characteristics, and archwire sequence
Complete dental root formation of the anterior maxillary teeth prior to the treatment with MBA
OT with MBA at least in the maxilla with 0.022-in. bracket slot
Orthodontic space closure or prosthodontic rehabilitation on the cleft side or/and the contralateral side
Good quality of X-rays (displaying clear measurements of the whole tooth, including visible root apex) available at two well-defined treatment time points: OPGs at T2 and periapical radiographs (PAs) of the six upper anterior teeth at T3, which were part of the patients’ routine record documentation
Available dental casts, at T1, T2, and T3
In total, 41 patients with CUCLP met the inclusion criteria. All the included patients underwent OT in the early mixed dentition (T1). The main OT goal at T1 was to achieve a symmetric maxillary arch form before the bone grafting. Almost 70% of these patients were treated with maxillary orthodontic appliances, before MBA. These were removable orthodontic appliances with lateral bite planes and expansion or Bertoni screws for transversal, and in some case, sagittal arch expansion and proclination or derotation of the upper incisors (T1). Eleven patients (26.83%) were treated with fixed expansion appliances (quad-helix or rapid maxillary expansion devices). Besides the expansion devices, extra-oral appliances such as chin cup and face mask were used in ten patients (24.39%), for the early correction of Cl lll malocclusion (T1–T2). In several occasions, a serial extraction protocol for guided tooth eruption was used. Fifteen patients (36.58%) were treated with premolar extraction in the maxilla and mandible due to asymmetric agenesis of upper lateral incisors or second premolars.
Of the included patients, a total of 175 maxillary anterior teeth were well documented and evaluated for EARR. OPGs at T2 and PA radiographs at T3 available for all patients were assessed for EARR. The distribution of the evaluated teeth on the cleft and non-cleft side is presented in Table 3. Well-trained dental assistants performed all radiographs. All the available OPGs were taken using a standardized technique and with the same rotation axis for each patient according to the instructions of the manufacturer (Orthoralix SD, Philips, 66–70 kV, 14 mA and 12 s exposure time). The posttreatment PA X-rays of the upper six anterior teeth (incisors and canines) were made following the long-cone paralleling technique. The X-ray film was positioned parallel to the long axis of the teeth, so that magnification or distortion could be minimized.
OPGs at T2 were first used for the subjective evaluation of the root configuration and anatomic variations (blunt, eroded, pointed, bent, or bottle-shaped roots) of the anterior teeth. Duplicates of the OPGs were then cut centrally and numbered randomly to ensure that the contralateral side of the X-ray was not visible at the time of the evaluation. Finally, the duplicates of OPGs (at T2) and PA X-rays (at T3) were projected on a wall at × 10 magnification and then assessed for the existence of EARR by the Malmgren et al. scoring system [38, 51]. The scoring index is ranging from 0 to 4. Score 0 represents normal apical root contour with no visible erosions or root resorption. Score 1 represents irregular apical root contour but with no signs of root reduction. Score 2 is given in EARR ≤ 2 mm and score 3 for EARR amounting from 2 mm to 1/3 of the initial root length. Score 4 is assigned for EARR > 1/3 of the initial root length [38, 51].
Linear measurements of posttreatment tooth length (Online Resource 1) were taken on the magnified images using a transparent metric ruler in millimeters. The ruler was held along the long axis of the tooth, following the pulp canal. The measurements were made from the incisal edge to the root apex to the nearest 1.0 mm (equivalent to 0.1 mm on the radiograph) [2, 40, 41].
Oral habits (tongue thrust, thumb sucking, nail biting) were recorded in the patients’ medical history, but only considered in this study if they persisted beyond the age of 8 years. The use of intermaxillary elastics and their wear time was also registered.
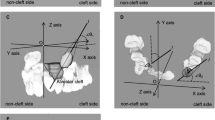
The direction and amount of tooth movement were reconstructed with the patients’ dental casts by a 3D-computer supported reflex microscope (Reflex Measurement Ltd., Hadley House, Water Lane, Butleigh, Somerset, BA6 8SP). The intertuberosity line served as reference line. The right tuberosity was set as starting point for the coordination system employed to register the tooth movement. Movements in bucco-palatal and mesio-distal direction, as well as rotations were recorded from T1 to T3. Vertical movements and torque were not registered.
Method error
For the assessment of the intra-rater reliability, dental casts and X-rays of 20 randomly selected patients were measured twice in a 4-week interval by the same observer. The intra-rater reliability for the different variables (tooth length, resorption score, amount of tooth movement) was calculated by the Dahlberg formula [61]. The results showed no significant systematic error between the double measurements.
A total agreement was found between the double measurements of the lateral incisors on the cleft side. For all other tooth groups, the correlation between the first and second measurement was at least 0.992 (p < 0.001).
Additionally, the reproducibility of the measurements according to Malmgren’s scoring index [38] was assessed for 92 teeth. In 82 teeth (89.1%) the double measurements were identical. In the remaining ten teeth (10.9%), differences in the assigned scores were found as follows: 4.3% were between the score 0–1, and 3.3% between the score 1–2 and 2–3. In case of inconsistency, the highest score of resorption and the mean value in the tooth length measurements were considered in the statistical analysis.
Statistical analysis
The statistical analysis was performed with SPSS (version 6.0; Chicago, Ill). The available data was evaluated separately for each group of teeth. The Wilcoxon test was used to compare EARR in the different tooth groups on the cleft and non-cleft side, at T2 and T3. This test was also employed to compare the posttreatment lengths of the anterior teeth and the total amount of tooth movement on the cleft and non-cleft side (Online Resource 1). The McNemar test was used to assess the incidence of atypical root form. Possible causal relationship between the studied variables and the development of an EARR after an OT with MBA was determined using the chi-square test.
The Mann-Whitney test was carried out to calculate a statistical relationship between the age of the patient at the beginning of treatment (T1), as well as between MBA treatment time (T2–T3), total OT time (T1–T3), amount of orthodontic movement, and incidence of an EARR of at least 2 mm (score 2–4).
A multiple linear and a logistic regression analysis was performed to identify predictors related to the observed posttreatment EARRs. For the first analysis, an EARR of at least 2 mm was set as dependent variable. The posttreatment EARR scores at T3 and the maximum amount of EARR in each patient were set as dependent variables for the second and third regression analysis, respectively. Furthermore, the Pearson correlation coefficient was calculated to investigate a possible relationship between the different studied variables.
Results
Twenty-one of the patients (51.2%) showed EARR at least in one of the evaluated anterior teeth at T2. The incidence of EARR was considerably higher (40 patients—97.6%) at T3. Of the 175 total evaluated teeth, 150 teeth (85.7%) presented a score 0 at T2 and only 49 of them (28%) had this score at T3. The vast majority of the evaluated teeth (91.4%) presented a light form of EARR (up to 2 mm—score 0–2). The central incisors were the most affected teeth with 80% of EARR followed by the lateral incisors (69.6%) and the canines (61.2%). Only two patients developed severe EARR on the central incisors of the cleft side (score 4) after MBA treatment. Moderate EARR (score 3) was found in approximately every fourth patient (22%), in at least one of the evaluated teeth. The central incisors and canines on the cleft side showed a significantly higher incidence (p < 0.01, p < 0.05 respectively) of EARR at T3 in comparison to the same group of teeth on the non-cleft side. Lateral incisors showed no statistical significance on the incidence of EARR between cleft and non-cleft side at T3 (p = 0.109). The EARR scores of different tooth groups before and after MBA (T2 and T3) are presented in Table 4.
Preexisting EARR at T2 was correlated to further development of EARR and this was statistically significant for all evaluated teeth (p < 0.05) (Table 5).
The present study also recorded and compared the amount of mean movement (labio-palatal, mesio-distal, and rotational movement) described during the OT in the different tooth groups, and between the cleft and non-cleft side. The teeth located on the cleft side showed a considerably higher amount of OTM when compared with the ones on the contralateral side. The amount of tooth movement on the cleft side was statistically significantly different on the canines, both in a mesio-distal and rotational direction (p < 0.001 and p < 0.01, respectively), as well as on the central and lateral incisors in labio-palatal direction (p < 0.01) when compared to the non-cleft side (Table 6).
Regarding the mean tooth length, the statistical analysis revealed a significant difference in the central and lateral incisor group between the cleft and non-cleft side (p < 0.001 and p < 0.01, respectively, Online Resource 1).
The regression analysis model, with the score of EARR at T3 as dependent variable, revealed that the degree of EARR at T2 was the most predictable variable to assess the risk of further deterioration of the pathology for all evaluated tooth groups (Table 7). The lateral incisors of the cleft side were excluded from this statistical analysis because only 12 of those teeth could be evaluated in the study, and none of them exhibited a preexisting EARR at T2 (Table 5). Thus, the available data for the lateral incisors on the cleft side could not ensure sufficient power to the analysis. Regarding the other variables, patient’s age or sex, and the treatment duration with MBA (T2-T3) do not seem to have an effect over the incidence of EARR (Online Resource 2). On the contrary, total OT time (T1–T3) of the canines (p < 0.05) on the cleft side, as well as the total amount of labio-palatal movement of the lateral incisors (p < 0.01) on the non-cleft side seem to have an effect on the development of EARR at T3 (Table 7).
41.5% of the patients wore intermaxillary elastics, but our study did not find proof of correlation to EARR. An oral habit was registered (most frequently thumb or finger sucking) in 12 out of 41 (29.3%) patients. Nevertheless, no statistically significant correlation of oral habit and EARR could be identified. Similarly, the initial root form neither had statistical significance for the prediction of EARR at T3 (Online Resource 2).
The standardized regression coefficients show the importance of the different variables in the prediction of EARR (Table 7). For instance, our analysis estimates that in the lateral incisors on the non-cleft side, the EARR score at T2 (β = 0.49) has a stronger influence on root resorption than the OTM in labio-palatal (β = 0.43) direction. The highest R2 found in this regression model was 0.43 for the lateral incisors and the canines on the non-cleft side, indicating that only 43% of the EARR is explained by the examined variables. The R2 for the central incisors and the canines of the cleft side is (R2 = 0.20), and for the central incisor on the non-cleft side is even smaller (R2 = 0.12).
When setting the maximum amount of EARR per patient as dependent variable and all other variables as independent, the maximum EARR in each of the examined patients was significantly associated with the EARR at T2 (p = 0.008) (Online Resource 2).
The following equation resulted from this regression analysis and describes the predictive model for the calculation of the maximum amount of EARR per patient:
Posttreatment score (T3) = 1.90 mm + treatment variable × 0.44 × score at T2
Meaning that the maximum amount of EARR is 1.90 mm, if all other independent variables have no effect on the EARR.
Discussion
Apical root resorption is a common undesirable effect of OT. The maxillary incisors have been commonly cited as the most affected teeth [62]. In this study, we aimed to comparatively investigate the risk to which CUCLP patients are subjected regarding the development of EARR in the anterior teeth, either due to patients’ or to OT-related factors.
The limitation of all longitudinal retrospective studies, as this one, is the difficulty to ascertain the role of the multifactorial parameters causing or predisposing to EARRs. The available OPGs at T1 were not used for initial root length evaluation, since the root formation in most of the evaluated maxillary front teeth was not fully completed at this time point. Therefore, EARRs were evaluated on OPGs in all patients at T2 and on periapical (PA) radiographs at T3, which were part of the routine record documentation of these patients. In this case, a two-dimensional (2D) representation of the lesions was only available and therefore changes on the palatal or labial side of the teeth could not be registered. The tooth length was measured along the whole tooth axis and the pulp canal, since this technique has been proved to be more accurate than using the cementoenamel junction as reference line [41, 63]. Even though the paralleling technique has been used as a standardized method for the evaluation of root resorption progress, incisor tipping during OT may influence the reproducibility of this method [62, 64, 65]. Furthermore, EARRs can be underestimated by the radiologic evaluation when compared to a histological examination [66]. The apical root cementum is softer in comparison to the cementum on the cervical or middle part of the root, as it has been presented in a three-dimensional (3D) evaluation [67]. Nevertheless, root resorption craters have been described along the root cementum [68]. Over the last years, cone-beam computed tomography (CBCT) has been recommended for the diagnosis of EARR [44, 50, 69,70,71]. However, CBCT should be considered for EARR evaluation during OT, only if it is already available [62], and always respecting the ALARA (As Low As Reasonably Achievable) principle.
In this study, even though strict inclusion criteria and a well-defined treatment protocol were used in order to control follow-up bias, there are still limitations and confounding factors influencing the final outcome. Individual variables such as systemic diseases, asthma, allergies, and medication that could predispose to EARR were not evaluated in this study. All the interindividual variabilities were though eliminated due to the split-mouth design [72] of this study, where EARRs of the front teeth on the cleft and non-cleft side were compared.
Eligible patients, sex distribution and cleft laterality, as well as records available at the three time points (T1, T2, T3) are presented in Fig. 1. Table 1 shows the mean and range of age of the patients at T2, the time required for treatment with MBA (T2–T3), and the total OT time (T1–T3). Surgical and orthodontic treatment protocol followed at the Charité – Universitaetsmedizin Berlin, Campus Mitte is presented in Table 2. One of the goals of the orthodontist in the treatment of patients with CLP is the presurgical orthodontic preparation in order to achieve symmetry of the arch segments. In this group of patients, the correction of the collapsed arch segments was achieved with removable or fix expansion appliances during the early mixed dentition phase (T1). All patients participated in this study before the eruption of the permanent lateral or the canine, and underwent SABG with autologous bone harvesting from the anterior iliac crest for the stabilization of the alveolar segments and the spontaneous eruption of these teeth in the grafted area (Table 2). The grafted cancellous bone joins anatomically the existing bone and becomes radiographically indistinguishable after approximately 3 months [73]. The OTM on the cleft side can then start actively again through the grafted bone [74]. The incidence of EARR has been investigated in both mature and immature bone. OTM in well-organized bone has a better prognosis for the teeth roots. These data are though based on animal studies investigating bone formation by means of distraction osteogenesis [75] and not in grafted bone.
Teeth in the cleft area are often hypoplastic and exhibit a reduced root length due to insufficient mecenchymal support, surgical procedures in the early tooth developmental stage, and congenital or iatrogenic reduced blood supply.
The distribution of the evaluated front teeth on the cleft and non-cleft side is presented in Table 3. The lateral incisors on the cleft and non-cleft side were not equally distributed. Lateral incisors of the cleft side are the most frequent missing teeth in the CUCLP patients as part of their phenotype [76]. These teeth are sensitive to developmental deviations, and due to shape or size anomalies or tissue insufficiency in the area are often extracted for orthodontic purposes [77, 78]. A considerable number of canines were also excluded due to incomplete root formation. This led to a significant sample size reduction on cleft and non-cleft side (Table 3). Therefore, generalized conclusions for laterals and canines deriving from this study should be cautiously interpreted. On the contrary, the central incisors presented a relatively large and similar distribution on both sides, and sample size, hence, is suitable for statistical analysis.
The tooth length, the EARR [38], and the amount of tooth movement were evaluated in this study. Twenty patients were randomly selected and double measurements were performed. Intra-rater reliability was high. The correlation between first and second measurements was at least κ = 0.992 (p < 0.0001).
The EARR of front maxillary teeth on the cleft and non-cleft side at T2 and T3 has been evaluated according to Malmgren’s scoring index [38] (Table 4).
In various studies, the incidence of EARR in orthodontic patients ranges from 1.8 to 100% [1, 5, 13, 50, 54, 79, 80]. The incidence of EARR found in this study was 97.6%. The most frequently affected teeth were the central incisors (80.0%) followed by the lateral incisors (69.6%) and the canines with 61.2%. Although almost every tooth presented an EARR after the OT, most of them (88.1%) showed resorption scores of 1 or 2 only, which is of no clinical relevance since as already histological studies have shown, all teeth exposed to an orthodontic force application develop a mild degree of EARR [8, 9]. Only 2.2% of all evaluated teeth had EARR of score 4. The very low incidence of severe root resorption after OT is a common believe of many studies over the last decades [41, 50, 51, 53, 54, 64, 81].
In the present study, the most severe EARRs were observed on the cleft side. This was statistically significant for central incisors (p < 0.01) and canines (p < 0.05) (Table 4). Only five out of the 12 included laterals on the cleft side showed an EARR ≥ 2 mm at T3 and none of these teeth presented preexisting EARR at T2 (Table 5). Even if the preserved lateral incisors on the cleft side often present shape deviations, there is no evidence that shows that lateral incisors are at higher risk for EARR [82].
The amount of mesio-distal (mm), labio-palatal (mm), and rotational (degrees) OTM of the evaluated teeth are presented in Table 6. OTM was evaluated on the basis of dental casts, and neither torque nor vertical movements were recorded. Teeth on the cleft side showed a considerably higher amount of OTM in comparison to the ones on the contralateral side. Central incisors on the cleft side are usually severely rotated, retroclined, and often their roots are very close to the cleft [83]. Our statistical analysis showed a significant difference between the total amount of labio-palatal movement of central incisors on the cleft in comparison to the contralateral side (Table 6). Consequently, the magnitude and duration of force application on the cleft side are higher in comparison to the non-cleft side. According to published data, other mechanical factors associated with an increased development of EARR are the point of force application, the position of the center of resistance, the mean force vector, and moments of force [15].
A multiple regression anaylsis model was used for the prediction of EARR at T3 (Table 7). The dependent variable in this model was the EARR according to Malmgren’s scoring index [38] at T3. The lateral incisors on the cleft side were not included in this regression analysis model. The sample size of this teeth group on the cleft side could not ascertain sufficient power to the analysis. Only five of these teeth had EARRs ≥ 2 mm at T3 (Table 7). EARRs of less than 2 mm are within the expected average amount of root resorption after OT [41, 64]. The regression model could not identify a significant association between EARR of central incisors at T3 and the mesio-distal or the labio-palatal OTM. A statistical correlation, though, was found between the labio-palatal crown movement of the lateral incisors on the non-cleft side and the prediction of EARR at T3 (p = 0.005) (Table 7). The laterals on the non-cleft side are frequently severely rotated, and shape deviations both on crown and root are observed more often than in the non-cleft population [84]. Previous studies have shown an association between the total labio-palatal apical displacement and the severity of EARR [41, 80, 85,86,87]. Uncontrolled and torque force application are associated with increased EARR [15]. Furthermore, intrusion forces induce more severe EARR in comparison to the extrusive forces [68]. Tooth derotation and translation were evaluated in a 3D reconstruction model and no association was identified among these OTMs and the EARR [88]. Moreover, a higher risk of EARR has been reported when teeth are moved against the cortical bone [15, 85]. Teeth adjacent to the cleft are surrounded by a thin layer of bone and they are often pressed against the cortical bone when OTM is taking place [60]. Nevertheless, it remains unclear if EARR is caused by a more extensive OTM [2] and not because of the vicinity of the teeth to the cortical bone. A more precise evaluation of the total amount and type of OTM with 3D data may elucidate the influence of this variable on the severity of EARR.
The central incisors on the cleft side at T3 were 9% shorter than the homonym teeth of the contralateral side and this result was statistically significant (p < 0.001). Eighty-two percent of all evaluated front teeth on the cleft side and 64.3% of the controls had some degree of EARR at the end of treatment (T3) (teeth with score 1 were not included, since these teeth only presented contour configuration changes and not root length shortening). Only 11.9% of the evaluated teeth on the cleft side and 6.1% of the non-cleft side had a severe degree (score 3–4) of tooth resorption at T3. Early signs of EARR [12, 53] and initial atypical root form [11, 41, 89] have been considered as risk factors for EARR development during OT, and this was in accordance with our findings (Tables 5 and 7).
The multiple regression analysis showed a positive correlation between preexisting EARR and the development of further lesions over the course of OT for all teeth that have been examined. Based on these results, we could say that the preexisting EARR is a predictive factor for root resorption during the OT and therefore should be carefully evaluated when assessing patient’s individual risks for EARR (Table 7).
The prolonged OT duration with MBA was not identified as a risk factor for EARR in our study (p = 0.515). This may be explained by the fact that treatment time is rather an unspecific variable, which also depends on many factors (e.g., employed mechanics, patient’s compliance, or less OTM in the last stages of OT). The regression analysis showed that the total OT time (T1–T3) has a significant effect (p = 0.018) on the incidence of EARR in the canines of the cleft side.
Even though it has been widely accepted that the overall OT time is a risk factor associated to EARR [5, 11, 49, 85, 89, 90], which was also in accordance with our finding, there are investigators that could not confirm it [2]. Nevertheless, the early identification of patients at risk for EARR is fundamental and can be done by examining PA radiographs of the maxillary incisors after the first 6 months of active OT [39].
Factors affecting the decision-making between space closure and prosthodontic rehabilitation in the area of missing or poorly shaped or displaced laterals are the sagittal discrepancy of the maxilla, the position of the erupting canine, and the shape and size of the lateral on the contralateral side [83, 91].
All the above mentioned criteria were taken into consideration for treatment planning for orthodontic space closure or prosthodontic rehabilitation in this group of patients. The amount and type of OTM was registered for all front teeth, and for this reason, no information about prosthodontic rehabilitation of these patients is provided (Table 6). In addition, the goal of an orthodontist should be to minimize the need for an prosthodontic treatment [83].
The results of this study showed no significant effect on the development of post-therapeutic EARRs after the use of intermaxillary elastics. Even though our findings are in agreement with published data [5, 14, 64, 92, 93], it is still a controversial issue [2, 5, 51, 94]. Severe oral habits have been considered risk factors for EARR [55, 94] but this is also inconclusive [34]. In this group of patients, oral habits after the age of seven were not correlated to EARR.
There are rather inconsistent findings in the literature regarding the treatment variables related to EARR. Patient’s sex was an unreliable predictor for the development of EARR in this study (p = 0.923), which has been verified in previous published data [12, 53, 92, 95]. Despite many current studies focusing on EARR, great difficulties are still present in the identification of the predisposing factors. It has been stated that the individual predisposing factors are paying the major role in this pathology and not the OT-related factors [79]. Medical history [96, 97], medication [98, 99], genetics, and immune system [100, 101] have been investigated in patients prone to EARR in order to solve the puzzle of the role of the genome in this pathology.
High levels of salivary IgA (sIgA) in human-dentine-extract (HDE) have also been correlated to a higher incidence of root resorption [102]. It has been suggested that an analysis of the sIgA level [102], a DNA examination (e.g., variations in the interleukin 1-RN) [33], or the determination of different biologic molecules that are associated to EARR should be performed before an OT. This suggestion, though, has not been established in the routine clinical orthodontic practice.
The low bone metabolism has also been associated with an increased risk for EARR [20]. Diseases (osteoporosis, hyperthyroidism, etc.), or medication (bisphosphonates, estrogen hormone therapy, etc.) that decrease the bone turnover should be registered. The biochemical profile of the patients could prevent complications related to the OT. The extrapolation of results derived from experimental animal studies in humans should be considered with caution [103], and further clinical trials are still required for a better understanding of EARR at the molecular level [31].
More accurate and standardized measuring methods and long-term multicenter prospective studies are needed in order to clarify the influences of patient-related factors and treatment variables in the development of EARR and help us to overcome the small population studies. Early signs of EARR and predisposing factors should be carefully evaluated before and during the OT.
Conclusions
According to the findings of this study we could say:
- 1.
EARRs developed after an OT with fixed appliances are more severe and frequently observed on the central incisor of the cleft side.
- 2.
Pretherapeutic EARRs had a significant influence on the development of post-therapeutic EARRs on both cleft and non-cleft side.
- 3.
Abnormal root morphology was not among the risk factors for EARRs.
- 4.
Most EARRs developed during the OT were of less than 2 mm and therefore of no clinical relevance.
References
Lund H, Grondahl K, Hansen K, Grondahl HG (2012) Apical root resorption during orthodontic treatment. A prospective study using cone beam CT. Angle Orthod 82(3):480–487. https://doi.org/10.2319/061311-390.1
Mirabella AD, Artun J (1995) Risk factors for apical root resorption of maxillary anterior teeth in adult orthodontic patients. Am J Orthod Dentofac Orthop 108:48–55. https://doi.org/10.1016/S0889-5406(95)70065-X
Kocadereli I, Yesil TN, Veske PS, Uysal S (2011) Apical root resorption: a prospective radiographic study of maxillary incisors. Eur J Dent 5(3):318–323
Jatania A, Shivalinga BF, Kiran J (2012) Root resorption after orthodontic treatment: a review. Int J Orthod Milwaukee 23(2):45–49
Motokawa M, Sasamoto T, Kaku M, Kawata T, Matsuda Y, Terao A, Tanne K (2012) Association between root resorption incident to orthodontic treatment and treatment factors. Eur J Orthod 34(3):350–356. https://doi.org/10.1093/ejo/cjr018
Poumpros E, Loberg E, Engstrom C (1994) Thyroid function and root resorption. Angle Orthod 64:389–393
Sharab LY, Morford LA, Dempsey J, Falcão-Alencar G, Mason A, Jacobson E, Kluemper GT, Macri JV, Hartsfield JK (2015) Genetic and treatment-related risk factors associated with external apical root resorption (EARR) concurrent with orthodontia. Orthod Craniofacial Res 18(S1):71–82. https://doi.org/10.1111/ocr.12078
Roscoe M, Meira J, Cattaneo P (2015) Association of orthodontic force system and root resorption: a systematic review. Am J Orthod Dentofac Orthop 147(5):610–626. https://doi.org/10.1016/j.ajodo.2014.12.026
Remington D, Joondeph DR, Artun J, Riedel R, Chapko M (1989) Long-term evaluation of root resorption occuring during orthodontic treatment. Am J Orthod Dentofac Orthop 96:43–46. https://doi.org/10.1016/0889-5406(89)90227-8
Harris EF, Kineret SE, Tolley EA (1997) A heritable component for external apical root resorption in patients treated orthodontically. Am J Orthod Dentofac Orthop 111:301–309. https://doi.org/10.1016/S0889-5406(97)70189-6
Sameshima GT, Sinclair PM (2001) Predicting and preventing root resorption: part 1. Diagnostic factors. Am J Orthod Dentofac Orthop 119:505–510. https://doi.org/10.1067/mod.2001.113409
Jiang RP, McDonald JP, Fu M (2010) Root resorption before and after orthodontic treatment: a clinical study of contributory factors. Eur J Orthod 32(6):693–697. https://doi.org/10.1093/ejo/cjp165
Phillips JR (1955) Apical root resorption under orthodontic therapy. Angle Orthod 25(1):1–22
Pandis N, Nasika M, Polychronopoulou A, Eliades T (2008) External apical root resorption in patients treated with conventional and self-ligating brackets. Am J Orthod Dentofac Orthop 134(5):646–651. https://doi.org/10.1016/j.ajodo.2007.01.032
Brezniak N, Wasserstein A (1993) Root resorption after orthodontic treatment: part 2. Literature review. Am J Orthod Dentofac Orthop 103:138–146. https://doi.org/10.1016/S0889-5406(05)81763-9
Dougherty HL (1968) The effect of mechanical forces upon the mandibular buccal segments during orthodontic treatment. Am J Orthod 54(2):83–103
Newman WG (1975) Possible etiologic factors in external root resorption. Am J Orthod 67(5):522–539
Kinsella P (1971) Some aspects of root resorption in orthodontics. N Z Orthod J:21-25
Kjær I (1995) Morphological characteristics of dentitions developing excessive root resorption during orthodontic treatment. Eur J Orthod 17(1):25–34. https://doi.org/10.1093/ejo/17.1.25
Verna C, Dalstra M, Melsen B (2003) Bone turnover rate in rats does not influence root resorption induced by orthodontic treatment. Eur J Orthod 25(4):359–363. https://doi.org/10.1093/ejo/25.4.359
Vázquez-Landaverde LA, Rojas-Huidobro R, Alonso Gallegos-Corona M, Aceves C (2002) Periodontal 5′-deiodination on forced-induced root resorption-the protective effect of thyroid hormone administration. Eur J Orthod 24(4):363–369. https://doi.org/10.1093/ejo/24.4.363
Becks H (1939) Orthodontic prognosis: evaluation of routine dentomedical examinations to determine “good and poor risks”. Am J Orthod Oral Surg 25(7):610–624. https://doi.org/10.1016/S0096-6347(39)90061-X
Becks H, Cowden RC (1942) Root resorptions and their relation to pathologic bone formation: part II. Classification, degrees, prognosis and frequency. Am J Orthod Oral Surg 28(8):513–526. https://doi.org/10.1016/S0096-6347(42)90327-2
Sirisoontorn I, Hotokezaka H, Hashimoto M, Gonzales C, Luppanapornlarp S, Darendeliler M, Yoshida N (2012) Orthodontic tooth movement and root resorption in ovariectomized rats treated by systemic administration of zoledronic acid. Am J Orthod Dentofac Orthop 141(5):563–573. https://doi.org/10.1016/j.ajodo.2011.11.016
Goldie RS, King GJ (1984) Root resorption and tooth movement in orthodontically treated, calcium-deficient, and lactating rats. Am J Orthod 85(5):424–430. https://doi.org/10.1016/0002-9416(84)90163-5
Brudvik P, Rygh P (1991) Root resorption after local injection of prostaglandin E2 during experimental tooth movement. Eur J Orthod 13:255–263. https://doi.org/10.1093/ejo/13.4.255
Seifi M, Eslami B, Saffar AS (2003) The effect of prostaglandin E2 and calcium gluconate on orthodontic tooth movement and root resorption in rats. Eur J Orthod 25(2):199–204. https://doi.org/10.1093/ejo/25.2.199
Gonzales C, Hotokezaka H, Karadeniz E, Miyazaki T, Kobayashi E, Darendeliler MA, Yoshida N (2011) Effects of fluoride intake on orthodontic tooth movement and orthodontically induced root resorption. Am J Orthod Dentofac Orthop 2(139):196–205. https://doi.org/10.1016/j.ajodo.2009.05.029
Haugland L, Kristensen KD, Lie SA, Vandevska-Radunovic V (2018) The effect of biologic factors and adjunctive therapies on orthodontically induced inflammatory root resorption: a systematic review and meta-analysis. Eur J Orthod 29. doi: https://doi.org/10.1093/ejo/cjy003
Tehranchi A, Sadighnia A, Younessian F, Abdi AH, Shirvani A (2017) Correlation of vitamin D status and orthodontic-induced external apical root resorption. Dent Res J (Isfahan) 14(6):403–411
Spoerri A, Koletsi D, Eliades T (2018) Intrinsic hormone-like molecules and external root resorption during orthodontic tooth movement. A systematic review and meta-analysis in preclinical in-vivo research. Front Physiol 9:303. https://doi.org/10.3389/fphys.2018.00303
Massler M, Malone AJ (1954) Root resorption in human permanent teeth. Am J Orthod 40:619–633
Al-Qawasmi RA, Hartsfield JK, Everett ET, Flury L, Liu L, Foroud TM, Macri JV, Roberts WE (2003) Genetic predisposition to external apical root resorption. Am J Orthod Dentofac Orthop 123(3):242–252. https://doi.org/10.1067/mod.2003.42
Nanekrungsan K, Patanaporn V, Janhom A, Korwanich N (2012) External apical root resorption in maxillary incisors in orthodontic patients: associated factors and radiographic evaluation. Imaging Sci Dent 42(3):147–154. https://doi.org/10.5624/isd.2012.42.3.147
Brezniak N, Wasserstein A (1993) Root resorption after orthodontic treatment: part 1. Literature review. Am J Orthod Dentofac Orthop 103(1):62–66. https://doi.org/10.1016/0889-5406(93)70106-X
Cardinal L, da Rosa ZG, Mendes FM, Andrade I, Oliveira DD, Dominguez GC (2018) The impact of rapid maxillary expansion on maxillary first molar root morphology of cleft subjects. Clin Oral Investig 22(1):369–376. https://doi.org/10.1007/s00784-017-2121-3
Mavragani M, Vergari A, Selliseth NJ, Bøe OE, Wisth PL (2000) A radiographic comparison of apical root resorption after orthodontic treatment with a standard edgewise and a straight-wire edgewise technique. Eur J Orthod 22(6):665–674. https://doi.org/10.1093/ejo/22.6.665
Malmgren O, Goldson L, Hill C, Orwin A, Petrini L, Lundberg M (1982) Root resorption after orthodontic treatment of traumatized teeth. Am J Orthod 82(6):487–491. https://doi.org/10.1016/0002-9416(82)90317-7
Smale I, Artun J, Behbehani F, Doppel D, van't Hof M, Kuijpers-Jagtman AM (2005) Apical root resorption 6 months after initiation of fixed orthodontic appliance therapy. Am J Orthod Dentofac Orthop 128(1):57–67. https://doi.org/10.1016/j.ajodo.2003.12.030
Spurrier SW, Hall SH, Joondeph DN, Shapiro PA, Riedel RA (1990) A comparison of apical root resorption during orthodontic treatment in endodontically treated and vital teeth. Am J Orthod Dentofac Orthop 97:1304. https://doi.org/10.1016/0889-5406(90)70086-R
Mirabella AD, Artun J (1995) Prevalence and severity of apical root resorption of maxillary anterior teeth in adult orthodontic patients. Eur J Orthod 17(2):93–99
Rosenberg HN (1972) An evaluation of the incidence and amount of apical root resorption and dilaceration occuring in orthodontically treated teeth, having incompletely formed roots at the beginning of Begg treatment. Am J Orthod 61:524–525
Iglesias-Linares A, Sonnenberg B, Solano B, Yañez-Vico R-M, Solano E, Lindauer SJ, Flores-Mir C (2017) Orthodontically induced external apical root resorption in patients treated with fixed appliances vs removable aligners. Angle Orthod 87(1):3–10. https://doi.org/10.2319/02016-101.1
Aras I, Unal I, Huniler G, Aras A (2018) Root resorption due to orthodontic treatment using self-ligating and conventional brackets. J Orofac Orthop 79(3):181–190. https://doi.org/10.1007/s00056-018-0133-5
Jacobs C, Gebhardt PF, Jacobs V, Hechtner M, Meila D, Wehrbein H (2014) Root resorption, treatment time and extraction rate during orthodontic treatment with self-ligating and conventional brackets. Head Face Med 10(1):2. https://doi.org/10.1186/1746-160x-10-2
Leite V, Conti AC, Navarro R, Almeida M, Oltramari-Navarro P, Almeida R (2012) Comparison of root resorption between self-ligating and conventional preadjusted brackets using cone beam computed tomography. Angle Orthod 82(6):1078–1082. https://doi.org/10.2319/080911-501.1
Alzahawi K, Færøvig E, Brudvik P, Bøe OE, Mavragani M (2014) Root resorption after leveling with super-elastic and conventional steel arch wires: a prospective study. Prog Orthod 15(1):35. https://doi.org/10.1186/s40510-014-0035-z
Simplicio H, da Silva JS, Caldas SG, dos Santos-Pinto A (2012) External apical root resorption in retracted incisors. Orthodontics (Chic) 13(1):86–93
Fox N (2005) Longer orthodontic treatment may result in greater external apical root resorption. Evid Based Dent 6(1):21. https://doi.org/10.1038/sj.ebd.6400304
Weltman B, Vig KWL, Fields HW, Shanker S, Kaizar EE (2010) Root resorption associated with orthodontic tooth movement: a systematic review. Am J Orthod Dentofac Orthop 137(4):462–476. https://doi.org/10.1016/j.ajodo.2009.06.021
Levander E, Malmgren O (1988) Evaluation of the risk of root resorption during orthodontic treatment: a study of upper incisors. Eur J Orthod 10(1):30–38. https://doi.org/10.1093/ejo/10.1.30
Pereira S, Lavado N, Nogueira L, Lopez M, Abreu J, Silva H (2014) Polymorphisms of genes encoding P2X7R, IL-1B, OPG and RANK in orthodontic-induced apical root resorption. Oral Dis 20(7):659–667. https://doi.org/10.1111/odi.12185
Lopatiene K, Dumbravaite A (2008) Risk factors of root resorption after orthodontic treatment. Stomatologija 10(3):89–95
Maués CPR, do Nascimento RR, Vilella OV (2015) Severe root resorption resulting from orthodontic treatment: prevalence and risk factors. Dental Press J Orthod 20(1):52–58. https://doi.org/10.1590/2176-9451.20.1.052-058.oar
Odenrick L, Brattström V (1985) Nailbiting: frequency and association with root resorption during orthodontic treatment. Br J Orthod 12(2):78–81
Dewinter G, Quirynen M, Heidbuchel K, Verdonck A, Willems G, Carels C (2003) Dental abnormalities, bone graft quality, and periodontal conditions in patients with unilateral cleft lip and palate at different phases of orthodontic treatment. Cleft Palate Craniofac J 40(4):343–350. https://doi.org/10.1597/1545-1569_2003_040_0343_dabgqa_2.0.co_2
Mao L-X, Shen G-F, Fang B, Xia Y-H, Ma X-H, Wang B (2013) Bone grafting, corticotomy, and orthodontics: treatment of cleft alveolus in a Chinese cohort. Cleft Palate Craniofac J 50(6):662–670. https://doi.org/10.1597/12-034r
Lee KS, Straja SR, Tuncay OC (2003) Perceived long-term prognosis of teeth with orthodontically resorbed roots. Orthod Craniofacial Res 6(3):177–191. https://doi.org/10.1034/j.1600-0544.2003.02276.x
Bergland O, Semb G, Abyholm F, Borchgrevink H, Eskeland G (1986) Secondary bone grafting and orthodontic treatment in patients with bilateral complete clefts of the lip and palate. Ann Plast Surg 17(6):460–474
Maeda-Iino A, Furukawa M, Kwon S, Marutani K, Nakagawa S, Fuchigami T, Nakamura N, Miyawaki S (2017) Evaluation of maxillary central incisors on the noncleft and cleft sides in patients with unilateral cleft lip and palate—part 2: relationship between root resorption, horizontal tooth movement, and quantity of grafted autogenous bone. Angle Orthod 87(6):863–870. https://doi.org/10.2319/031317-189.1
Dahlberg G (1940). In: Statistical methods for medical and biological students. George Allen and Unwin Ltd., London
Barros SE, Janson G, Chiqueto K, Baldo VO, Baldo TO (2017) Root resorption of maxillary incisors retracted with and without skeletal anchorage. Am J Orthod Dentofac Orthop 151(2):397–406. https://doi.org/10.1016/j.ajodo.2016.06.048
Brice GL, Sampson WJ, Sims MR (1991) An ultrastructural evaluation of the relationship between epithelial rests of Malassez and orthodontic root resorption and repair in man. Aust Orthod J 12(2):90–94
Årtun J, Van’t Hullenaar R, Doppel D, Kuijpers-Jagtman AM (2009) Identification of orthodontic patients at risk of severe apical root resorption. Am J Orthod Dentofac Orthop 135(4):448–455. https://doi.org/10.1016/j.ajodo.2007.06.012
Chan E, Darendeliler MA (2006) Physical properties of root cementum: part 7. Extent of root resorption under areas of compression and tension. Am J Orthod Dentofac Orthop 129(4):504–510. https://doi.org/10.1016/j.ajodo.2004.12.018
Alamadi E, Alhazmi H, Hansen K, Lundgren T, Naoumova J (2017) A comparative study of cone beam computed tomography and conventional radiography in diagnosing the extent of root resorptions. Prog Orthod 18(1):37. https://doi.org/10.1186/s40510-017-0191-z
Malek S, Darendeliler MA, Swain MV (2001) Physical properties of root cementum: part I. A new method for 3-dimensional evaluation. Am J Orthod Dentofac Orthop 120(2):198–208. https://doi.org/10.1067/mod.2001.114535
Han G, Huang S, Hoff JWV, Zeng X, Kuijpers-Jagtman AM (2005) Root resorption after orthodontic intrusion and extrusion. Angle Orthod 75(6):912–918. https://doi.org/10.1043/0003-3219(2005)75[912:RRAOIA]2.0.CO;2
Dudic A, Giannopoulou C, Leuzinger M, Kiliaridis S (2009) Detection of apical root resorption after orthodontic treatment by using panoramic radiography and cone-beam computed tomography of super-high resolution. Am J Orthod Dentofac Orthop 135(4):434–437. https://doi.org/10.1016/j.ajodo.2008.10.014
Makedonas D, Lund H, Hansen K (2013) Root resorption diagnosed with cone beam computed tomography after 6 months and at the end of orthodontic treatment with fixed appliances. Angle Orthod 83(3):389–393. https://doi.org/10.2319/042012-332.1
Grünheid T, Kolbeck Schieck JR, Pliska BT, Ahmad M, Larson BE (2012) Dosimetry of a cone-beam computed tomography machine compared with a digital x-ray machine in orthodontic imaging. Am J Orthod Dentofac Orthop 141(4):436–443. https://doi.org/10.1016/j.ajodo.2011.10.024
Pandis N, Walsh T, Polychronopoulou A, Katsaros C, Eliades T (2013) Split-mouth designs in orthodontics: an overview with applications to orthodontic clinical trials. Eur J Orthod 35(6):783–789. https://doi.org/10.1093/ejo/cjs108
Hall HD, Posnick JC (1983) Early results of secondary bone grafts in 106 alveolar clefts. J Oral Maxillofac Surg 41(5):289–294. https://doi.org/10.1016/0278-2391(83)90295-1
da Silva Filho OG, Teles SG, Ozawa TO, Filho LC (2000) Secondary bone graft and eruption of the permanent canine in patients with alveolar clefts: literature review and case report. Angle Orthod 70(2):174–178
Nakamoto N, Nagasaka H, Daimaruya T, Takahashi I, Sugawara J, Mitani H (2002) Experimental tooth movement through mature and immature bone regenerates after distraction osteogenesis in dogs. Am J Orthod Dentofac Orthop 121(4):385–395. https://doi.org/10.1067/mod.2002.122368
Bartzela TN, Carels CEL, Bronkhorst EM, Jagtman AMK (2013) Tooth agenesis patterns in unilateral cleft lip and palate in humans. Arch Oral Biol 58(6):596–602. https://doi.org/10.1016/j.archoralbio.2012.12.007
Boehn A (1963) Dental anomalies in harelip and cleft palate. Acta Odontol Scand 21(SUPPL38):1–109
Hansen K, Mehdinia M (2002) Isolated soft tissue cleft lip: the influence on the nasal cavity and supernumerary laterals. Cleft Palate Craniofac J 39(3):322–326. https://doi.org/10.1597/1545-1569_2002_039_0322_istclt_2.0.co_2
Owman-Moll P (1995) Orthodontic tooth movement and root resorption with special reference to force magnitude and duration. A clinical and histological investigation in adolescents. Swed Dent J Suppl 105:1–45
DeShields RW (1969) A study of root resorption in treated class II, division I malocclusions. Angle Orthod 39(4):231–245
Nieto-Nieto N, Solano JE, Yañez-Vico R (2017) External apical root resorption concurrent with orthodontic forces: the genetic influence. Acta Odontol Scand 75(4):280–287. https://doi.org/10.1080/00016357.2017.1294260
Kook Y-A, Park S, Sameshima GT (2003) Peg-shaped and small lateral incisors not at higher risk for root resorption. Am J Orthod Dentofac Orthop 123(3):253–258. https://doi.org/10.1067/mod.2003.81
Semb G, Ramstad T (1999) The influence of alveolar bone grafting on the orthodontic and prosthodontic treatment of patients with cleft lip and palate. Dent Update 26(2):60–64. https://doi.org/10.12968/denu.1999.26.2.60
Tortora C, Meazzini MC, Garattini G, Brusati R (2008) Prevalence of abnormalities in dental structure, position, and eruption pattern in a population of unilateral and bilateral cleft lip and palate patients. Cleft Palate Craniofac J 45(2):154–162. https://doi.org/10.1597/06-218.1
Kaley J, Phillips C (1991) Factors related to root resorption in edgewise practice. Angle Orthod 61(2):125–132
Baumrind S, Korn EL, Boyd RL (1996) Apical root resorption in orthodontically treated adults. Am J Orthod Dentofac Orthop 110(3):311–320. https://doi.org/10.1016/S0889-5406(96)80016-3
Hollender L, Rönnerman A, Thilander B (1980) Root resorption, marginal bone support and clinical crown length in orthodontically treated patients. Eur J Orthod 2(4):197–205. https://doi.org/10.1093/ejo/2.4.197-a
Guo Y, He S, Gu T, Liu Y, Chen S (2016) Genetic and clinical risk factors of root resorption associated with orthodontic treatment. Am J Orthod Dentofac Orthop 150(2):283–289. https://doi.org/10.1016/j.ajodo.2015.12.028
Årtun J, Smale I, Behbehani F, Doppel D, Hof MV, Kuijpers-Jagtman AM (2005) Apical root resorption six and 12 months after initiation of fixed orthodontic appliance therapy. Angle Orthod 75(6):919–926. https://doi.org/10.1043/0003-3219(2005)75[919:Arrsam]2.0.Co;2
Mohandesan H, Ravanmehr H, Valaei N (2007) A radiographic analysis of external apical root resorption of maxillary incisors during active orthodontic treatment. Eur J Orthod 29(2):134–139. https://doi.org/10.1093/ejo/cjl090
Freitas JA, Garib DG, Oliveira M, Lauris Rde C, Almeida AL, Neves LT, Trindade-Suedam IK, Yaedu RY, Soares S, Pinto JH (2012) Rehabilitative treatment of cleft lip and palate: experience of the Hospital for Rehabilitation of Craniofacial Anomalies-USP (HRAC-USP)—part 2: J Appl Oral Sci 20(2):268–281
Patel N, Currier GF, Kadioglu O, Kierl JP, Skaggs VJ (2012) A CBCT comparison of anterior root resorption in SureSmile and conventional edgewise treatments. Orthodontics (Chic) 13(1):100–109
Janson GRP, de Luca CG, Martins DR, Henriques JFC, de Freitas MR (2000) A radiographic comparison of apical root resorption after orthodontic treatment with 3 different fixed appliance techniques. Am J Orthod Dentofac Orthop 118(3):262–273. https://doi.org/10.1067/mod.2000.99136
Linge L, Linge BO (1991) Patient characteristics and treatment variables associated with apical root resorption during orthodontic treatment. Am J Orthod Dentofac Orthop 99(1):35–43. https://doi.org/10.1016/S0889-5406(05)81678-6
Jung Y-H, Cho B-H (2011) External root resorption after orthodontic treatment: a study of contributing factors. Imaging Sci Dent 41(1):17–21. https://doi.org/10.5624/isd.2011.41.1.17
Nishioka M, Ioi H, Nakata S, Nakasima A, Counts A (2006) Root resorption and immune system factors in the Japanese. Angle Orthod 76(1):103–108
Iglesias-Linares A, Morford LA, Hartsfield JK (2016) Bone density and dental external apical root resorption. Curr Osteoporos Rep 14(6):292–309. https://doi.org/10.1007/s11914-016-0340-1
Gonzales C, Hotokezaka H, Matsuo K-I, Shibazaki T, Yozgatian JH, Darendeliler MA, Yoshida N (2009) Effects of steroidal and nonsteroidal drugs on tooth movement and root resorption in the rat molar. Angle Orthod 79(4):715–726. https://doi.org/10.2319/072108-381.1
Liu L, Igarashi K, Haruyama N, Saeki S, Shinoda H, Mitani H (2004) Effects of local administration of clodronate on orthodontic tooth movement and root resorption in rats. Eur J Orthod 26(5):469–473
Silva LB, Guimaraes CS, Santos RA (2008) Immunology of root resorption: a literature review. Indian J Dent Res 19(4):340–343
van der Veen FJ, van Hagen JM, Berkhof J, Don Griot JP (2006) Regional underreporting of associated congenital anomalies in cleft patients in the Netherlands. Cleft Palate Craniofac J 43(6):710–714. https://doi.org/10.1597/05-179
Ramos SP, Ortolan GO, Dos Santos LM, Tobouti PL, Hidalgo MM, Consolaro A, Itano EN (2011) Anti-dentine antibodies with root resorption during orthodontic treatment. Eur J Orthod 33(5):584–591. https://doi.org/10.1093/ejo/cjq145
Bartzela T, Türp JC, Motschall E, Maltha JC (2009) Medication effects on the rate of orthodontic tooth movement: a systematic literature review. Am J Orthod Dentofac Orthop 135(1):16–26. https://doi.org/10.1016/j.ajodo.2008.08.016
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors. Appropriate Institutional Review Boards and Subcommittee Reviews at Charité Universitätsmedizin Berlin approved the study (EA2/045/16).
Informed consent
For this type of study, formal consent is not required.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
ESM 1
(DOCX 15 kb)
Rights and permissions
About this article

Cite this article
Bartzela, T.N., Mang de la Rosa, M., Wolf, K. et al. Apical root resorption after orthodontic treatment in patients with unilateral cleft lip and palate. Clin Oral Invest 24, 1807–1819 (2020). https://doi.org/10.1007/s00784-019-03044-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-019-03044-2