
Abstract
Objectives
To compare the dimensions of maxillary sinuses in dentate and edentulous patients using cone beam computed tomography (CBCT) scans and a customised software program.
Materials and methods
This study comprised CBCTs of 50 dentate and 50 edentulous posterior maxillae. The observers drew two planar curves in all included sinuses in the frontal, sagittal and axial planes of the respective CBCT scans. The volume (mm3), surface (mm2) and maximum diameter (mm) of the sinuses were calculated using a custom-made software program. The variables analysed were the influence of the state of dentition on sinus dimensions (primary outcome) and the influence of age, gender and side on sinus dimensions; the time needed for analysis; and the intra- and inter-observer agreement (secondary outcomes).
Results
There was no difference in sinus dimensions between dentate and edentulous posterior maxillae. Males had significantly (p < 0.05) greater volume, surface and diameter than females. Strong intra- and inter-observer agreement (Pearson correlation) was found for the calculated sinus dimensions. The time needed per analysis was less than 4 min for both observers.
Conclusions
Being edentulous did not have an impact on the sinus dimensions, suggesting that there is no ongoing pneumatisation in the sinus after tooth loss. Males had larger sinuses than females in a population older than 30 years.
Clinical relevance
Following tooth loss in the posterior maxilla, vertical bone height is primarily lost due to resorption of the alveolar crest, and not due to pneumatisation of the maxillary sinus. The customised software program was found to be user-friendly and efficient.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The maxillary sinus has multiple functions, which include serving as a resonance body for the voice, contributing to the olfactory processes and adapting the temperature and humidity of inspired air before it passes into the bronchi and lungs. The maxillary sinus is already present at birth [1], but until eruption of the permanent teeth, its size remains negligible [2]. Its size increases through pneumatisation, with final dimensions being reached around the age of 18 [3,4,5,6,7].
It has been reported that another type of pneumatisation takes place after tooth extraction in the posterior maxilla, supported by remodelling on the floor of the maxillary sinus [8, 9]. As a consequence, the maxillary sinus may exhibit only a paper-thin cortical bone wall basally and on its lateral sides after tooth loss, especially in elderly people [2, 9, 10]. For patients with edentulous posterior maxillae, anatomical conditions for a planned implant therapy can be challenging. Sinus floor elevation (SFE) procedures may be needed prior to or at the same time as dental implant placement [5]. Cone beam computed tomography (CBCT) is considered an ideal imaging technique for preoperative analysis of the maxillary sinus in combination with diagnosis and treatment planning [11,12,13,14].
The aim of this study was to evaluate pneumatisation of the maxillary sinus following tooth loss. This analysis compared the volume, surface and maximum diameter of the sinuses of patients with a dentate or edentulous posterior maxilla, using CBCT and a customised software program. Secondary objectives included analysis of the influence of gender, age and sinus side on the dimensions of the maxillary sinus; the intra-observer and inter-observer variability in measurement of dimensions; and the time needed to conduct these analyses.
Material and methods
Study design and patient selection
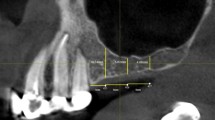
This retrospective case-control study is based on CBCT images from patients examined in the Section of Dental Radiology and Stomatology, Department of Oral Surgery and Stomatology, University of Bern. Out of this CBCT pool, a total of 100 cases were consecutively selected during the period from October 13, 2011, to May 2, 2016. The cases were grouped into 50 dentate posterior maxillae (all teeth present in the maxilla or all teeth present posterior to the maxillary canine) and 50 edentulous posterior maxillae (all teeth missing posterior to the maxillary canine or a completely edentulous maxilla). The inclusion criteria consisted of (1) patients older than 30 years with fully developed maxillary sinuses, (2) at least one maxillary sinus completely visible in the field of view (FOV), (3) maxillary sinus and alveolar crest free of any pathology, (4) no implant or graft in the posterior maxilla, (5) maxillary sinus without signs of previous sinus surgeries, (6) a maximum of 4 mm localised or generalised mucosal thickening of the Schneiderian membrane and (7) maxillary sinuses free of artefacts (acquisition or patient related) (Fig. 1). If both sinuses were visible on the CBCT scan, the maxillary sinus to be analysed in the present study was randomly chosen by the flip of a coin.

CBCT images (FOV, 8 × 5 cm) of coronal (a), sagittal (b), and axial (c) planes of a fully visible maxillary sinus (on the left) included in this study. The right maxillary sinus did not fulfil the inclusion criteria due to > 4 mm thickening of the Schneiderian membrane
The study protocol was approved by the local ethics committee of the state of Bern, Switzerland (approval number 384/14). The study was performed in accordance with the Declaration of Helsinki (2013 update, www.wma.net).
Radiographic imaging (CBCT) and analysis
CBCT scans were obtained using a 3D Accuitomo 170 unit (Morita Corp., Kyoto, Japan), recorded at 80 kV and 5.0 mA using variable FOVs (in cm) with the following corresponding voxel sizes (in mm): 6 × 6 cm (0.125 mm), 8 × 5 cm (0.160 mm), 8 × 8 cm (0.160 mm), 10 × 5 cm (0.250 mm), 10 × 10 cm (0.250 mm), 14 × 5 cm (0.250 mm), 14 × 10 cm (0.250 mm) and 17 × 12 cm (0.250 mm). The exposure time was 17.5 s for a 360° exposition. The data were reconstructed with slices at an interval of 0.5 mm.
For the assessment of the maxillary sinus dimensions (volume/surface/maximum diameter), a customised software program was developed in collaboration with Swissmeda AG (Zürich, Switzerland) using reconstructed CBCT data sets in a DICOM format [15]. For all analyses, the software program was installed on a Dell Precision T3500 workstation (Dell, Round Rock, Texas, USA) with a 19-in. EIZO FlexScan monitor (resolution of 1280 × 1024 pixels; EIZO Nanao AG, Wädenswil, Switzerland). First, a planar curve delineating the outlines of the maxillary sinus was drawn manually for all cases. For each plane, two or a maximum of three curves were drawn (Fig. 2a–f). Based on this information about a set of closed curves, each lying in a supporting plane, the software program estimated initial surface vectors, and the curves were adjusted at interceptions (Fig. 2g). A radial basis function with compact support was used to define an implicit form of the volume as a zero set of the radial basis function. The zero set was polygonalised by marching tetrahedrons in the bounding box of the curves. The accuracy of the volume was determined by the grid size of the marching tetrahedrons, the support grid of the radial basis functions and the sampling density of the curves [15]. For the sinus dimensions, the program produced a volume (in mm3), a surface (in mm2) and a maximum diameter (in mm). The software performed two outputs for each sinus. First, an initial calculation of the dimensions was generated (preview result; Fig. 2h). This was followed by a second, more time-consuming refined analysis (final result; Fig. 2i).

A customised software program (Swissmeda AG, Zürich, Switzerland) was used to calculate the volume, surface and maximum diameter of the maxillary sinuses included. Two planar curves delineating the maxillary sinus were drawn manually in the coronal (a, b), sagittal (c, d) and axial (e, f) planes and combined for further computing (g). Three-dimensional reconstruction of the volume, surface and maximum diameter of the maxillary sinus is shown for the preview (h) and the final result (i)
One calibrated and experienced observer (M.S.) performed all dimensional measurements twice to assess for repeatability (intra-observer reliability) of the values. Between the first and the second measurements, there was a time interval of at least 1 month. To test for inter-observer reliability (reproducibility), a second examiner (M.B.) independently assessed the dimensions of 20 randomly selected CBCT scans.
Statistical analysis
First, the data was analysed descriptively. For all dimensional outcomes (sinus volume, sinus surface and sinus maximum diameter), the mean, standard deviation, maximum, minimum and median were calculated. For the median, 95% confidence intervals based on the Mann-Whitney-Wilcoxon tests were determined. Linear models were used to quantify the effect of “dentate versus edentulous”, “gender”, “age” and “side” on the outcomes “volume”, “surface” and “maximum diameter” for both software outputs (preview and final). Aberrations were calculated as relative differences of both outputs and presented as a ratio. For analysis of age as an influencing factor, the data was divided into two groups (< 62 and ≥ 62 years; median split).
For both observers, the time needed (minutes and seconds) to produce the software outputs (preview and final) for the dimensions was given as mean, standard deviation, maximum, minimum and median values. Time aberrations of both outputs were calculated as relative differences and presented as a ratio. For the median, confidence intervals (95%) based on the Mann-Whitney-Wilcoxon test were calculated.
Intra- and inter-observer agreement for volume, surface, maximum diameter of the maxillary sinuses analysed and time needed for the analysis was analysed using Pearson correlations [16].
All results were calculated with R, 3.3.3 (R Foundation for Statistical Computing, Vienna, Austria). For all tests, a p value of < 0.05 was chosen as the level of significance.
Results
Population under investigation
Of the 100 patients included, 66 were women and 34 were men (female-to-male ratio of 2:1). The mean age was 60.89 years (range 32 to 91 years; Table 1). Both maxillary sinuses were completely visible in 22 CBCT scans and only one sinus in 78. Of a total of 100 sinuses, 59 were from the right side and 41 from the left. Of the 59 right sinuses, 29 exhibited a dentate and 30 an edentulous posterior maxilla. Of the 41 left sinuses, 21 exhibited a dentate and 20 an edentulous posterior maxilla. The most frequent indication for CBCT imaging in the 100 included patients was treatment planning prior to implant placement (47%; n = 47).
Volumes, surfaces and maximum diameters of maxillary sinuses
The preview and final results of all patients showed mean maxillary sinus volumes of 16,260.90 and 16,511.19 mm3, respectively. The mean surface was 3697.14 mm2 (preview) and 3777.74 mm2 (final), and the mean maximum diameters were 40.20 mm (preview) and 40.50 mm (final). The relative aberration between preview and final outputs was 1% for the mean surface and diameter and 2% for the mean volume (Table 2).
For the primary outcome variable, there was no association between the state of dentition (dentate/edentulous) and the volume (p = 0.0630), the surface (p = 0.1278) or the maximum diameter (p = 0.0841) of the maxillary sinuses analysed (Table 3). For secondary outcomes, there was no association between the dimensions of the maxillary sinuses and age or side (right/left sinus). Gender showed a significant association for sinus dimensions. Being male resulted in a significantly larger volume (p = 0.0160), surface (p = 0.0083) and diameter (p = 0.0016; Table 3).
Intra- and inter-observer reliability (reproducibility)
For observer I (M.S.), the Pearson correlations exhibited a strong intra-observer correlation between the first and the second sessions in terms of volume, surface and maximum diameter of the sinus analysed (Table 4). The 20 randomly selected cases analysed by observer II (M.B.) showed a strong inter-observer correlation for the dimensional values.
The time needed for the dimensional analyses was less than 4 min for all cases for both observers. Generally, observer I obtained software outputs (preview and final) faster than observer II. The mean time for obtaining previews was 122.40 s (observer I) versus 155.10 s (observer II), and the mean time for the final outputs was 177 s (observer I) versus 192 s (observer II) (Table 5). The inter-observer correlation for the time needed to obtain the preview software output showed a moderate (0.36) correlation, and that for the final software output showed a weak correlation (0.15).
Discussion
There was no significant association between the state of the dentition (dentate versus edentulous) and the volume, the surface or the maximum diameter of the included maxillary sinuses. Furthermore, secondary outcomes analysed showed no association between the dimensional measurements of the sinuses and the age or the sinus side (right/left). Gender was significantly associated with volume, surface and maximum diameter of the maxillary sinuses, with men exhibiting larger values than females. The intra- and inter-observer reliability (reproducibility) for the dimensional measurements was strong. The time needed for volume, surface and diameter analysis using the customised software program was less than 4 min for every case evaluated by both trained observers.
Until eruption of the permanent teeth, the size of the maxillary sinus remains negligible [2]. Later, the maxillary sinus expands actively, reaching its definitive shape after completion of the second dentition at the age of 13, with the end of growth of the midface and eruption of the maxillary teeth. Around the age of 18, the maxillary sinus reaches its final size [3,4,5,6,7, 17].
In addition to this growth-driven pneumatisation, sinus expansion is also observed after tooth extraction in the posterior maxilla of adults due to remodelling and resorption processes on the floor of the sinus [9, 10]. It has been suggested that the presence of osteoclasts in the endosteal cells of the Schneiderian membrane allows an expansion of the sinus into the alveolar process of the maxilla following tooth loss, which may be promoted due to a lack of resistance in this region [5, 9]. Another factor contributing to this process may be reduced occlusal loading following tooth extraction in the posterior maxilla, and the resulting bone remodelling and resorption processes leading to atrophy of the alveolar process [18]. Wehrbein and Diedrich [19] suggested furthermore that pneumatisation processes are influenced by genetic factors and disposition, growth patterns and an open ostium. Some authors have stated further that a slight increase in intra-antral pressure can cause enlargement in the volume of the maxillary sinus after growth has ceased [9, 19].
The present study showed that the volume, surface and maximum diameter of the maxillary sinus are greater in males than in females. Age, side and being edentulous did not have an impact on the sinus dimensions in the present study, suggesting that there is no ongoing pneumatisation process in the sinus after tooth loss. These findings are corroborated by Uchida and co-workers [7], who analysed the volume and dimensions of 59 maxillary sinuses in 32 human cadavers by producing casts with dental impression material. As in the present study, they found no significant differences in the volumes of maxillary sinuses with regard to side (right/left) or age, but in contrast to the present study, there was no difference in sinus volumes between genders. Ariji and co-workers [20] analysed sinus dimensions with traditional CT scans, including 194 maxillary sinuses of 115 patients ranging in age from 4 to 94. Ninety-seven patients were older than 20 years and subdivided into a dentate (133 sinuses) and an edentulous (61 sinuses) group. Similar to the present analysis, the authors found no significant difference in the mean volume between right and left sinuses. Nevertheless, they observed an increase in the maxillary sinus volume until the age of 20 years and a decrease afterwards. As in the present study, there was no significant difference in the mean volume for dentate and edentulous patients aged 50–79 years. And in contrast to the present study, no difference between genders was found in the dimensions of the sinus [20].
Limitations of the present study were the lack of a sample size calculation and that the two groups assessed (dentate and edentulous maxillae) were not matched in terms of age. Due to its retrospective nature, the limiting factor for inclusion of cases was the availability of CBCTs exhibiting an entire maxillary sinus in edentulous patients. Thus, the inclusion of 50 edentulous and 50 dentate cases was based on the assumption that if there would be no difference between the 50 cases in each group for the primary outcome, an eventual statistically significant difference of a larger sample might be of very limited clinical relevance. Furthermore, previous studies either had more [20] or less [7, 19] maxillary sinuses included for volume analysis. The difference of the two groups concerning the age was because patients without teeth were generally distinctly older than patients with all teeth present in the posterior maxilla.
To quantify the progressive pneumatisation process in maxillary sinuses after tooth extraction, Wehrbein and Diedrich [19] examined 32 panoramic radiographs of adults before and during/after orthodontic space closure treatment by superimposing them. In contrast to the present study, the authors found progressive pneumatisation in the maxillary sinus, especially in the molar region. Nevertheless, these results have to be interpreted with caution, as panoramic radiographs have limited diagnostic capability and poor reliability for detecting anatomic structures in maxillary sinuses [19, 21,22,23].
The resorption process after tooth extraction in the upper posterior region can be so pronounced that the alveolar ridge disappears nearly completely. Then, only a paper-thin cortical basal and lateral bone wall remains on the sinus [2, 9, 10]. Implant therapy will be more challenging in such atrophic cases, as SFE procedures may be needed for dental implant placement [10, 24]. When SFE procedures are needed and in all complex implant cases, a preoperative CBCT is advantageous. It delivers detailed radiographic visualisation and determination of ridge dimensions, allows examination of the maxillary sinus and related anatomical structures and pathologies and has been recommended in recent guidelines [14, 25, 26]. Furthermore, maxillary sinus diagnostics using CBCT imaging have also been suggested for the analysis of oro-antral communications to localise dislocated foreign bodies and teeth in the maxillary sinus and before apical surgery [19, 27,28,29,30].
Recent studies have also measured volumes in CBCTs using different software calculations, for example volume changes before and after grafting procedures like SFE, volume of extraction sockets or volume of intra-osseous pathologies like cysts [15, 31,32,33]. In the study by Suter and co-workers [15], the methodology used to assess dimensions of nasopalatine duct cysts was similar to that of the present study [15]. To the best of our knowledge, there are not many options yet to work with a semi-automated software program generating three-dimensional volume calculations based on CBCT images, without relying on a subtraction technique or on stacking multi-segmented 2D slices. For this study, the semi-automated software program used by Suter and co-workers [15] was further refined to make it suitable for sinus volume calculations and to generate accurate and not too time-consuming outputs. This is of importance as computer-aided diagnostic software options will only be integrated in daily clinical practice if they are easy to use and do not result in a loss of time.
Therefore, the time needed for the dimensional analyses until result output was also measured in this study. Observer I was faster than observer II, with a moderate inter-observer correlation for the preview and a weak inter-observer correlation for the final output. The first observer was an experienced clinician trained specifically in the use of this software program. The second observer was an experienced clinician too, but not particularly trained in the use of this specific software. While observer I measured the 100 cases twice, observer II only measured 20 randomly selected sinuses once. The intra-observer reliability (repeatability) for the volume, surface and maximum diameter software outputs (preview and final) exhibited strong values (0.99, 0.99), which were similar to the inter-observer reproducibility (0.99, 0.99). This proves the reliability of repeated measurements using this customised software program but also demonstrates that the software is associated with a learning curve and users may become faster in performing the measurements over time. Nevertheless, the time needed for the dimensional analyses based on CBCT scans was less than 4 min for all cases included by both observers, which seems to be a reasonable time for daily use in clinical practice as well. Interestingly, the time needed to perform a specific procedure is one of the major thresholds for implementation in daily practice.
Conclusions
On the basis of the data analysed in the present study, the following can be concluded:
-
The state of dentition (dentate versus edentulous) in the posterior maxilla did not influence the volume, surface or diameter of the maxillary sinus in an analysis based on CBCT scans.
-
Patient age had no significant influence on the sinus dimensions in a pool of patients older than 30 years.
-
Being male had a significant influence on the sinus volume, surface and diameter.
-
The time needed to analyse the volume, surface and diameter of sinuses based on CBCT scans and with the help of a customised software program was less than 4 min for all cases included by two trained observers, and there was a strong intra- and interrater correlation for these measurements.
References
Jovanovic S, Jelicic N, Kargovska-Klisarova A (1984) Le développement post-natal et les rapports du sinus maxillaire. Acta Anat 118:122–128
Kao SY, Lui MT, Cheng DH (2014) Lateral trap-door window approach with maxillary sinus membrane lifting for dental implant placement in atrophied edentulous alveolar ridge. J Chin Med Assoc 5:1–4. https://doi.org/10.1016/j.jcma.2014.05.016
Kittel G, Göhr H (1955) Bestimmungen von Nasennebenhöhlengrössen. Z Laryng Rhinol 44:59–66
Heyne HJ, Fanghänel J (1972) Zur Anatomie der menschlichen Nasennebenhöhlen. 1. Räumliche Darstellungen. 2. Volumetrie. Anat Anz 130:132–157
Chanavaz M (1990) Maxillary sinus: anatomy, physiology, surgery, and bone grafting related to implantology: eleven years of surgical experience (1979-1990). J Oral Implantol 16:199–209
Anagnostopoulou S, Venieratos D, Spyropoulos N (1991) Classification of human maxillary sinuses according to their geometric features. Anat Anz 173:121–130
Uchida Y, Goto M, Katsuki T, Akiyoshi T (1998) A cadaveric study of maxillary sinus size and aid in bone grafting of the maxillary sinus floor. J Oral Maxillofacial Surg 56:1158–1163
Kraut R, Kessler H (1989) Quantification of bone in dental implant sites after composite grafting of the mandible. Int J Oral Maxillofac Implants 4:143
Smiler DG, Johnson PW, Lozada JL, Misch C, Rosenlicht JL, Tatum OH Jr, Wagner JR (1992) Sinus lift grafts and endosseous implants. Treatment of the atrophic posterior maxilla. Dent Clin N Am 36:151–186 discussion 187-188
Raja SV (2009) Management of the posterior maxilla with sinus lift: review of techniques. J Oral Maxillofac Surg 67:1730–1734. https://doi.org/10.1016/j.joms.2009.03.042
Dobele I, Kise L, Apse P, Kragis G, Bigestans A (2013) Radiographic assessment of findings in the maxillary sinus using cone-beam computed tomography. Stomatologija 15:119–122
Bornstein MM, Scarfe WC, Vaughn VM, Jacobs R (2014) Cone beam computed tomography in implant dentistry: a systematic review focusing on guidelines, indications, and radiation dose risks. Int J Oral Maxillofac Implants 29(Suppl):55–77. https://doi.org/10.11607/jomi.2014suppl.g1.4
Bornstein MM, Al-Nawas B, Kuchler U, Tahmaseb A (2014) Consensus statements and recommended clinical procedures regarding contemporary surgical and radiographic techniques in implant dentistry. Int J Oral Maxillofac Implants 29(Suppl):78–82. https://doi.org/10.11607/jomi.2013.g1
Bornstein MM, Horner K, Jacobs R (2017) Use of cone beam computed tomography in implant dentistry: current concepts, indications and limitations for clinical practice and research. Periodontol 2000 73:51–72. https://doi.org/10.1111/prd.12161
Suter VG, Warnakulasuriya S, Reichart PA, Bornstein MM (2015) Radiographic volume analysis as a novel tool to determine nasopalatine duct cyst dimensions and its association with presenting symptoms and postoperative complications. Clin Oral Investig 19:1611–1618. https://doi.org/10.1007/s00784-014-1391-2
Kosfeld R, Eckey HF, Türck M, Eckey HF, Türck M (2008) Deskriptive Statistik: Grundlagen – Methoden - Beispiele - Aufgaben. 5. Aufl. Springer, Berlin
Stern L (1939) Roentgenologische Betrachtung der Entwicklung und Ausdehnung der Nasennebenhöhlen. HNO 30:169–199
Pfyffer A (1951) Über die Spätfolgen der Sechsjahrmolar-Extraktion. Schweiz Monatsschr Zahnheilkd 61:565–590
Wehrbein H, Diedrich P (1992) Die fortschreitende Pneumatisation der basalen Kieferhöhle nach Extraktion und Lückenschluss. Fortschr Kieferorthop 53:77–83
Ariji Y, Kuroki T, Moriguchi S, Ariji E, Kanda S (1994) Age changes in the volume of the human maxillary sinus: a study using computed tomography. Dentomaxillofac Radiol 23:163–168
Kasabah S, Slezák R, Simünek A, Krug J, Lecaro MC (2002) Evaluation of the accuracy of panoramic radiograph in the definition of maxillary sinus septa. Acta Med (Hradec Kralove) 45:173–175
González-Santana H, Peñarrocha-Diago M, Guarinós-Carbó J, Sorní-Bröker M (2007) A study of the septa in the maxillary sinuses and the subantral alveolar processes in 30 patients. J Oral Implantol 33:340–343. https://doi.org/10.1563/1548-1336(2007)33[340:ASOTSI]2.0.CO;2
Maestre-Ferrín L, Carrillo-García C, Galán-Gil S, Peñarrocha-Diago M, Peñarrocha-Diago M (2011) Prevalence, location, and size of maxillary sinus septa: panoramic radiograph versus computed tomography scan. J Oral Maxillofac Surg 69:507–511. https://doi.org/10.1016/j.joms.2010.10.033
Garg AK (1999) Augmentation grafting of the maxillary sinus for the placement of dental implants: anatomy, physiology, and procedure. Implant Dent 8:36–46
Harris D, Buser D, Dula K, Gröndahl K, Harris D, Jacobs R, Lekholm U, Nakielny R, van Steenberghe D, van der Stelt P (2002) E.A.O. guidelines for the use of diagnostic imaging in implant dentistry. A consensus workshop organized by the European Association for Osseointegration in Trinity College Dublin. Clin Oral Implants Res 13:566–570
Harris D, Horner K, Gröndahl K, Jacobs R, Helmrot E, Benic GI, Bornstein MM, Dawood A, Quirynen M (2012) E.A.O. guidelines for the use of diagnostic imaging in implant dentistry 2011. A consensus workshop organized by the European Association for Osseointegration at the Medical University of Warsaw. Clin Oral Implants Res 23:1243–1253. https://doi.org/10.1111/j.1600-0501.2012.02441.x
Jerome CE, Hill AV (1995) Preventing root tip loss in the maxillary sinus during endodontic surgery. J Endod 21:422–424
Ziegler CM, Woertche R, Brief J, Hassfeld S (2002) Clinical indications for digital volume tomography in oral and maxillofacial surgery. Dentomaxillofac Radiol 31:126–130
Sharan A, Madjar D (2008) Maxillary sinus pneumatisation following extractions: a radiographic study. Int J Oral Maxillofac Implants 23:48–56
Wolf MK, Rostetter C, Stadlinger B, Locher M, Damerau G (2015) Preoperative 3D imaging in maxillary sinus: brief review of the literature and case report. Quintessence Int 46:627–631. https://doi.org/10.3290/j.qi.a33930
Agbaje JO, Jacobs R, Maes F, Michiels K, van Steenberghe D (2007) Volumetric analysis of extraction sockets using cone beam computed tomography: a pilot study on ex vivo jaw bone. J Clin Periodontol 34:985–990
Kim ES, Moon SY, Kim SG, Park HC, Oh JS (2013) Three-dimensional volumetric analysis after sinus grafts. Implant Dent 22:170–174. https://doi.org/10.1097/ID.0b013e31827f3576
Mazzocco F, Lops D, Gobbato L, Lolato A, Romeo E, del Fabbro M (2014) Three-dimensional volume change of grafted bone in the maxillary sinus. Int J Oral Maxillofac Implants 29:178–184. https://doi.org/10.11607/jomi.3236
Acknowledgments
The authors thank M. Gabriel Fischer, significantis GmbH, Herzwil b. Köniz, Switzerland, for his assistance with the statistical analysis.
Funding
This study was funded by a grant from the Swiss Association of Dentomaxillofacial Radiology (grant number 15/01).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This study was reviewed and approved by the local ethics committee of the State of Bern, Switzerland (approval number 384/14). All procedures in this retrospective study were conducted in accordance with the Declaration of Helsinki (1964) and its later amendments.
Informed consent
For this type of study (retrospective study), formal consent is not required.
Rights and permissions
About this article

Cite this article
Schriber, M., Bornstein, M.M. & Suter, V.G.A. Is the pneumatisation of the maxillary sinus following tooth loss a reality? A retrospective analysis using cone beam computed tomography and a customised software program. Clin Oral Invest 23, 1349–1358 (2019). https://doi.org/10.1007/s00784-018-2552-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-018-2552-5