
Abstract
Objectives
This study evaluated the influence of cavity depth on polymerization shrinkage of bulk-fill resin composites with and without adhesive resin.
Materials and methods
Standardized box-shaped cavities (width, 4 mm; length, 5 mm, depth, 2 mm or 4 mm) were made on occlusal surfaces of extracted human third molars (N = 60). The teeth were assigned to 3 groups to receive bulk-fill resin composites (low-viscosity bulk-fill, SDR; high-viscosity bulk-fill; Filtek Bulk-Fill—FB; and TetricEvo Ceram Bulk-Fill—TB) in the prepared cavities with and without adhesive resin (Clearfil S3 Bond). Each specimen (n = 5 per group) was scanned twice using microcomputed tomography (micro-CT): once after application of the resin composite to the cavity prior to polymerisation and once after polymerisation. The shrinkage of volumetric loss (%) was measured using micro-CT. Data were analysed using Kruskal-Wallis and Mann-Whitney U tests (alpha = 0.05).
Results
The material type (p < 0.05), application of adhesive resin (p < 0.05) and cavity depth (p < 0.05) significantly affected the shrinkage values. The interaction terms were also significant (p < 0.05). All the bulk-fill resin composites tested showed significantly less shrinkage when applied in cavities with adhesive resin (0.94–2.55) compared with those without (2.01–3.45) (p < 0.05) and presented significantly more shrinkage after polymerisation (p < 0.05). At a 2-mm cavity depth without (2 mm, 2.28; 4 mm, 2.41) and with adhesive (2 mm, 0.94; 4 mm, 1.67), significantly less shrinkage was observed with FB compared with SDR and TB (p < 0.05). At a 4-mm cavity depth without (3.14) and with adhesive (2.55), SDR showed significantly higher shrinkage compared with FB and TB (p < 0.05).
Conclusions
The bulk-fill composites tested presented less shrinkage when used in conjunction with adhesive resin application on dentin. Overall, the low-viscosity bulk-fill resin SDR showed more shrinkage compared with high-viscosity resins tested.
Clinical relevance
Low- or high-viscosity bulk-fill resin composites should be applied on dentin after application of adhesive resin to decrease shrinkage.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
In restorative dentistry, resin-based composite materials allow for minimum loss of tooth substance and offer maximum strength while retaining aesthetic and functional characteristics. In addition to such advantages, polymerisation shrinkage is the most significant problem associated with resin composites. As methacrylate monomers polymerise, van der Waals gaps become narrower due to covalent bonding, resulting in 1.5 to 5% volumetric contraction [1]. Configuration factor (C factor), which is the ratio of the number of bonded to unbonded surfaces, markedly affects the extent and stress of shrinkage. Cavities with a higher C factor and those with larger dimensions present increased polymerisation shrinkage [2].
Polymerisation shrinkage causes several complications, such as a disjunction at the tooth-composite interface [3], enamel cracks [4] and secondary caries. When using conventional resin composites, an incremental layering technique is advised to control the shrinkage, but this technique is time-consuming. Recently, to overcome this limitation, bulk-fill composites have been introduced [5]. The intention with such materials is to allow fabrication of 4- to 5-mm thick resin composite restoration in a single layer and thereby save time. Bulk-fill composites have low polymerisation shrinkage and are thus relatively more useful for patients and clinicians, as claimed by their manufacturers. However, there are no sufficient clinical studies on the use of these materials to date [6], particularly those focusing on the high C factor of cavities.
Since the early 1980s, computed tomography (CT) technologies have gained more importance in preclinical and clinical research. The first X-ray microtomography system was developed by Jim Elliot in the early 1980s, and the first published X-ray microcomputed tomography (micro-CT) images were reconstructed from slices of a small tropical snail with a cross-sectional thickness of approximately 50 μm [7]. Since then, software and hardware features have been significantly improved, enabling clearer image acquisition at reduced cross-sectional thicknesses [8] from approximately 7-mm thickness in conventional CT to 81 μm [9], 34 μm [10] and 12.5 μm [11] in micro-CT. Given the advances in micro-CT, faster acquisition of high-resolution 3D images has become possible even with small objects as it corrects the artefacts caused by air bubbles and provides accurate images regardless of the shape of the object and its position [12]. Today, micro-CT is also used for polymerisation shrinkage measurements with accurate results [13]. Micro-CT results could also enable a better understanding of polymerisation shrinkage stress with respect to the elasticity modulus of materials.
The objective of this study therefore was to investigate the influence of cavity depth and the use of adhesive resin on dentin on the polymerisation shrinkage of bulk-fill resin composites using micro-CT. The null hypothesis tested was that there would be no significant difference in polymerisation shrinkage of bulk-fill materials at 2- or 4-mm cavity depths with and without the use of the adhesive resin.
Materials and methods
Tooth selection and cavity preparation
Recently extracted human third molars (N = 60) were collected after approval of the Ethical Committee of the Istanbul Medipol University, School of Dentistry. To confirm sample size, a power analysis was conducted where Δ was 0.7 and standard deviation was 0.3. Accordingly, the number of specimens determined for 0.80 power at α: 0.05 was n = 4 for each subgroup.
The teeth with intercuspal width and mesiodistal length within a maximum deviation of 10% from their respective specific means (9.5–10.5 mm and 10.5–11.5 mm, respectively) were selected. All teeth were cleaned from hard and soft tissue debris using periodontal ultrasonic scalers (Woodpecker UDS-B, Guilin Woodpecker Medical Instrument Co., China) at 30 kHz by one operator and were stored in distilled water at room temperature (25 °C) before and after cavity preparation.
Standardised box-shaped class I cavities were prepared paying attention that occlusal fissure acts as the midpoint of the width and positioned in the midst the cavity in the mesiodistal length of the teeth (width, 4 mm; length, 5 mm). Half of the teeth received cavities with a depth of 2 mm and the other half 4 mm. Cavities were prepared with round and fissure diamond dental burs (Kerr, CA, USA) underwater cooling by one researcher. Throughout cavity preparation, the dimensions were frequently assessed with a digital calliper with 0.01-mm sensitivity. Cavity depth was also controlled with a periodontal probe. One dental bur was used for preparing six consecutive cavities. Each cavity preparation took approximately 20 min.
Restorative procedures
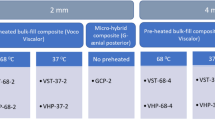
The cavities were randomly assigned to 12 groups (n = 5 per group) according to the adhesion procedures and the filling materials used. In all groups, the cavities were filled with the bulk-fill composite assigned to their group. After adhesive resin (Clearfil S3 Bond, Kuraray Noritake Dental, Tokyo, Japan) application, the cavities were restored with either high-viscosity bulk-fill composites (Filtek Bulk-Fill—FB; 3 M ESPE, St. Paul, MN USA; Tetric EvoCeram Bulk-Fill—TB; Ivoclar Vivadent AG, Liechtenstein) or low-viscosity bulk-fill composite (SDR; Dentsply, York, USA) depending on the assigned group (Table 1). Only Shade A2/U of each composite was used.
Micro-CT imaging
The teeth were kept in dark before photo-polymerisation and micro-CT scans were performed (Skyscan 1172, Bruker, Kontich, Belgium). Each tooth was scanned for approximately 30 min. To ensure that the same amount of resin composite was applied to the cavities in all samples, aluminium reference moulds (2 × 4 × 5 mm3 and 4 × 4 × 5 mm3) were used for 2-mm and 4-mm deep cavities, respectively. After the first scan, each tooth was removed from the scanner using a sample holder and polymerised using a LED photo-polymerization device (BA Optima 10, B.A. International, Northampton, England). Each tooth was placed again in the micro-CT device for a second scan with a reference line over the platform to ensure that the scans are performed exactly from the same position of the tooth.
Each tooth was scanned before and after polymerisation and volumetric shrinkage was calculated. For photo polymerisation, the distance between the light source and the bulk-fill composite was kept at 0.5 mm using a fixed device where the lamp was attached. The duration of polymerization was 20 s, 40 s and 10 s for SDR, TB and FB, respectively.
Overall, 120 micro-CT readings were acquired from 60 scanned teeth. To ensure the stability of each tooth in the device and to maintain a constant distance between the X-ray source and the sample before and after polymerisation, teeth were embedded in silicon impression material (Zetaplus, Zhermack, Badia Polesine, Italy). It was also assured that the cementoenamel junction (CEJ) was over the sample holder. Use of the mould for each sample restricted positional changes while repeating the micro-CT scanning as described earlier [13]. The operating energy (100 Kvp, 100 μA), resolution (16.06 μm/slice) and rotation step (0.5°) for the micro-CT device were kept constant for all samples. The acquired raw images were reconstructed with the software (SkyScan reconstruction program, NRecon, v.1.6.9.4, Bruker) to correct for radiologic artefacts and prepare for analysis. Images were converted to 1000 × 1000 pixel resolution in *.bmp format. Then, the reconstructed images were analysed using the determined processes in the software (Skyscan software CTAn, v. 1.15.4.0, Bruker) according to the following workflow: raw image acquisition, identification of region of interest, binary selection, morphometry and custom processing (Fig. 1a, b). From these data, volumetric loss due to polymerisation shrinkage was calculated as a percentage.

a Operation of region of interest (ROI) constitution; b Operation of binary selection in CTAn analysis programme
Statistical analysis
Statistical analysis was performed using Number Cruncher Statistical System 2007 Statistical Software (UT, USA). Data were expressed as the mean, standard deviation, median, frequency, percentage, minimum and maximum values. Kolmogorov-Smirnov and Shapiro-Wilk tests were used to test normal distribution of the data. As the data were not normally distributed, the Kruskal-Wallis test was used for comparisons of parameters and Mann-Whitney U and Wilcoxon tests were used for pairwise comparisons. A p value of < 0.05 was considered statistically significant in all tests.
Results
Material type (p < 0.05), application of adhesive resin (p < 0.05) and cavity depth (p < 0.05) significantly affected the shrinkage values. Interaction terms were also significant (p < 0.05).
All bulk-fill resin composites tested showed significantly less shrinkage when applied in the cavities with adhesive resin (0.94–2.55) compared with those without (2.01–3.45) (p < 0.05) and presented significantly more shrinkage after polymerisation (p < 0.05) (Table 2).
For all materials tested, volumetric shrinkage after polymerisation was significantly increased compared with the non-polymerised stage (p = 0.001). At 2-mm cavity depth without (2 mm, 2.28; 4 mm, 2.41) and with adhesive (2 mm, 0.94; 4 mm, 1.67), significantly less shrinkage was observed with FB compared with SDR and TB (p < 0.05). At 4-mm cavity depth without (3.14) and with adhesive (2.55), SDR showed significantly increased shrinkage compared with FB and TB (p < 0.05).
When adhesive resin was applied, specimens with 4-mm deep cavities showed higher volumetric loss compared with 2-mm deep cavities. Volumetric loss was significantly higher in SDR and FB than with TB. Representative micro-CT images are presented in Fig. 2a–d.

Representative micro-CT images of horizontal sectional views from the SDR group. a Before polymerisation, b after polymerisation, c magnified view of the relevant region before polymerisation, d magnified view of the relevant region after polymerisation. Note that the resin composite is viewed in white, dentin in black and enamel in grey. Shrinkage can typically be observed in sections where the red arrows indicate increased marginal gap between the composite and the tooth
Discussion
This study assessed the influence of cavity depth and the use of adhesive resin on dentin on the polymerisation shrinkage of bulk-fill resin composites using micro-CT. Since the material type, application of adhesive resin and cavity depth significantly affected the shrinkage values, the null hypothesis was partially rejected.
Use of bulk-fill composites allows for reduced application steps during incremental build-up of resin composites in the cavities, thus reducing a clinician’s operational errors and chairside time. Application of self-etch adhesives also further eases the implementation of bulk-fill composites. However, herein, concerns are present regarding the polymerisation shrinkage severity and shrinkage stress of bulk-fill composites [14, 15]. Typically, for many resin composites, a linear relationship is reported between the polymerisation shrinkage and the associated polymerisation shrinkage stress [16]. Similarly, a direct correlation among polymerisation stress, shrinkage and marginal gap has been previously reported [17, 18]. In this regard, using micro-CT, the consistency of bulk-fill composites applied to class II cavities was demonstrated to affect the internal gap and polymerisation shrinkage where the flowable bulk-fill resin showed less favourable results [19]. Certainly, cavity configuration (C factor), restoration volume and restoration technique significantly affect the polymerisation stress [20, 21]. For instance, cavities with higher C factor have inferior mechanical characteristics due to the higher shrinkage stress [22].
In this study, all bulk-fill resin composites showed shrinkage, and this finding varied depending on the product as volumetric loss was significantly higher in SDR and FB compared with TB. The reason for favourable results with TB could be explained by its chemical composition. Moszner et al. investigated the use of benzoyl germanium derivatives as a novel visible photo initiator and compared these results with other photoinitiators based on benzoyltrimethylgermane (BTMGe) or dibenzoyldiethylgermane (DBDEGe) that are mixed with camphorquinone (CQ) and ethyl 4-(N,N-dimethylamino)benzoate (EMBO) [23]. Accordingly, photo initiators based on BTMGe and DBDEGe showed significantly more intense absorption in the visible region compared with CQ. In our study, TB with the germanium-based initiator showed the lowest polymerisation shrinkage in 4-mm deep cavities although the time of exposure to light was the least among all tested bulk-fill composites. Increased extent of polymerisation with bulk-fill composites is obtained with the modulation of translucency and photoinitiators. Moszner et al. reported that the germanium-based Ivocerin initiator in Tetric EvoCeram Bulk-Fill exhibits increased light activation than camphorquinone [16]. A new germanium-based photoinitiator has been accepted as a pre-polymer stress reliever that putatively decreases polymerisation shrinkage and stress [23]. While polymerising resin composites, the tip of light source was positioned 0.5 mm distant to the resin composite surface [24].
Even if an adhesive is not used, resin composites could hold to the cavity surface due to surface irregularity; in unbonded groups, the shrinkage pattern was not regular [25]. In our study, volumetric loss (%) was significantly increased in unbonded samples compared with bonded samples. This result shows that the use of an adhesive significantly reduced the volumetric shrinkage. On examining shrinkage using micro-CT with and without an adhesive resin, Algamaiah et al. showed that the adhesive application in combination with different bulk-fill composites reduces polymerisation shrinkage by approximately 13% [26]. The values obtained in this study were considerably less. However, from clinical perspective, application of adhesive resin adds to the time spent also for the bulk-fill composites.
In all situations except in unbonded samples with a 2-mm depth, SDR showed higher polymerisation shrinkage than other resin composites. The results of this observation are consistent with that of Algamaiah et al. [26] where SDR showed the highest percentage in shrinkage among all tested materials (Tetric EvoCeram Bulk-Fill, and Filtek flowable Bulk-Fill) (3.65% and 3.78%, respectively).
Given its three-dimensional imaging capabilities, micro-CT is a preferred method to measure polymerisation shrinkage in cavities [25]. The accuracy of this method also allows for visualisation of failures, such as air bubbles, which cannot be rendered by conventional methods, such as replica techniques [12]. An important limitation of micro-CT is noted with analysing materials with low fillers or those that do not have sufficient radiopacity, such as certain dental adhesives [25, 27]. Both enamel and resin composites highly scatter light. Thus, differentiating between the two and setting a threshold is more challenging and potentially causes uncertainty. Although scanning in micro-CT was performed in fixed positions and images of samples were arranged using fiducial markers or reference locations in each sample, the images may not completely overlap during measurements before and after polymerisation [28]. This is one limitation of this study. Nevertheless, in contrast to sectioning procedures that inherently damage specimens, micro-CT is a non-destructive 3D imaging method. Given its three-dimensional imaging capabilities, micro-CT is the preferred device to measure polymerisation shrinkage in cavities [25]. The accuracy of this method allows us to visualise failures as bubbles, which cannot be rendered by conventional methods, such as replica techniques [12]. The results of this study should be verified in larger samples, and different cavity dimensions should be correlated with shrinkage potential of the bulk-fill materials in future studies.
Resin composites with high filler loads have less monomers and thus less polymerisation shrinkage. Although filler particle space does not participate in polymerisation contraction, high filler loads require low-molecular-weight monomers to ensure proper viscosity for handling. Conversely, in lower viscosity materials, monomers move actively given their increased participation in increasing polymerisation shrinkage [29]. In this study, the SDR group presented significantly higher volumetric loss than FB and TB. As a result, it could be stated that low-viscosity bulk-fill composites show higher polymerisation shrinkage than high-viscosity bulk composite. When comparing shrinkage amounts according to the cavity depth, 4-mm deep cavities showed more shrinkage compared with 2-mm deep cavities in most groups, thus indicating that bulk-fill composites currently have an acceptable shrinkage range, but further improvements are still needed for larger and deeper cavities.
Conclusions
From this study, the following could be concluded:
- 1)
All tested bulk-fill resin composites tested showed polymerisation shrinkage at varying degrees depending on the product.
- 2)
Increased cavity depth from 2 to 4 mm increased shrinkage and volumetric loss in all materials tested except for FB.
- 3)
Application of adhesive resin decreased volumetric loss, but samples with and without adhesive SDR showed significantly higher volumetric loss compared with other bulk-fill materials.
References
Bouillaguet S, Gamba J, Forchelet J, Krejci I, Wataha JC (2006) Dynamics of composite polymerization mediates the development of cuspal strain. Dent Mater 22:896–902
Silikas N, Eliades G, Watts DC (2000) Light intensity effects on resin-composite degree of conversion and shrinkage strain. Dent Mater 16:292–296
Krejci I, Planinic M, Stavridakis M, Bouillaguet S (2005) Resin composite shrinkage and marginal adaptation with different pulse-delay light curing protocols. Eur J Oral Sci 113:531–536
Panduric V, Demoli N, Tarle Z, Sariri K, Mandic VN, Knezevic A, Sutalo J (2007) Visualization of marginal integrity of resin-enamel interface by holographic interferometry. Oper Dent 32:266–272
Tsujimoto A, Barkmeier WW, Takamizava T, Latta MA, Miyazaki M (2017) Depth of cure, flexural properties and volumetric shrinkage of low and high viscosity bulk-fill giomers and resin composites. Dent Mater 36:205–213
Walter R (2013) Bulk-fill flowable composite resins. J Esthet Restor Dent 25:72–76
Elliot JC, Dover SD (1982) X-ray microtomography. J Microsc 126:211–213
Gambill JM, Alder M, del Rio CE (1996) Comparison of nickel-titanium and stainless steel hand-file instrumentation using computed tomography. J Endod 22:369–375
Rhodes JS, Ford TR, Lynch JA, Liepins PJ, Curtis RV (1999) Microcomputed tomography: a new tool for experimental endodontology. Int Endod J 32:165–170
Kuhn JL, Goldstein SA, Feldkamp LA, Goulet RW, Jesion G (1990) Evaluation of a microcomputed tomography system to study trabecular bone structure. J Orthop Res 8:833–842
Bergmans L, Van Cleynenbreugel J, Beullens M, Wevers M, Van Meerbeek B, Lambrechts P (2003) Progressive versus constant tapered shaft design using NiTi rotary instruments. Int Endod J 36:288–295
Sun J, Lin-Gibson S (2008) X-ray microcomputed tomography for measuring polymerization shrinkage of polymeric dental composites. Dent Mater 24:228–234
Kim HJ, Park SH (2014) Measurement of the internal adaptation of resin composites using micro-CT and its correlation with polymerization shrinkage. Oper Dent 39:57–716
Ilie N, Bucuta S, Draenert M (2013) Bulk-fill resin-based composites: an in vitro assessment of their mechanical performance. Oper Dent 38:618–625
Leprince JG, Palin WM, Vanacker J, Sabbagh J, Devaux J, Leloup G (2014) Physico-mechanical characteristics of commercially available bulk-fill composites. J Dent 42:993–1000
Kleverlaan CJ, Feilzer AJ (2005) Polymerization shrinkage and contraction stress of dental resin composites. Dent Mater 21:1150–1157
Ferracane JL, Mitchem JC (2003) Relationship between composite contraction stress and leakage in Class V cavities. Am J Dent 16:239–243
Calheiros FC, Sadek FT, Braga RR, Cardoso PE (2004) Polymerization contraction stress of low-shrinkage composites and its correlation with microleakage in Class V restorations. J Dent 32:407–412
Han SH, Park SH (2017) Comparison of internal adaptation in Class II bulk-fill composite restorations using micro-CT. Oper Dent 42:203–214
Gordan VV, Mjor IA (2002) Short- and long-term clinical evaluation of postoperative sensitivity of a new resin-based restorative material and self-etching primer. Oper Dent 27:543–548
Ilie N, Hickel R (2009) Investigations on mechanical behavior of dental composites. Clin Oral Investig 13:427–438
Cho E, Sadr A, Inai N, Tagami J (2011) Evaluation of resin composite polymerization by three dimensional micro-CT imaging and nanoindentation. Dent Mater 27:1070–1078
Moszner N, Fischer UK, Ganster B, Liska R, Rheinberger V (2008) Benzoyl germanium derivatives as novel visible light photoinitiators for dental materials. Dent Mater 24:901–907
Fronza BM, Rueggeberg FA, Braga RR, Mogilevych B, Soares LES, Martin AA, Ambrosano G, Giannini M (2015) Monomer conversion, microhardness, internal marginal adaptation, and shrinkage stress of bulk-fill resin composites. Dent Mater 31:1542–1551
Chiang YC, Röschb P, Dabanoglu A, Linc CP, Hickel R, Kunzelmanna KH (2010) Polymerization composite shrinkage evaluation with 3D deformation analysis from CT images. Dent Mater 26:223–231
Algamaiah H, Sampaio CS, Rigo LC, Janal MN, Giannini M, Bonfante EA, Coelho PG, Reis AF, Hirata R (2017) Microcomputed tomography evaluation of volumetric shrinkage of bulk-fill composites in class ii cavities. J Esthet Restor Dent 29:118–127
Papadogiannis D, Kakaboura A, Palaghias G, Eliades G (2009) Setting characteristics and cavity adaptation of low-shrinkage resin composites. Dent Mater 25:1509–1516
Zeiger DN, Sun J, Schumacher GE, Lin-Gibson S (2009) Evaluation of dental composite shrinkage and leakage in extracted teeth using X-ray microcomputed tomography. Dent Mater 25:1213–1220
Davidson CL, Feilzer AJ (1997) Polymerization shrinkage and polymerization shrinkage stress in polymer based restoratives. J Dent 25:435–440
Funding
The work was supported by TUBITAK (Grant number: 215S840), Turkey.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This article does not contain any studies with human participants or animals.
Informed consent
Formal consent is not required for this type of study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Ersen, K.A., Gürbüz, Ö. & Özcan, M. Evaluation of polymerization shrinkage of bulk-fill resin composites using microcomputed tomography. Clin Oral Invest 24, 1687–1693 (2020). https://doi.org/10.1007/s00784-019-03025-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-019-03025-5