
Abstract
Objectives
The purpose of the present study was to evaluate the retentive forces of CAD/CAM-fabricated polyetheretherketone (PEEK) secondary crowns on zirconia primary crowns over an artificial aging period representing 10 years of clinical service and compare them to electroformed secondary crowns made from pure gold.
Material and methods
Implant-supported zirconia primary crowns (N = 20) were CAD/CAM milled and provided either with electroformed secondary crowns (group ZE; N = 10) or CAD/CAM-fabricated PEEK secondary crowns (group ZP; N = 10). All secondary crowns were attached to a casted tertiary structure to ensure adequate stability. A universal testing machine was used to determine the retentive force values at baseline and after 1, 3, 5, and 10 years of simulated aging in the presence of artificial saliva. Data were analyzed applying Kolmogorov-Smirnov, Kruskal-Wallis, and Mann-Whitney U test. Level of significance was set at p < 0.05.
Results
Retentive forces were not different for the groups ZE and ZP at baseline (median ZE 2.85 N; ZP 2.8 N; p ≤ 0.218). Because retentive force values changed significantly over simulation time for group ZE (Kruskal-Wallis; p ≤ 0.028), the values between the test groups ZE and ZP differed significantly (Mann-Whitney U) at 5 years (ZE 3.03 N; ZP 2.76 N; p ≤ 0.003) and 10 years (ZE 3.1 N; ZP 2.78 N; p ≤ 0.011).
Conclusions
PEEK secondary crowns exhibit stable retentive force values over 10 years of simulated aging showing no signs of deterioration while the retentive force values of electroformed secondary crowns increase over time.
Clinical relevance
PEEK might be a suitable alternative to proven metallic materials for the fabrication of secondary crowns.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
A variety of different treatment options is available in modern dentistry, including conventional concepts that have proven their reliability for decades, but also innovative computer-aided workflows that have created entirely new opportunities [1].
The double crown technique was described as early as 1886, when American dentist R. Walter Starr attached a removable bridge by means of double crown technique [2]. Ever since, double crowns have become established as a solid treatment option in everyday dental practice, especially to attach removable partial dentures (RPDs) [3]. Nowadays, double crown systems are commonly used to anchor dentures to the residual dentition or to dental implants, or combined to both [4, 5]. Double crown systems consist of an inner primary crown attached to the tooth or implant and a precisely matching outer secondary crown firmly connected to the denture [6]. The retentive effect of classical double crown systems is based on the mechanical principles of either friction or wedging. The original telescopic crown, as described by Böttger in 1953, is based on the principle of friction of parallelized surfaces [7]. A variation of the telescopic double crown is the clearance fit double crown presented by Hofmann in 1966, which provides guidance and resistance to horizontal displacement but no vertical support [8]. Not much later, Körber introduced the conical double crown system in 1968, thus establishing a system in which retention is based on the principle of wedging [9]. For both telescopic and conical double crown systems, high patient comfort and favorable long-term survival rates have been reported [4, 10,11,12]. Double crowns effectively transfer the occlusal forces along the longitudinal axis of the abutment tooth or implant abutment. In addition, they provide guidance, support, and protection against dislodging movements [3]. Further benefits are whether tooth or implant supported, the universal applicability, the good hygiene capability, and uncomplicated expansion options [3, 13]. Primary and secondary crowns commonly made from precious, reduced precious, and non-precious alloys are usually manufactured using analogue casting methods, primarily the lost-wax technique [13, 14].
Another younger approach is represented by the electroforming of secondary crowns, as introduced by Diedrichs and Rosenhain [15]. The galvanic process entails the electrolytic deposition of gold ions on a specially prepared master die or the conical primary crown [16]. Using this technology, the retention between inner and outer crown is basically created by hydraulic adhesion [17, 18]. The retentive force is determined by the gap between the primary and the secondary telescopic crown as well as the composition and viscosity of the saliva and the denture’s removal speed [19,20,21]. The technology exhibits certain advantages. The electroforming process leads to a reproducible and exact fit without a need for manual adjustments resulting in an ideally balanced degree of retentive force, which is almost independent of individual chewing pressure [18]. Intraorally bonding the secondary crowns to the tertiary framework ensures the “passive fit,” which is considered desirable in terms of proper stress distribution, especially with implant-supported dentures [20, 22]. On the downside, the complexity and technique sensitivity of technology leads to a time-consuming and expensive manufacturing process [23].
The application of zirconia as a primary crown material has undoubtedly proven to be reliable in terms of retention and wear performance [20, 24, 25]. In general, aesthetic virtues, superior physical properties, and a high level of biocompatibility make zirconia an interesting material that meets many of the requirements of modern dentistry [26]. Additionally, zirconia can be excellently embedded in the CAD/CAM workflow and thus bridges the gap for the double crown systems to computer-aided technologies.
Dental CAD/CAM, for its part, has advantages such as the use of modern high capacity materials, increased efficiency in the dental laboratory, or better quality control, resulting in improved predictability, fit, and durability of the denture [27]. One of these innovative materials that have recently been established is polyetheretherketone (PEEK). PEEK has long been used in medicine as a high performance thermoplastic resin having favorable physicochemical properties [28]. It is a modified semi-crystalline polyaryletherketone (PAEK) with an elastic modulus (3–4 GPa) that can be altered relatively easily to resemble that of human cortical bone and dentine (18 GPa) [29]. Due to its properties and history in orthopedics, PEEK first appeared in the dental discourse as a possible alternative material for dental implants. Inferior osteoconductive potential and bioactivity of current PEEK materials compared to titanium have impeded, inter alia, its serious implementation on this matter [30]. Nevertheless, exhibiting chemical inertness and thus superior biocompatibility, high thermal and chemical resistance, low water solubility [28], moderate biofilm formation [31], and excellent mechanical properties [28, 32], PEEK has attracted attention and is increasingly being used in fixed and removable prosthetics [33]. The possibility of efficiently processing PEEK within the framework of the digital workflow makes it particularly interesting for modern dentistry and an appealing possible alternative to electroformed secondary crowns in implant-prosthetics.
So far, few in vitro studies have been conducted on the performance of PEEK as a double crown material, but it has been consistently reported that it could be a suitable material for the indication [34,35,36,37].
This in vitro study aimed to compare the changes in retentive force values of CAD/CAM produced PEEK secondary crowns during artificial aging and compare them to electroformed ones (control). Retentive force values were measured before, during, and after 10,000 separation cycles and simultaneous thermocycling. The null hypothesis was that there will be no difference between the retentive force values of PEEK secondary crowns and the electroformed ones. Further on, it was hypothesized that artificial aging has no influence on the retentive force values of both experimental groups over time.
Materials and methods
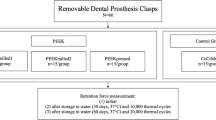
The experimental setup of the study is presented in Fig. 1. The CAD/CAM-fabricated primary crowns made from zirconia (N = 20) were attached to implant-supported titanium bases and the secondary crowns were either electroformed from pure gold (group ZE; N = 10) or CAD/CAM-fabricated from PEEK (group ZP; N = 10). A tertiary framework made from non-precious alloy to which the secondary crown was adhesively attached was manufactured to prevent the secondary crowns from damage during artificial aging [17].

Experimental setup
Primary crowns
On a lab analogue implant (ZZ Base C-CL MI 5.0, Zirkonzahn, Gais, Italy), a scan marker (ZZ Base C-CL SM 5.0, Zirkonzahn) was mounted and scanned using a structured light scanner (S600 Arti Scanner, Zirkonzahn). Applying a modeling software (Modellier; version 6194, Zirkonzahn), an abutment was designed featuring a cone angle of 1° and a vertical height of 7 mm. The abutment was milled (M1 Milling Unit, Zirkonzahn) 20 times from a zirconia blank (Anatomic Coloured 95H14 A2, LOT ZB6256A, Zirkonzahn). Adhesive cementation of the zirconia abutments onto the titanium bases (ZZ Base C-CI PCTBH 5,0, Zirkonzahn) was carried out according to the manufacturer’s specifications using a self-curing luting composite (Multilink Hybrid Abutment HO 0, Ivoclar Vivadent AG, Schaan, FL). The specimens were circularly finished manually, utilizing a water-cooled grinder with a 1° cone angle (Acurata, Thurmansbang, Germany) and a parallelometer.
Electroformed secondary gold crowns
In the group ZE, the primary crowns were spray-coated (Solaris, Degudent, Hanau, Germany) with a thin layer of conductive silver lacquer using an airbrush gun (Sirius Dental, Frankfurt, Germany) and the secondary crowns were then electroformed in an automated electroplater (Preciano IQ, Heraeus Kulzer, Hanau, Germany). Device setting was chosen to create gold layers of approximately 0.25–0.3 mm in thickness. Subsequently, the secondary crowns were adhesively attached (AGC CEM, Wieland Pforzheim, Germany) to casted tertiary structures made from non-precious alloy (Remanium Star, Ispringen, Germany).
CAD/CAM secondary PEEK crowns
In the group ZP, every primary crown was coated with a thin and even layer of scan spray (Zirko Scanspray, Zirkonzahn) and scanned (S600 Arti Scanner, Zirkonzahn). Using the CAD software, a secondary crown with a wall thickness of 0.3 mm was modeled for each primary crown. All 10 secondary crowns of the group ZP were milled from one PEEK resin blank (Tecno Med 95 H12, LOT 7286, Zirkonzahn) using appropriate milling cutters (PMMA CAD/CAM Ø 2L, Ø 1L, and Ø 0.5S, Zirkonzahn). The PEEK crowns were also adhesively attached to the tertiary structures.
Artificial aging and retentive force measurements
To simulate clinical conditions as close as possible, the retentive force measurements and the artificial aging procedures were conducted in a bath of artificial saliva (Glandosane, Fresenius, Bad Homburg, Germany). The retentive force values were determined at a separation speed of 1000 mm/min [20, 25, 38]. After baseline testing, all samples were subjected to artificial aging in the chewing simulator (Chewing Simulator CS-4, Mechatronic, Feldkirchen-Westerham, Germany), undergoing 1095 aging cycles (representing 1 year of clinical service with 3 times removal/day) and simultaneous thermocycling (5 °C/55 °C). A special specimen holder ensured that the secondary crowns were only moving along the insertion axis during joining and separating of the components (Fig. 2) [25]. Joining speed was set at 60 mm/s and separation speed at 10 mm/s. The joining force was 20 N [25]. Retentive force measurements were conducted and subsequently repeated after 3 years (3285 cycles), 5 years (5475 cycles), and 10 years (10,950 separation cycles) of artificial aging.

Schematic representation of the specimen holder. (1) Gadget to mount the die of the chewing simulator, (2) ball joint, (3) guide pins, (4) gadget to mount the specimen, (5) resin to fix the secondary crown, (6) implant with primary crown embedded in resin, (7) screw thread to mount the chewing simulator, (8) specimen, and (9) screw to adjust the specimen [25]
Statistical analysis
Kolmogorov-Smirnov test was applied to evaluate whether the values were distributed normally within the test groups. Kruskal-Wallis test was applied to find out if a difference in retentive forces occurred within the groups over time. To compare the groups with each other at different stages of artificial aging, the Mann-Whitney U test was used.
For statistical evaluation, the software SPSS (Statistics 23.0, SPSS Inc., Stanford, USA) was used and level of significance was set at p < 0.05.
Results
Retentive forces were not different for secondary crowns made from PEEK and electroformed the ones at baseline. The groups ZE and ZP showed median retentive force values of 2.85 N and 2.8 N respectively. Retentive force values changed over artificial aging time only for group ZE. Groups ZE and ZP displayed 3.03 N (ZE) and 2.76 N (ZP) after 5 years as well as 3.1 N (ZE) and 2.78 N (ZP) after 10 years of simulated aging.
Mann-Whitney U test showed no significant differences at baseline (p ≤ 0.218), after 1 year (1095 cycles; p ≤ 0.52), and after 3 years (3285 cycles; p ≤ 0.52). Significant differences could be found between group ZE and group ZP after 5 years (5475 cycles; p ≤ 0.003) and after 10 years (10,950 cycles; p ≤ 0.011). This is due to the fact that a significant (Kruskal-Wallis test) raise of retentive forces was observed over time for group ZE (p ≤ 0.028). Group ZP did not display significant aging-related changes whatsoever (p ≤ 0.938).
The results for retentive force values over time for groups ZE and ZP are given in Fig. 3 and Table 1.

Comparison of the retentive force value changes in the experimental groups at different stages of aging
Discussion
This study evaluated the differences in retentive force over time of CAD/CAM-fabricated secondary crowns made from a polyetheretherketone (PEEK) versus electroformed secondary crowns made from pure gold on zirconia primary crowns. Electroformed secondary crowns are expensive to manufacture [23] and have proven prone to some complications [22]. The intention of the current investigation was therefore to examine a completely digital method of efficiently producing double crowns for implant prosthetic use, stripping out some of the disadvantages of the electroformed secondary crowns, but also operating according to the hydraulic principle and ensuring a satisfactory passive fit.
The artificial aging had significant influence on the retentive force of the electroformed primary crowns by means of an increase of their retentive force. The PEEK secondary crowns presented stable retentive force values over the time of simulation. Also, the retentive force values differed between groups ZE and ZP after 5 and 10 years of simulation. Therefore, both hypotheses had to be rejected.
Previous studies have shown that the retentive force of double crowns depends on cone angle, abutment height, precision of fit, material, and artificial aging [17, 20, 25, 39]. Especially for electroformed secondary crowns, a growth of retentive force results from an increasing abutment height and decreasing cone angle [20, 25]. The height of 7 mm chosen for all primary crowns in the present study represents a clinically relevant value [20, 25]. Also, a cone angle of 1° means a clinical standard that was used in previous studies [34,35,36,37]. In addition to the shape of the primary crown, the thickness of the conductive silver lacquer of about 0.008–0.012 mm also affects the retentive force values [15]. Another factor is the presence and quality of artificial saliva [20, 39]. The substitute used in this study has proven its ability to mimic the characteristics of human saliva [40].
Weigl showed that retentive force values of electroformed secondary crowns are not correlated to masticatory forces [17] and therefore the applied joining force of 40 N was not supposed to have a significant impact. The number of 10,000 separation cycles representing 10 years of clinical service has proven to be adequate to receive sound results [19, 24, 25, 41]. Separation speed values in previous investigations varied widely between 1 mm/min [23] and 1000 mm/min [20, 25, 38], whereby many authors recently chose a value of about 50 mm/min [34, 36, 37]. However, Ohkawa et al. found that a clinically relevant separation speed of a telescopic denture was around 6000 mm/min [38]. Since the separation speed affects the retentive force values of double crowns based on hydraulic retention [21], a separation speed of 1000 mm/min was chosen in accordance with earlier investigations [20, 25, 38].
Usually, patients feature two or more double crowns and abutment teeth or implants are distributed heterogeneously, which affects not least handling and thus clinical retentive behavior. Nonetheless, as many previous studies agreed on testing single double crown specimens [19, 20, 23,24,25, 34,35,36,37, 41], and in order to obtain comparable results, this modus operandi appeared plausible and therefore was adopted.
The retentive force values found in this study are in line and comparable with the results of Engels et al. They tested electroformed secondary crowns with 7-mm-high zirconia primary crowns, which exhibited baseline retentive force values of 1.68 N (cone angle 2°) and 3.44 N (cone angle 0°) respectively [25]. A mean baseline retentive force of 2.86 N at a cone angle of 1° in the present study seems thus plausible. Overall, the results of investigations dealing with the retentive force values of electroformed secondary crowns on zirconia primary crowns are rather discrepant. In contrast to the present results, Beuer et al. observed significantly lower retentive force values in specimen with cone angles of 0° and 2°. Nevertheless, they claimed zirconia to be an alternative to high gold alloys for primary crowns [20], as patients seem to be satisfied with retentive force values of 2.5–3 N for RPDs in general [42]. Other investigators found higher retentive force values for electroformed secondary crowns on zirconia primary crowns of 5.57 N [24] or even 7.4 N [14] in similar experimental setups.
The increase in retentive force values observed in the electroformed secondary crowns after aging is in contrast to other findings, which mostly exhibit decreasing retentive forces [14, 25] or no significant changes [17, 24]. In opposition, and therefore in line with the present study, Dillschneider et al. showed slightly increasing retentive force values for electroformed secondary crowns on zirconia primary crowns during artificial aging [41], but did not comment on possible causes. The phenomenon of increasing values could be attributed to the high ductility of the pure gold. As a result, the electroformed secondary crowns gradually adapt better to the primary crowns, while the gap sizes decrease. Consequently, the hydraulic operating principle gets stronger and retentive force increases.
Engels et al. also demonstrated that electroformed secondary crowns were not necessarily superior to conventional cast secondary crowns in terms of retentive force and wear behavior but displayed more predictable retentive force values [25]. On the contrary, Dillschneider et al. found electroformed secondary crowns to show more consistency in retentive force values over time compared to conventional cast secondary crowns [41]. Bayer et al. found a slightly higher level of retention force for electroformed secondary crowns, but no significant difference in wear behavior. Thus, both technologies, electroforming and casting, were regarded as applicable for clinical practice [19]. As different physical principles of retention take effect and the fields of clinical application vary, the direct comparison of conventional cast telescopic or conical double crowns with the ones operating on the hydraulic principle was not within the scope of the present study.
Focusing on PEEK secondary crowns, only a few in vitro studies are existing [35,36,37]. The authors of the present investigation are not aware of profound clinical data. Hahnel et al. presented a case report, describing the usage of PEEK in a double crown-retained RPD. They recommended that, concerning the difficulties in bonding to PEEK and the lack of knowledge regarding retentive behavior, it should only be used in interim dentures at present, and further investigations are necessary [43].
So far, all authors of laboratory studies rated their findings as promising and PEEK as an interesting material option for double crown prosthetics. Only Merk et al. investigated the retentive force values of PEEK secondary crowns on zirconia primary crowns [36]. The milled secondary crowns with a cone angle of 1° presented an average retentive force of 6.07 N [36], and thus significantly higher values compared to the ones in the present study. The explanation for this could be found in different settings of the production parameters during the CAD/CAM production. Merk et al. noted that one of the most important aspects of CAD/CAM production is the definition of software parameters for the design of the secondary crowns [36]. By varying the “offset,” in other words defining the gap size between the primary and secondary crown, the retentive force values can be adjusted. This fact provides interesting possibilities to digitally tailor the retentive force individually for each anchor of the denture to the individual clinical situation and needs. In accordance with the findings of Wagner et al. [35], the PEEK secondary crowns exhibited constant retentive force values during artificial aging, which could be attributed to the excellent mechanical and physicochemical properties of the material [28]. Though the level of median values was on the same level at baseline for groups ZE and ZP, group ZP exhibited higher degree of variance (IQR (interquartile range) values).
This leads to the assumption that the manual processing steps within the almost entirely digital workflow of the PEEK secondary crowns, especially the spray-coating of the primary crowns, might influence the resulting retentive forces. This assumption subsequently resulted in an expansion of the study design to find out about the impact of the manual handling processes during the fabrication of the PEEK secondary crowns.
Therefore, test specimen No. 6 was randomly selected from the group ZP and 10 secondary crowns (group ZPI) were milled from one PEEK blank, applying the same dataset (N = 10) and thus identical production parameters. The specimens underwent baseline retentive force measurements (group ZPI) and the results were then compared with baseline retentive force values of groups ZE and ZP. Results are given in Fig. 4.

Comparison of retentive force values of the group ZE, the group ZP, and the subgroup ZPI at baseline
By avoiding the impact of imprecisions during manual processing steps, more precisely, variations in the application of scan spray, the IQR in group ZPI (0.21 N) could be reduced in comparison to group ZP (IQR 0.72 N); however, it still does not reach the reproducibility of group ZE (IQR 0.12 N). This means, although the manual application of scan spray was conducted by a skilled expert under standardized conditions, it represents a source of error within the digital workflow and should be subject to further investigations. Repeating the milling process with identical design and production parameters for one single specimen, it could be shown that the CAM process scarcely presented any variance and thus its impact on the overall result seems to be negligible.
Due to these promising results in terms of manufacturing accuracy, another future topic could be the approach of producing secondary crowns and framework as a monolithic workpiece [23]. This could, on condition of an acceptable passive fit, help further minimize the work effort, diminish potential sources of technical complications, and although less crucial in implant-prosthetics, reduce space requirements.
An invaluable advantage of the complete digital fabrication of double crowns is that in case of loss of retention or any other damage to the secondary crown, any part of the structure can be reproduced any number of times based on the stored data.
Conclusion
The findings of this in vitro study suggest that CAD/CAM-manufactured secondary crowns made from polyetheretherketone (PEEK) are able to provide sufficient and stable retentive force values even after artificial aging representing 10 years of clinical use. Based on these data, PEEK secondary crowns could offer an efficient and appropriate alternative to electroformed secondary crowns used in removable implant prosthetics and forward the integration into the digital workflow. Further clinical investigations on the long-term behavior and survival rates under clinical conditions are necessary. As the higher IQRs of PEEK secondary crowns can be attributed to systemic inaccuracies, particularly with regard to manual processing steps, future scientific efforts should also address this issue.
References
van Noort R (2012) The future of dental devices is digital. Dent Mater 28(1):3–12. https://doi.org/10.1016/j.dental.2011.10.014
Starr W (1886) Removable bridge-work. - porcelain cap-crowns. The Dental cosmos; a monthly record of dental science 28 (1):17–19
Langer A (1981) Telescope retainers for removable partial dentures. J Prosthet Dent 45(1):37–43
Lian M, Zhao K, Feng Y, Yao Q (2018) Prognosis of combining remaining teeth and implants in double-crown-retained removable dental prostheses: a systematic review and meta-analysis. Int J Oral Maxillofac Implants 33(2):281–297. https://doi.org/10.11607/jomi.5796
Rammelsberg P, Bernhart G, Lorenzo Bermejo J, Schmitter M, Schwarz S (2014) Prognosis of implants and abutment teeth under combined tooth-implant-supported and solely implant-supported double-crown-retained removable dental prostheses. Clin Oral Implants Res 25(7):813–818. https://doi.org/10.1111/clr.12197
Langer Y, Langer A (2000) Tooth-supported telescopic prostheses in compromised dentitions: a clinical report. J Prosthet Dent 84(2):129–132. https://doi.org/10.1067/mpr.2000.108026
Böttger H (1953) Die prothetische Versorgung des Lü̧ckengebisses mit Teleskopprothesen. Zahnärztl Rundsch (62):18–23
Hofmann M (1966) Die Versorgung von Gebissen mit einzelstehenden Restzähnen mittels sog. Cover-Denture-Prothesen. Dtsch Zahnärztl Z 21:478–482
Körber K (1968) Konuskronen – ein physikalisch definiertes Teleskopsystem. Dtsch Zahnärztl Z 23:619–630
Koller B, Att W, Strub JR (2011) Survival rates of teeth, implants, and double crown-retained removable dental prostheses: a systematic literature review. Int J Prosthodont 24(2):109–117
Wostmann B, Balkenhol M, Kothe A, Ferger P (2008) Dental impact on daily living of telescopic crown-retained partial dentures. Int J Prosthodont 21(5):419–421
Stober T, Danner D, Bomicke W, Hassel AJ (2016) Improvement of oral health-related quality-of-life by use of different kinds of double-crown-retained removable partial dentures. Acta Odontol Scand 74(1):1–6. https://doi.org/10.3109/00016357.2014.976262
Langer A (1980) Telescope retainers and their clinical application. J Prosthet Dent 44(5):516–522 doi:0022-3913(80)90070-0
Arnold C, Hey J, Setz JM, Boeckler AF, Schweyen R (2017) Retention force of removable partial dentures with different double crowns. Clin Oral Investig 22:1641–1649. https://doi.org/10.1007/s00784-017-2224-x
Diedrichs G, Rosenhain P (1991) Galvano-Außenteleskope in der direkten Technik. Quintessenz 42:49–55
Vence BS (1997) Electroforming technology for galvanoceramic restorations. J Prosthet Dent 77(4):444–449
Weigl P, Hahn L, Lauer HC (2000) Advanced biomaterials used for a new telescopic retainer for removable dentures. J Biomed Mater Res 53(4):320–336
Weigl P, Lauer HC (2000) Advanced biomaterials used for a new telescopic retainer for removable dentures. J Biomed Mater Res 53(4):337–347
Bayer S, Kraus D, Keilig L, Golz L, Stark H, Enkling N (2012) Wear of double crown systems: electroplated vs. casted female part. J Appl Oral Sci 20(3):384–391
Beuer F, Edelhoff D, Gernet W, Naumann M (2010) Parameters affecting retentive force of electroformed double-crown systems. Clin Oral Investig 14(2):129–135. https://doi.org/10.1007/s00784-009-0271-7
Faber F, Huber C (2001) Electroformed telescope crowns – a hydraulic system. J Dent Res 80(Spec Iss):551
Schwindling FS, Lehmann F, Terebesi S, Corcodel N, Zenthofer A, Rammelsberg P, Stober T (2017) Electroplated telescopic retainers with zirconia primary crowns: 3-year results from a randomized clinical trial. Clin Oral Investig 21(9):2653–2660. https://doi.org/10.1007/s00784-017-2067-5
Schwindling FS, Stober T, Rustemeier R, Schmitter M, Rues S (2016) Retention behavior of double-crown attachments with zirconia primary and secondary crowns. Dent Mater 32(5):695–702. https://doi.org/10.1016/j.dental.2016.03.002
Bayer S, Kraus D, Keilig L, Golz L, Stark H, Enkling N (2012) Changes in retention force with electroplated copings on conical crowns: a comparison of gold and zirconia primary crowns. Int J Oral Maxillofac Implants 27(3):577–585
Engels J, Schubert O, Guth JF, Hoffmann M, Jauernig C, Erdelt K, Stimmelmayr M, Beuer F (2013) Wear behavior of different double-crown systems. Clin Oral Investig 17(2):503–510. https://doi.org/10.1007/s00784-012-0746-9
Miyazaki T, Nakamura T, Matsumura H, Ban S, Kobayashi T (2013) Current status of zirconia restoration. J Prosthodont Res 57(4):236–261. https://doi.org/10.1016/j.jpor.2013.09.001
Miyazaki T, Hotta Y, Kunii J, Kuriyama S, Tamaki Y (2009) A review of dental CAD/CAM: current status and future perspectives from 20 years of experience. Dent Mater J 28:44–56
Kurtz SM, Devine JN (2007) PEEK biomaterials in trauma, orthopedic, and spinal implants. Biomaterials 28(32):4845–4869. https://doi.org/10.1016/j.biomaterials.2007.07.013
Skinner HB (1988) Composite technology for total hip arthroplasty. Clin Orthop Relat Res (235):224-236
Najeeb S, Bds ZK, Bds SZ, Bds MS (2016) Bioactivity and osseointegration of PEEK are inferior to those of titanium: a systematic review. J Oral Omplantol 42(6):512–516. https://doi.org/10.1563/aaid-joi-D-16-00072
Hahnel S, Wieser A, Lang R, Rosentritt M (2015) Biofilm formation on the surface of modern implant abutment materials. Clin Oral Implants Res 26(11):1297–1301. https://doi.org/10.1111/clr.12454
Wimmer T, Huffmann AM, Eichberger M, Schmidlin PR, Stawarczyk B (2016) Two-body wear rate of PEEK, CAD/CAM resin composite and PMMA: effect of specimen geometries, antagonist materials and test set-up configuration. Dent Mater 32(6):e127–e136. https://doi.org/10.1016/j.dental.2016.03.005
Najeeb S, Zafar MS, Khurshid Z, Siddiqui F (2016) Applications of polyetheretherketone (PEEK) in oral implantology and prosthodontics. J Prosthodont Res 60(1):12–19. https://doi.org/10.1016/j.jpor.2015.10.001
Stock V, Schmidlin PR, Merk S, Wagner C, Roos M, Eichberger M, Stawarczyk B (2016) PEEK primary crowns with cobalt-chromium, zirconia and galvanic secondary crowns with different tapers-a comparison of retention forces. Materials (Basel) 9(3). https://doi.org/10.3390/ma9030187
Wagner C, Stock V, Merk S, Schmidlin PR, Roos M, Eichberger M, stawarczyk B (2018) Retention load of telescopic crowns with different taper angles between cobalt-chromium and polyetheretherketone made with three different manufacturing processes examined by pull-off test. J Prosthodont 27(2):162–168
Merk S, Wagner C, Stock V, Eichberger M, Schmidlin PR, Roos M, Stawarczyk B (2016) Suitability of secondary PEEK telescopic crowns on zirconia primary crowns: the influence of fabrication method and taper. Materials (Basel) 9(11). https://doi.org/10.3390/ma9110908
Stock V, Wagner C, Merk S, Roos M, Schmidlin PR, Eichberger M, Stawarczyk B (2016) Retention force of differently fabricated telescopic PEEK crowns with different tapers. Dent Mater J 35(4):594–600. https://doi.org/10.4012/dmj.2015-249
Ohkawa S, Okane H, Nagasawa T, Tsuru H (1990) Changes in retention of various telescope crown assemblies over long-term use. J Prosthet Dent 64(2):153–158
Gungor MA, Artunc C, Sonugelen M (2004) Parameters affecting retentive force of conus crowns. J Oral Rehabil 31(3):271–277. https://doi.org/10.1111/j.1365-2842.2004.01036.x
Hatton MN, Levine MJ, Margarone JE, Aguirre A (1987) Lubrication and viscosity features of human saliva and commercially available saliva substitutes. J Oral Maxillofac Surg 45(6):496–499
Dillschneider T, Nothdurft F, Abed-Rabbo M, Mitov G, Pospiech P (2009) In vitro-investigations on the wear behavior of different double crown systems. Dent Mater 25(5):e20
Becker H (1982) Untersuchung der Abzugskräfte abnehmbarer Teleskop-Prothesen. Zahnärztl Prax 33:153–156
Hahnel S, Scherl C, Rosentritt M (2018) Interim rehabilitation of occlusal vertical dimension using a double-crown-retained removable dental prosthesis with polyetheretherketone framework. J Prosthet Dent 119(3):315–318. https://doi.org/10.1016/j.prosdent.2017.02.017
Acknowledgments
The authors thank Zirkonzahn (Gais, Italy) for supporting this investigation.
Funding
The work was financially supported by Zirkonzahn, Gais, Italy.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
For this type of study, formal consent is not required.
Rights and permissions
About this article

Cite this article
Schubert, O., Reitmaier, J., Schweiger, J. et al. Retentive force of PEEK secondary crowns on zirconia primary crowns over time. Clin Oral Invest 23, 2331–2338 (2019). https://doi.org/10.1007/s00784-018-2657-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-018-2657-x