
Abstract
Objectives
The purpose of this systematic review was to compare the clinical performance of bulk-fill resin composites with conventional resin composites used for direct restorations of posterior teeth.
Methods
This review followed the PRISMA statement. This review was registered at PROSPERO (registration number CRD42016053436). A search of the scientific literature was performed by two independent reviewers using the PubMed/MEDLINE, Embase, The Cochrane Library, and Web of Science databases from commencement until January 2018. The research question was “Do bulk-fill resin composites have a clinical performance comparable to conventional resin composites in posterior restorations?” Only studies evaluating class I and II direct restorations in permanent teeth with a follow-up period of at least 1 year were included. The RevMan 5 program was used for meta-analysis, calculating the relative risk (RR) and 95% confidence interval (CI) of the dichotomous outcome (restoration failure or success).
Results
Ten articles were selected, comprising 941 analyzed restorations. The mean follow-up period was 33.6 months (12–72 months). No statistically significant differences in the failure rate were observed between conventional and base/flowable bulk-fill resin composites (p = 0.31; RR 1.49; 95% CI 0.69–3.25) or full-body/sculptable bulk-fill resin composites (p = 0.12; RR 1.89; 95% CI 0.84–4.24).
Conclusions
The present systematic review and meta-analysis indicate similar clinical performances of bulk-fill and conventional resin composites over a follow-up period of 12 to 72 months.
Clinical significance
Based on the results of this study, the bulk-fill resin composites could be an alternative for direct restorations in posterior teeth. However, clinical trials of longer duration are required.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Clinical evidence for the overall survival of direct light-cured resin composites restorations in posterior teeth has been well documented [1,2,3,4,5]. This material is considered to be the first choice for esthetic restorations in posterior teeth [6].
The main reasons for the clinical failure of direct resin composite restorations in posterior teeth over time are secondary caries and restoration fractures [1, 3]. Resin composite shrinkage stress may lead to the development of marginal gaps at the tooth–restoration interface, which may result in the development of secondary caries. Conversely, the occurrence of fractures is associated with the limitations of the materials’ mechanical properties, cavity configuration, quantity and quality of the remnant tooth structure, and a patient’s occlusion [7,8,9]. To reduce the polymerization shrinkage stress, incremental layering of the resin composites has been recommended for decades. The incremental technique reduces stress at the cavity wall interface and allows a more efficient light curing of the material and a lower gap formation at the interface [10,11,12].
Bulk-fill resin composites have been designed to simplify the restorative technique because they can be placed into posterior teeth cavities in a single increment of 4–5 mm [13,14,15]. These materials offer greater translucency, allowing greater light dissipation through the material; incorporation of more reactive photoinitiators, which enable a greater depth of cure; and include monomers that act as modulators of the polymerization reaction, achieving low polymerization shrinkage [8, 16]. Two types of these materials are commercially available: base and full-body bulk-fill resin composites. Base bulk-fill materials are low-viscosity resin composites and therefore are also known as flowable bulk-fill resin composites [17]. These materials involve lower filler loading than conventional/standard microhybrid or nanohybrid resin composites, which require incremental filling. Therefore, they are used as a liner/ base, followed by capping with the conventional resin composites. Full-body bulk-fill resin composites can be applied in one increment without the need for coverage or capping. Because of their viscosity, they are also referred to as sculptable or paste-like bulk-fill resin composites, allowing the reconstruction of the lost tooth structures. In addition, these materials have high inorganic filler loading and are therefore used in areas of high masticatory load [17,18,19,20].
The simplification of the operative procedures is desirable in clinical daily practice. In this context, bulk-fill resin composites are an attractive alternative for posterior restorations. However, a clearer understanding of the clinical performance of this relatively new class of materials in comparison to conventional resin composites is required. Therefore, the aim of the current systematic review and meta-analysis was to compare the clinical performance of bulk-fill and conventional resin composites in direct restorations in posterior teeth. The hypothesis of this study was that the clinical performance of these restorative materials is similar.
Materials and methods
Protocol and registration
This review was conducted following the recommendations of the Cochrane Collaboration for systematic reviews [21] and is reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [22]. The study was registered at the international prospective register of systematic reviews—PROSPERO under the registration number CDR42016053436.
Eligibility criteria
The research question of this study was “Do bulk-fill resin composites have a comparable clinical performance to conventional composites in posterior restorations?” The population/problem, intervention/exposure, comparison, and outcome of the study were established according to the PICO question. In this respect, the population consisted of patients with direct resin restorations in permanent posterior teeth. The intervention was posterior teeth restored with a bulk-fill resin composite, and a comparison was performed with posterior teeth restored with a conventional resin composite. Evaluated outcomes were failure such as anatomical shape, marginal adaptation and discoloration, surface roughness, color, secondary caries, loss of retention, fracture, and postoperative sensitivity.
The inclusion criteria used were as follows: (1) only randomized clinical trials (RCTs), (2) studies with a follow-up period of at least 1 year, and (3) studies evaluating class I and II direct restorations in permanent teeth restored with bulk-fill and conventional resin composites.
The exclusion criteria were as follows: (1) prospective studies without randomization and retrospective studies, (2) case reports, (3) reviews, (4) in vitro studies, and (5) studies reported in more than one publication with different follow-up periods, and studies evaluating only bulk-filled resin restorations without direct comparison with conventional resin composites.
Information sources and search strategy
The databases searched were PubMed/MEDLINE, Excerpta Medica Database (Embase), Cochrane Library, and Web of Science. The search strategies for each database are represented in Tables 1, 2, 3, and 4. A manual search through journals in the area of interest, even if they are indexed in the research databases, is recommended as an additional form of search [23,24,25]. Therefore, the electronic search was complemented by manual searches of the following journals: Journal of Orofacial Sciences, Operative Dentistry, Dental Materials, and Journal of Dentistry. Additionally, the reference lists of the included studies were checked to identify possible relevant studies. The electronic search was performed up to January 2018 and without any language restrictions.
Study selection and data collection
Two independent researchers (S.R.M.V. and C.A.A.L.) performed the electronic search, selecting studies based on titles and abstracts that answered the research question. Relevant information extraction, as well as an assessment of the risk of bias of the articles, were performed by one of the researchers (S.R.M.V.) and verified by a second researcher (C.A.A.L.). Disagreements between the evaluators were resolved by consensus.
Relevant information was extracted using a form containing questions regarding the author, study design, number of patients and restorations, mean age, follow-up, bonding agent and resin composites of the control and intervention groups, number of surfaces and restoration locations, and restoration failures [26].
Risk of bias in individual studies
The risk of bias of the selected articles was assessed using the Cochrane risk of bias tool for randomized clinical trials, which uses a domain-based approach [21]. In this tool, the aspects of bias risk are evaluated individually without assigning scores and are divided into six domains: random sequence generation, allocation concealment, blinding of outcome assessors, blinding of participants and personnel, incomplete outcome data, and selective outcome reporting, comprising the assessment of selection, performance, attrition, reporting, and detection bias. Each domain is classified as having a low risk, unclear risk, or high risk of bias.
Summary measures
The data extracted were analyzed using the Review Manager (RevMan) 5.3 software (The Cochrane Collaboration, Copenhagen, Denmark). The relative risk (RR) and 95% confidence interval (CI) were calculated for each study. The data of the eligible studies were ordinal, referring to the scores for the characteristics of the restorations evaluated using the modified versions of the U.S. Public Health Service (USPHS) (Table 5). For further analysis, these data were dichotomized as either acceptable or unacceptable. The acceptable restorations were those that received the Alpha and Bravo scores. The unacceptable restorations were those that received the Charlie and Delta score in at least one of the characteristics. Therefore, failed restorations were those that were classified as unacceptable.
The I2 index was used to measure the percentage of variation across studies that was due to heterogeneity, where 25% corresponded to low heterogeneity, 50% to moderate heterogeneity, and 75% to high heterogeneity. A fixed-effect model was used because no statistically significant heterogeneity was found among the studies (p > 0.10) [37].
Additional analysis
The kappa coefficient was calculated to determine inter-reader agreement in the initial selection of the articles in the PubMed/MEDLINE, Embase, The Cochrane Library, and Web of Science.
Results
Selection of studies
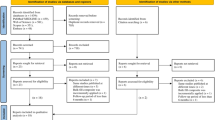
The initial search of the databases retrieved 522 articles, including 300 in PubMed/MEDLINE, 79 in Embase, 16 in Cochrane Library, 127 in Web of Science, and 2 in the manual search (Fig. 1). After the removal of duplicates, 356 articles remained and 15 were selected based on the research question. After reading the full text, five articles were excluded; one was excluded because of a short follow-up period (30 days) [38] and the other four were excluded because they contained the data reported in another study with a longer follow-up period [39,40,41,42]. Thus, 10 articles were selected for final analysis of the results. The kappa test was applied to determine inter-reader agreement in the initial selection of the studies, which showed a high level of agreement for PubMed/MEDLINE (kappa = 0.9), Embase (kappa = 1.0), The Cochrane Library (kappa = 1.0), and Web of Science (kappa = 0.83) [43].

Flow diagram of the article selection process
Characteristics of included studies
Ten studies were selected for qualitative and quantitative analysis. A total of 1076 restorations were performed in 459 patients, and 941 restorations were evaluated. Nine studies were split-mouth studies [27,28,29,30,31,32,33,34, 36] and one was a parallel group study [35]. The mean follow-up was 33.6 months (12–72 months). Five studies [27, 30, 32,33,34] did not report sample size calculation.
Rubber dam isolation was only reported in four studies [30, 34,35,36]; the remaining six studies used only cotton rolls and saliva ejectors. In one of these four studies [30], rubber dam isolation was only employed only when cotton rolls/saliva ejector were insufficient. Most studies did not report the use of a lining material. In two studies [27, 32], used calcium hydroxide cement was used as a liner in deep cavities, and in one study [33], calcium hydroxide cement and/or glass ionomer cement was used in deeper cavities. Regarding the bonding agent used, self-etch systems were used in both the intervention and control groups of six studies [27,28,29, 32,33,34], three studies [31, 35, 36] used etch-and-rinse systems, and one study [30] used an etch-and-rinse system in the control group and a self-etch system in the intervention group. All base/flowable bulk-fill resin composites were used with a 2-mm capping of a conventional resin composite [28, 29, 31]. One study [27] evaluated four groups: two full body/sculptable bulk-fill composites, a base/flowable bulk-fill composite covered with a conventional resin composite, and a conventional resin composite by itself. The remaining studies [30, 32,33,34,35,36] compared full-body/sculptable bulk-fill resin composites with conventional composites (incremental technique) (Table 6).
Among the 941 restorations evaluated, 43 failures occurred, with a 5.57% (29 of 520) failure rate in bulk-fill resin composites and a 3.32% (14 of 421) failure rate in conventional resin composites. The causes of restoration failure were secondary caries (23%; n = 10), tooth and resin fractures (19%; n = 8, each), postoperative sensitivity (9%; n = 4), anatomical shape and poor marginal adaptation (7%; n = 3, each), marginal discoloration (9%; n = 4), caries associated with tooth fracture (5%; n = 2), and retention (2%; n = 1) (Table 7).
Assessment of risk of bias
Six of the included studies did not describe the randomization process. Karaman et al. [31], Arhun et al. [32], and Çolak et al. [33] used coin tossing for randomization, and Yazici et al. [36] used a random number table of the groups. None of the studies mentioned the method used for allocation concealment. Four studies were unclear about the blinding of participants and personnel [30, 33,34,35], and the other studies reported that patients were blinded. Only one study was unclear about the blinding of outcome assessment [35]. The incomplete outcome data domain was unclear in four studies [27, 31, 32, 36] because of unexplained reasons for participant loss. All studies had a low risk of bias regarding selective reporting. Even when the study protocol was unavailable, it was clear that the published reports clearly included all expected outcomes, including those that were prespecified [21] (Fig. 2).

Risk of bias of the included studies
Meta-analysis
The meta-analysis included the 10 studies selected in the systematic review. The failure rates of bulk-fill and conventional resin composite restorations were evaluated using subgroups for the classification of the bulk-fill resin composites (base/flowable and full-body/sculptable). No significant differences were observed between conventional resin composites and base/flowable (p = 0.31; RR 1.49; 95% CI 0.69–3.25; p = 0.10; I2 = 56%) or full-body/sculptable bulk-fill resin composites (p = 0.12; RR 1.89; 95% CI 0.84–4.24; p = 0.51; I2 = 0%) (Fig. 3).

Forest plots of included studies
Publication bias
A funnel plot was used for assessing the publication bias. The funnel plot of the studies included in this review exhibited symmetry, indicating low heterogeneity and the possible absence of publication bias (Fig. 4).

Funnel plot
Discussion
The hypothesis of this study was not rejected. The clinical performance of bulk-fill resin composites is comparable to conventional resins in direct posterior restorations. The studies included in this review reported similar results with the use of bulk-fill resin composites, regardless of type (base/flowable and full-body/sculptable).
The greater translucency of bulk-fill resin composites [8, 44] and the use of more reactive photoinitiators [16] allow a higher depth of cure. The higher reactiveness enables the insertion of the material in thick increments of 4–5 mm, with uniform polymerization and degree of conversion. These factors are essential to obtaining satisfactory mechanical properties and, consequently, increasing the longevity of the restorations [45, 46]. In addition, bulk-fill resin composites contain polymerization modulators that achieve low contraction and less stress at the bonded interface [8, 16, 47]. The insertion of thicker increments also contributes to reducing the incorporation of air voids, forming a more homogeneous restorative unit [8, 16].
The longevity of restorations is also related to the operative technique, as well as the patients’ and cavity characteristics [27]. In this respect, a larger number of failures in restorations of posterior teeth seem to be related to parafunctional habits such as bruxism [5]. Van Djiken and Pallesen [28, 29] reported a considerable significant number of failures caused by fracture of the material and tooth, most of which occurred in patients with bruxism.
Failure caused by secondary caries was considered in the studies when it was clinically observed in continuity with the margins of the evaluated restoration [26]. Secondary caries can be associated with the presence of marginal defects in a restoration [6, 9] or with high caries risk patients [48]. However, characteristics such as a high caries index and poor oral hygiene were considered exclusion criteria in most studies [27, 30,31,32,33,34,35,36]. Van Djiken and Pallesen [28, 29] did not exclude patients with this condition and confirmed that failure caused by secondary caries was associated with patients at high risk of caries. Thus, secondary caries may be related to biological failure rather than with the restorative material used [5, 48, 49]. The presence of secondary caries may also be related to problems of marginal adaptation and local failures such as contamination with saliva during the restorative procedure [27]. A previous systematic review [50] observed that direct restorations performed with rubber dam isolation resulted in a lower failure rate than restorations performed with only cotton rolls and saliva ejectors.
The location and number of surfaces involved, as well as the extent of the cavities, also appear to be related to the overall survival of restorations. The studies included in this review evaluated class I and II direct restorations in posterior teeth (molars and premolars). Five studies evaluated only class II restorations. Three studies did not report failure in class I restorations [28, 29, 34] and two other studies did not observe any failure in class II restorations over the follow-up period [31, 36]. Class II restorations appear to be more prone to the development of secondary caries compared to class I restorations [48]. Thus, the failure rate seems to be lower for cavities where only one surface is affected instead of two [3].
Cavity depth [51] and extent [52] are factors that can influence postoperative sensitivity. Apart from the study conducted by Karaman et al. [31], which used endodontically treated teeth, only one study [34] radiographically confirmed that all were performed in 4- to 5-mm-deep cavities, and all other studies evaluating postoperative sensitivity did not describe the depth of the preparations. Two studies [28, 29] reported that most cavities were deep. Nevertheless, a low rate of failure caused by postoperative sensitivity was observed in the included studies. This result should be carefully analyzed because one study [35] contained many reports of an initial sensitivity with a Bravo score that then regressed but did not receive a Charlie score (intense and intolerable sensitivity).
The small number of failures caused by postoperative sensitivity may be associated with the use of lining materials in deep cavities [27, 33] and the use of self-etch adhesive systems [30]. Conversely, a systematic review found no statistically significant relationship between postoperative sensitivity and the bonding system used [53]. No association was found between the placement technique of the bulk-fill resin composite (incremental and bulk-filling) and the cavity depth on the postoperative sensitivity [52]. A Cochrane review found inconsistent evidence regarding the use of liners and restoration failure, particularly concerning postoperative sensitivity [54].
Air entrapment between increments can occur when the incremental technique is used, causing sensitivity and degradation of the restorative material degradation [10, 11, 16]. Although no differences were observed between bulk-fill and conventional resin composites, the lower technical sensitivity and the simplified procedure of the former support its use in restorations of posterior teeth.
Randomized clinical trials are a critical method for clinically evaluating new materials and treatments because they are standardized to achieve greater significant credibility and clinical reliability. However, a detailed description and similar methods should be employed to allow this comparison. All studies included in this review used the modified USPHS criteria, but observed variations resulted in a lack of standardization among the studies. Thus, the different analyzed aspects and various instruments and assessment criteria used hampered the comparison of the results.
The USPHS criteria are the most common method for evaluating restorations. However, they have shown a limited sensitivity, and the categories may not fully reflect the clinical success of restorations. Clinical trials that have used other criteria tend to detect failure rates more than four times higher than produced by the USPHS. However, this may be due not only to the greater sensitivity of these criteria but also to a large number of other factors, such as the fact that not all new systems are fully validated [55]. The World Dental Federation (FDI) criteria have been reported as an alternative. The categories can be selected according to the objective of the study, and the scores of 1 to 3 can also be simplified and considered as “clinically satisfactory” [56].
Similarly, the randomization procedure and allocation concealment are fundamental to the design of randomized clinical trials to avoid selection bias. Most of the included studies did not provide a full description of these steps. Göstemeyer et al. [55] reviewed the design and validity of randomized controlled dental restorative trials and observed a high risk of bias, mainly in the domains of allocation concealment (selection bias 93%) and blinding of participants and personnel (performance bias 99%) or blinding of outcome assessment (detection bias 46%). The blinding of the operator and examiners may, in certain cases, be more difficult or even impossible to do depending on the studied materials. However, allocation concealment can be implemented in all trials.
Sample size calculation was also not clearly described in five of the included studies [27, 30, 32,33,34]. In a previous review [55] of 114 studies, only 17% reported sample size calculations, with relatively small sample sizes varying from 8 to 456 participants (median 37). Additionally, most studies described sample size calculation inadequately. Although the absence of sample size calculation does not affect the risk of bias of clinical trials, it may result in underpowered studies that are unethical and wastes considerable resources. Small samples are unable to highlight small differences in the results [55, 57].
Thus, the results indicated the lack of adherence of the authors to the Consolidated Standards of Reporting Trials (CONSORT) statement for clear and transparent reporting of a randomized clinical trial, which would have aided the reader in forming a judgment and conclusions [58].
The follow-up periods observed in this study varied from 12 to 72 months. Differences in the efficacy of therapies can only be measured only after several years because failure behavior can vary, and one type of material may be more susceptible to long-term dental fracture and the other caries. Therefore, long periods of observation are essential (often more than 10 years) to observe all pertinent effects and differences. However, maintaining a population of participants over a prolonged period is extremely challenging, and attrition bias is very common [56].
The results of the present review should be interpreted with caution because of the small number of clinical studies evaluated. Further randomized clinical trials with longer observation periods are still needed before a full recommendation of clinical protocol change regarding direct restorations of posterior teeth with resin composites.
Conclusion
This systematic review and meta-analysis revealed that the clinical performance of bulk-fill and conventional resin composites in direct restorations of posterior teeth was similar, within a follow-up period of 12 to 72 months. However, randomized clinical trials with longer follow-up periods are still necessary.
References
Van Dijken JWV, Pallesen U (2013) A six-year prospective randomized study of a nano-hybrid and a conventional hybrid resin composite in class II restorations. Dent Mater 29:191–198. https://doi.org/10.1016/j.dental.2012.08.013
de Andrade A, Duarte R, FM e S et al (2014) Resin composite class I restorations: a 54-month randomized clinical trial. Oper Dent 39:588–594. https://doi.org/10.2341/14-067-C
Ástvaldsdóttir Á, Dagerhamn J, Van Dijken JWV et al (2015) Longevity of posterior resin composite restorations in adults—a systematic review. J Dent 43:934–954. https://doi.org/10.1016/j.jdent.2015.05.001
Schmidt M, Dige I, Kirkevang LL, Vaeth M, Hørsted-Bindslev P (2015) Five-year evaluation of a low-shrinkage Silorane resin composite material: a randomized clinical trial. Clin Oral Investig 19:245–251. https://doi.org/10.1007/s00784-014-1238-x
Opdam NJM, van de Sande FH, Bronkhorst E, Cenci MS, Bottenberg P, Pallesen U, Gaengler P, Lindberg A, Huysmans MCDNJM, van Dijken JW (2014) Longevity of posterior composite restorations: a systematic review and meta-analysis. J Dent Res 93:943–949. https://doi.org/10.1177/0022034514544217
Lynch CD, Opdam NJ, Hickel R, Brunton PA, Gurgan S, Kakaboura A, Shearer AC, Vanherle G, Wilson NH, Academy of Operative Dentistry European Section (2014) Guidance on posterior resin composites: Academy of Operative Dentistry—European section. J Dent 42:377–383. https://doi.org/10.1016/j.jdent.2014.01.009
Ferracane JL (2011) Resin composite—state of the art. Dent Mater 27:29–38. https://doi.org/10.1016/j.dental.2010.10.020
Fronza BM, Rueggeberg FA, Braga RR, Mogilevych B, Soares LES, Martin AA, Ambrosano G, Giannini M (2015) Monomer conversion, microhardness, internal marginal adaptation, and shrinkage stress of bulk-fill resin composites. Dent Mater 31:1542–1551. https://doi.org/10.1016/j.dental.2015.10.001
Kim RJY, Kim YJ, Choi NS, Lee IB (2015) Polymerization shrinkage, modulus, and shrinkage stress related to tooth-restoration interfacial debonding in bulk-fill composites. J Dent 43:430–439. https://doi.org/10.1016/j.jdent.2015.02.002
Sajnani A, Hegde M (2016) Leaching of monomers from bulk-fill composites: an in vitro study. J Conserv Dent 19:482–486. https://doi.org/10.4103/0972-0707.190020
Alrahlah A, Silikas N, Watts DC (2014) Post-cure depth of cure of bulk fill dental resin-composites. Dent Mater 30:149–154. https://doi.org/10.1016/j.dental.2013.10.011
Lopes GC, Baratieri LN, Monteiro S, Vieira LCC (2004) Effect of posterior resin composite placement technique on the resin–dentin interface formed in vivo. Quintessence Int 35:156–161
Flury S, Hayoz S, Peutzfeldt A, Hüsler J, Lussi A (2012) Depth of cure of resin composites: is the ISO 4049 method suitable for bulk fill materials? Dent Mater 28:521–528. https://doi.org/10.1016/j.dental.2012.02.002
Flury S, Peutzfeldt A, Lussi A (2014) Influence of increment thickness on microhardness and dentin bond strength of bulk fill resin composites. Dent Mater 30:1104–1112. https://doi.org/10.1016/j.dental.2014.07.001
Czasch P, Ilie N (2013) In vitro comparison of mechanical properties and degree of cure of bulk fill composites. Clin Oral Investig 17:227–235. https://doi.org/10.1007/s00784-012-0702-8
El-Safty S, Akhtar R, Silikas N, Watts DC (2012) Nanomechanical properties of dental resin-composites. Dent Mater 28:1292–1300. https://doi.org/10.1016/j.dental.2012.09.007
Van Ende A, De Munck J, Lise DP, Van Meerbeek B (2017) Bulk-fill composites: a review of the current literature. J Adhes Dent 19:95–110. https://doi.org/10.3290/j.jad.a38141
Alshali RZ, Silikas N, Satterthwaite JD (2013) Degree of conversion of bulk-fill compared to conventional resin-composites at two time intervals. Dent Mater 29:e213–e217. https://doi.org/10.1016/j.dental.2013.05.011
Didem A, Gözde Y, Nurhan Ö (2014) Comparative mechanical properties of bulk-fill resins. Open. J Compos Mater 4:117–121. https://doi.org/10.4236/ojcm.2014.42013
Miletic V, Peric D, Milosevic M, Manojlovic D, Mitrovic N (2016) Local deformation fields and marginal integrity of sculptable bulk-fill, low-shrinkage and conventional composites. Dent Mater 32:1441–1451. https://doi.org/10.1016/j.dental.2016.09.011
Higgins JPTGS (2009) Cochrane handbook for systematic reviews of interventions version 5.0.2 [updated September 2009]. In: Cochrane Collab available from www.cochrane--www.handbook.org
Moher D, Shamseer L, Clarke M et al (2015) Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev 4(1). https://doi.org/10.1186/2046-4053-4-1
Lemos CAA, Verri FR, Bonfante EA, et al (2017) Comparison of external and internal implant-abutment connections for implant supported prostheses. A systematic review and meta-analysis. J Dent 70: 14–22. https://doi.org/10.1016/j.jdent.2017.12.001
Atieh MA, Alsabeeha NH, Payne AG, et al (2015) Interventions for replacing missing teeth: alveolar ridge preservation techniques for dental implant site development. In: Cochrane Database Syst. Rev. p CD010176
Moraschini V, da Costa LS, dos Santos GO (2018) Effectiveness for dentin hypersensitivity treatment of non-carious cervical lesions: a meta-analysis. Clin Oral Investig 22:617–631. https://doi.org/10.1007/s00784-017-2330-9
Wilson MA, Cowan AJ, Randall RC, Crisp RJ, Wilson NH (2002) A practice-based, randomized, controlled clinical trial of a new resin composite restorative: one-year results. Oper Dent 27(5):423-429
Bayraktar Y, Ercan E, Hamidi MM, Çolak H (2017) One-year clinical evaluation of different types of bulk-fill composites. J Investig Clin Dent 8. https://doi.org/10.1111/jicd.12210
van Dijken JWV, Pallesen U (2016) Posterior bulk-filled resin composite restorations: a 5-year randomized controlled clinical study. J Dent 51:29-35. https://doi.org/10.1016/j.jdent.2016.05.008
van Dijken JWV, Pallesen U (2017) Bulk-filled posterior resin restorations based on stress-decreasing resin technology: a randomized, controlled 6-year evaluation. Eur J Oral Sci 125:303–309. https://doi.org/10.1111/eos.12351
Manhart J, Chen H-Y, Hickel R (2010) Clinical evaluation of the posterior composite Quixfil in class I and II cavities: 4-year follow-up of a randomized controlled trial. J Adhes Dent 12:237–243. https://doi.org/10.3290/j.jad.a17551
Karaman E, Keskin B, Inan U (2017) Three-year clinical evaluation of class II posterior composite restorations placed with different techniques and flowable composite linings in endodontically treated teeth. Clin Oral Investig 21:709–716. https://doi.org/10.1007/s00784-016-1940-y
Arhun N, Celik C, Yamanel K (2010) Clinical evaluation of resin-based composites in posterior restorations: two-year results. Oper Dent 35:387–404. https://doi.org/10.2341/09-345-C
Çolak H, Tokay U, Uzgur R et al (2017) A prospective, randomized, double-blind clinical trial of one nano-hybrid and one high-viscosity bulk-fill composite restorative systems in class II cavities: 12 months results. Niger J Clin Pract 20:822–831. https://doi.org/10.4103/1119-3077.212449
Atabek D, Aktaş N, Sakaryali D, Bani M (2017) Two-year clinical performance of sonic-resin placement system in posterior restorations. Quintessence Int 48:743–751. https://doi.org/10.3290/j.qi.a38855
Alkurdi RM, Abboud SA (2016) Clinical evaluation of class II composite: resin restorations placed by two different bulk-fill techniques. J Orofac Sci 8:34–39. https://doi.org/10.4103/0975-8844.181926
Yazici A, Antonson S, Kutuk Z, et al (2017) Thirty-six-month clinical comparison of bulk fill and nanofill composite restorations. Oper Dent. https://doi.org/10.2341/16-220-C
Egger M, Smith GD (2017) Principles of and procedures for systematic reviews. In: Egger M, Smith GD, Douglas GA (Eds.), Systematic Reviews in Health Care. Evidence-Based Health Care, 23–42
Hickey D, Sharif O, Janjua F, Brunton PA (2016) Bulk dentine replacement versus incrementally placed resin composite: a randomised controlled clinical trial. J Dent 46:18-22. https://doi.org/10.1016/j.jdent.2016.01.011
Manhart J, Med Dent P-D, Chen H-Y, Dent M (2008) Clinical performance of the posterior composite QuiXfil after 3, 6, and 18 months in class 1 and 2 cavities. Quintessence Int 3939:757–765
Manhart J, Chen HY, Hickel R (2009) Three-year results of a randomized controlled clinical trial of the posterior composite QuiXfil in class I and II cavities. Clin Oral Investig 13:301–307. https://doi.org/10.1007/s00784-008-0233-5
Van Dijken JWV, Pallesen U (2015) Randomized 3-year clinical evaluation of class I and II posterior resin restorations placed with a bulk-fill resin composite and a one-step self-etching adhesive. https://doi.org/10.3290/j.jad.a33502
Van Dijken JWV, Pallesen U (2014) A randomized controlled three year evaluation of bulk-filled posterior resin restorations based on stress decreasing resin technology. Dent Mater 30:e245–e251. https://doi.org/10.1016/j.dental.2014.05.028
Landis JR, Koch GG (1977) The measurement of observer agreement for categorical data. Biometrics 33:159–174. https://doi.org/10.2307/2529310
Monterubbianesi R, Orsini G, Tosi G, Conti C, Librando V, Procaccini M, Putignano A (2016) Spectroscopic and mechanical properties of a new generation of bulk fill composites. Front Physiol 7. https://doi.org/10.3389/fphys.2016.00652
Ibarra ET, Lien W, Casey J et al (2015) Physical properties of a new sonically placed composite resin restorative material. Gen Dent 63:51–56
Li X, Pongprueksa P, Van Meerbeek B, De Munck J (2015) Curing profile of bulk-fill resin-based composites. J Dent. https://doi.org/10.1016/j.jdent.2015.01.002
El-Damanhoury H, Platt J (2014) Polymerization shrinkage stress kinetics and related properties of bulk-fill resin composites. Oper Dent. https://doi.org/10.2341/13-017-L
Nedeljkovic I, Teughels W, De Munck J et al (2015) Is secondary caries with composites a material-based problem? Dent Mater 31:e247–e277. https://doi.org/10.1016/j.dental.2015.09.001
Sarrett DC (2005) Clinical challenges and the relevance of materials testing for posterior composite restorations. Dent Mater pp 21:9–20
Wang Y, Li C, Yuan H, Wong MCM, Zou J, Shi Z, Zhou X, Cochrane Oral Health Group (2016) Rubber dam isolation for restorative treatment in dental patients. Cochrane Database Syst Rev. https://doi.org/10.1002/14651858.CD009858.pub2
Unemori M, Matsuya Y, Akashi A, Goto Y, Akamine A (2001) Composite resin restoration and postoperative sensitivity: clinical follow-up in an undergraduate program. J Dent 29:7–13. https://doi.org/10.1016/S0300-5712(00)00037-3
Costa T, Rezende M, Sakamoto A, et al (2017) Influence of adhesive type and placement technique on postoperative sensitivity in posterior composite restorations. Oper Dent. https://doi.org/10.2341/16-010-C
Reis A, Dourado Loguercio A, Schroeder M, Luque-Martinez I, Masterson D, Cople Maia L (2015) Does the adhesive strategy influence the post-operative sensitivity in adult patients with posterior resin composite restorations? A systematic review and meta-analysis. Dent Mater 31:1052–1067. https://doi.org/10.1016/j.dental.2015.06.001
Schenkel AB, Peltz I, Veitz-Keenan A (2016) Dental cavity liners for class I and class II resin-based composite restorations. Cochrane Database Syst Rev. https://doi.org/10.1002/14651858.CD010526.pub2
Göstemeyer G, Blunck U, Paris S, Schwendicke F (2016) Design and validity of randomized controlled dental restorative trials. Materials (Basel) 9. https://doi.org/10.3390/ma9050372
Opdam NJM, Collares K, Hickel R, Bayne SC, Loomans BA, Cenci MS, Lynch CD, Correa MB, Demarco F, Schwendicke F, Wilson NHF (2018) Clinical studies in restorative dentistry: new directions and new demands. Dent Mater 34:1–12. https://doi.org/10.1016/j.dental.2017.08.187
Reis A, Loguercio AD, Maran BM et al (2017) Randomized clinical trials in bleaching: compliance with the consort statement. Braz Oral Res 33:e67–e67
Schulz KF, Altman DG, Moher D, Consort Group (2010) CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials (Chinese version). J Chinese Integr Med 8:604–612. https://doi.org/10.3736/jcim20100702
Acknowledgements
The authors would like to thank CAPES (Coordination for the Improvement of Higher Education Personnel) for their financial support.
Funding
The work was supported by the CAPES (Coordination for the Improvement of Higher Education Personnel).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
For this type of study, formal consent is not required.
Rights and permissions
About this article

Cite this article
Veloso, S.R.M., Lemos, C.A.A., de Moraes, S.L.D. et al. Clinical performance of bulk-fill and conventional resin composite restorations in posterior teeth: a systematic review and meta-analysis. Clin Oral Invest 23, 221–233 (2019). https://doi.org/10.1007/s00784-018-2429-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-018-2429-7