
Abstract
Objective
This study compared the effects of mold material and diameter on the thickness of cured composite remnants and depth of cure (DOC) of resin-based composites (RBC).
Material and methods
One Polywave® curing light was used to photo-cure two shades of the same “bulk-fill” RBC in 4, 6, or 10-mm internal diameter metal or white Delrin® molds. For 60 specimens, the uncured RBC was manually scraped away as described in the ISO 4049 depth of cure test. The remaining 60 specimens were immersed in tetrahydrofuran for 48 hours in the dark. Maximum lengths of remaining hard RBC and their DOC values were compared using analysis of variance (ANOVA) and Tukey–Kramer post hoc multiple comparison tests (α = 0.05).
Results
Specimen thickness and DOC were always greater using the white Delrin® molds compared to metal molds (p < 0.001). Increase in mold diameter significantly increased specimen thickness and DOC when made in the metal molds and in the 6-mm diameter Delrin® molds (p < 0.01). Increasing the diameter of the Delrin® molds to 10-mm did not increase specimen thickness or DOC. Sectioning and staining of specimens revealed an internal, peripheral transition zone of porous RBC in the solvent-dissolved specimens only.
Conclusion
Mold material and internal diameter significantly influenced cured composite remnant thickness as well as depth of cure. The existence of an outer region of RBC that is hard, yet susceptible to solvent dissolution, requires further investigation.
Clinical relevance
The depth of cure results obtained from a 4-mm diameter metal mold may not represent the true potential for evaluating composite depth of cure. A universally acceptable mold material and diameter size need to be established if this type of testing is to be useful for evaluating the relative performance of a given type of LCU and RBC.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
More than 260 million direct resin-based composite (RBC) restorations were placed worldwide in 2011. Currently, almost no amalgam restorations are placed in Scandinavian countries [1]. Instead, photo-polymerizable RBCs have become the material of choice for direct restorations. With the global phase down in amalgam use, the use of RBCs will only increase [2, 3]. In response to the increased use of RBCs, several developments have made the process of light curing RBCs more efficient and thus have shortened chairside procedures. However, there also exists indirect evidence that under-curing RBC restorations is undesirable and may result in more bulk fractures, increased restoration wear, increased release of leachates, and more microleakage [4–9]. A clinical study placed RBC restorations in denture teeth. The results showed increased wear when the RBC received inadequate light exposure [6]. Thus, a simple and clinically relevant test that measures the outcome of light curing the RBC is needed so the dentist can know what is required to adequately polymerize an entire RBC restoration.
Tests measuring resin polymerization
Fourier transform mid-infrared spectroscopy as well as Raman spectroscopic techniques are used to measure the degree of conversion of dental resins at different depths or thicknesses [10–14]. Alternatively, surface microhardness is a reliable method to determine material properties of the cured RBC [15], and a strong, positive correlation exists between changes in the degree of monomer conversion and the microhardness value of the same RBC [9, 16–18]. However, these tests require sophisticated equipment. Also, usually such testing does not test the entire specimen, but instead only measures a small region within the center of the RBC specimen.
Tests measuring depth of cure
In contrast, the ISO 4049 depth of cure (DOC) test is simple and quick to conduct. The test uses a stainless steel mold with a hole 4-mm in diameter filled with RBC [19]. Immediately after light exposure, the resin specimen is removed, and any uncured material is manually scraped away using a plastic spatula. The maximum length of the remaining cylinder of hard, cured material is measured and divided by two. This value is then reported as the depth of cure for that given LCU and RBC combination [19]. This specific testing makes no claims of correlating results with clinical performance of the LCU/RBC tested, but instead, is designed to provide a relative performance, among which, other lights and composites can be ranked. The DOC values, however, are used to provide a framework by which acceptable limits of the in vitro performance of LCUs and composites are stated.
Although the ISO 4049 test is fast and easy to administer, it has limitations. Depending on the operator technique, the stiffness or sharpness of the spatula, and the consistency of RBC, manual removal of uncured RBC using a plastic instrument can be subjective. Consequently, the DOC value may be either over or under-estimated [20]. This limitation is somewhat compensated for by dividing the value of the length of scrape-resistant RBC by a factor of two. Despite this adjustment, the ISO 4049 method may still overestimate the DOC [20, 21]. In addition, both the diameter [22] and type of mold material have been shown to affect the results [18, 23].
Relevance of a 4-mm-diameter metal mold to test DOC of bulk-fill RBCs
Bulk-fill RBCs are designed to fill an entire preparation to a depth of 4 to 5-mm and then to be light-cured in a single increment. With the dimensions of a mandibular molar being approximately 11.0-mm mesio-distally and 10.5-mm bucco-lingually at the crown, and 9.0-mm by 9.0-mm at the cervix [24], light-curing a 4-mm diameter cylinder of RBC in a metal mold to determine the DOC provides little information about the ability of the LCU to simultaneously polymerize the mesial and distal boxes of a bulk-filled mesial-occlusal-distal (MOD) restoration in a molar tooth. Instead, a larger diameter mold should be used for such a simulation. In addition, the ISO 4049 test assumes that the LCU delivers light that is uniformly distributed across the entire tip area, and that the position of the light tip over the RBC will not affect the results. It is now well established that the irradiance and the distribution of the spectral emission from dental LCUs can be very inhomogeneous [25–31] and that the shorter wavelengths do not penetrate as deeply into the RBC compared to longer wavelengths of light [32, 33]. Thus, if a 4-mm-diameter mold is positioned under an irradiance “hot or cold spot” (area of high or low local irradiance and/or with an inhomogeneous spectral distribution from the LCU), results may be generated that do not represent the DOC that may be achieved if the RBC is positioned under other regions of the light tip [29, 34].
Alternative methods to remove uncured resin
In industry, uncured resins are commonly removed using a solvent [35]. Removing uncured dental resin in a reproducible manner using a solvent would be advantageous, and both ethanol and acetone have been used [20, 36, 37]. Such testing would not rely upon the subjective judgment or inconsistent performance of the operator. However, direct comparisons between results obtained using the current ISO 4049 manual scraping test method and those obtained after using a solvent to remove uncured RBC have yet to be published.
The purpose of this study was to compare the effect of three different mold diameters and two different mold materials on the depth of cure of two RBCs. Additionally, the effects of using an organic solvent [tetrahydrofuran, (THF)] to remove the uncured RBC using a “no-touch” technique compared to using the manual scraping method as described in ISO 4049 were examined. The hypotheses tested were that:
-
1.
mold material will have no significant effect on the thickness or depth of cure of remaining RBC,
-
2.
mold diameter will have no significant effect on the thickness or depth of cure of remaining RBC, and
-
3.
the use of a solvent to remove uncured RBC will reveal an outer zone of hard, yet porous, RBC that will not be present in the same locations of specimens where uncured composite was manually scraped away, and never exposed to solvent treatment.
Materials and methods
LCU radiant power and beam profile
A mains-powered, Polywave® LCU (Bluephase Style serial # 1100012791, Ivoclar Vivadent, Amherst, NY, USA) with the 10-mm-diameter light guide that includes a light homogenizer (Ref #636240, Ivoclar Vivadent) was used. The total radiant power was recorded five times using a 6-inch integrating sphere (Labsphere, North Sutton, NH, USA) connected to a fiberoptic spectrometer (USB 4000, Ocean Optics, Dunedin, FL, USA). The system had been calibrated using a National Institute of Standards and Technology (Gaithersburg, MD, USA) traceable light source (Labsphere) prior to the start of the experiment. To demonstrate the relative spectral attenuation of wavelengths of light emitted by the LCU through different thicknesses of cured composite, the spectral radiant powers transmitted into the spectrometer through 12-mm diameter disks of cured RBC that were 0.5-, 1.0-, 2.0-, 3.0-, and 4.0-mm-thick, were measured. The LCU tip was placed in contact with the top surface of the RBC, and the bottom surface was flush with the entrance to the integrating sphere.
To examine the inhomogeneity of the light output at the light tip, the spectral radiant power was recorded five times through a 4-mm-diameter aperture into the integrating sphere. The LCU was first centered over the 4-mm aperture, and the spectral radiant power was recorded. The LCU was then moved up 2-mm and the output through the 4-mm aperture recorded, then down 2-mm from the center, then 2-mm to the right from the center, and finally 2-mm to the left from the center. The irradiance distribution across the light guide tip end was characterized using a previously described laser beam profiler technique [28, 38] to produce a color-scaled image of the irradiance distribution across the end of the light guide. This laser beam profiling technique used a camera with a 50-mm focal length lens (USB-L070, Ophir-Spiricon, Logan, UT, USA). The image was taken with the tip of the light guide just out of contact with a translucent, ground glass target (DG2X2-1500, Thor Laboratories, Newton, NJ, USA).
Depth of cure of RBCs
Two shades of the same bulk-fill RBC (Tetric Evoceram Bulk Fill, shades IVA and IVW, Ivoclar Vivadent, Schaan, Liechtenstein) were used. These resins are intended to fill posterior restorations and be photocured in a single-layer up to 4-mm thick [37]. The uncured RBC was packed into split molds that had either a 4-, 6-, or 10-mm internal diameter openings, over a white filter paper background [19]. The molds with the 10-mm diameter openings represented the average mesial-distal width of a molar tooth [24] and matched the outer diameter of the 10-mm wide light guide tip. Metal stainless steel molds were 10-mm deep, and the white Delrin® molds were 15-mm deep, to account for the greater depth of cure in the Delrin® molds. A polyester strip was placed over each surface of the RBC before it was exposed to the LCU for 10 s [37], with the tip end positioned concentrically to the mold opening and directly against the polyester surface. Throughout the study, the LCU was clamped rigidly in place, and all specimens were made at room temperature (~22 °C) using the same LCU/light tip and RBC orientation.
A total of 120 specimens were made (2 mold materials × 3 diameters × 2 RBCs × 10 replications). Immediately after exposure, the polyester strips were removed, the molds were opened, and the RBC was removed. Five specimens from each group were treated according to the ISO 4049 test method, and the uncured RBC was manually scraped away using a plastic spatula. The maximum length of the remaining hard, cured resin was measured to the nearest 0.1 mm using digital calipers (Mitutoyo Canada Inc., Mississauga, ON, Canada). For the other five specimens, the soft uncured RBC was not removed. Instead, the entire specimen was immersed immediately in an organic solvent (tetrahydrofuran, Sigma Aldrich, St. Louis, MO, USA) and dark-stored for 48 h at 22 °C. Upon removal from the solvent, the RBC specimens were allowed to air-dry, and the maximum length of remaining resin was measured using digital calipers. Standardized digital photographs were taken of the specimens before and after immersion in the solvent. In addition, all the 10-mm diameter specimens were sectioned longitudinally, from top-to-bottom, and placed in a stain (toluidine blue) to illustrate the presence of any porous, yet hard RBC material.
Statistics
A four-factor analysis of variance (ANOVA) showed that the length of cured RBC remnant was affected by both mold type and diameter of the mold. Therefore, the main effects of interest were examined separately for each combination, namely the effects RBC shade and the method of uncured resin removal were examined using a two-factor ANOVA at a pre-set alpha value of 0.05. This analysis was followed by a Tukey–Kramer multiple comparison procedure to test for significant pair-wise differences between mean values.
Results
Radiant power and beam profile
The radiant power from the LCU measured 670 mW. This value was used to provide the scaled irradiance beam profile image seen in Fig. 1. The manufacturer stated the tip diameter to be 10-mm, but the active, light-emitting area measured 9.0-mm. This discrepancy produced a 0.5-mm wide zone of RBC between the active LCU tip diameter and the 10-mm mold that was not directly irradiated. When moving the 4-mm-diameter mold aperture across the emitting end of the LCU, the ratios of the two emission peaks (409 and 456-nm) changed, depending on which region of the LCU tip was measured (Fig. 2). Depending on which 4-mm diameter region across the light guide was measured, the radiant powers measured through the apertures ranged from 119 to 160 mW, and irradiance values ranged from 950 to 1270 mW/cm2. Figure 3 illustrates the effect of this output inhomogeneity on the resin polymerization in the 10-mm diameter mold.

View of the light-emitting end of the Bluephase Style with a 9-mm internal diameter light guide. Outlines of the LED locations within the un-activated LCU are evident (a). Inhomogeneity in the tip exitance irradiance is illustrated in the beam profile image (b) using color-coded irradiance (mW/cm2) values (red = high, and violet = low irradiance). The circles in (b) indicate the diameters of the 4, 6, and 10-mm molds

View of the light-emitting end of the Bluephase Style light guide with outlines of the 4-mm aperture opening representing the restriction of light into the ISO 4049 mold dimension is superimposed over the light guide. Inhomogeneity in emission wavelengths can be observed together with inhomogeneity in the tip exitance irradiance (red = high, and violet = low irradiance values). It can be seen that the spectral radiant powers are different across the light-emitting tip

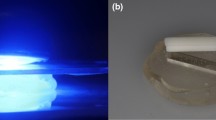
Views of the recovered cured remnants of 10-mm diameter RBC specimens made in the metal mold and subjected to either manual scraping using a plastic spatula (left), or retrieved after solvent dissolution (right). Note the asymmetrical, slanted bottom surfaces of both the scraped and dissolved specimens under the 409-nm emitting LED. Only the specimens subjected to solvent dissolution followed by sectioning and staining produced a region of porous stained RBC that was 0.5- to 2.0-mm thick at the sides and of the RBC (bottom right)
Remaining cured composite remnant thickness and depth of cure
Depending on the test condition, after 10 s of light exposure, the mean length of remaining hard RBC ranged from 5.90 to 12.00-mm. When this thickness was divided in half (in accordance with ISO 4049), the resulting depth of cure values fell between 2.95 and 6.00-mm, depending on the mold diameter used. Table 1 shows the groups where significant differences occurred when comparing the effects of all four factors on the depth of cure (Tukey–Kramer multiple comparison test). When the main effects of interest, namely the effects of RBC shade and the method of uncured resin removal, were examined separately for each combination using two-factor ANOVA, each of these factors presented no interactions. The effect of how the uncured RBC was removed on the remaining length of RBC was influenced by the type and diameter of the mold material used. An increase in mold diameter significantly increased the length of cured RBC when using the metal molds and between the 4 and 6-mm diameter Delrin® molds (p < 0.01). Figure 4 illustrates the effect of the two mold materials and the three mold diameters on the length of remaining RBC. The significant interaction effect of the mold type (p < 0.01), is illustrated in Fig. 4 where the mean length of the remaining RBC was less in the 10-mm diameter Delrin® mold, compared to the 4- and 6-mm diameter Delrin® mold. This effect was not observed when using the metal mold.

Maximum remaining length of retrieved, hard RBC (Tetric Bulk Fill shade IVA or shade IVW), according to method of removal of uncured RBC (S manually scraped, D solvent-dissolved), mold type (metal or Delrin®), and diameter (4, 6, or 10-mm). N = 5 specimens per condition, vertical bar = ±1 standard deviation
Bottom surface topography
Figures 1 and 2 illustrate the marked differences in the spectral radiant powers and irradiance distributions delivered to the top surface of the molds. Figure 3 illustrates the unsymmetrical bottom surface profile of the hard-cured RBC and the absorption patterns of the toluidine blue stain into the porous regions of transected RBC specimens seen when using the 10-mm diameter metal mold. In all specimens, the length of hard RBC positioned directly underneath the violet-emitting LED chip (emitting a peak spectral output at 409-nm) was not as long as the remaining resin exposed directly under the locations where the two blue-emitting LEDs (emitting peak spectral output at 456-nm) were located. Figure 5 illustrates the decline in the transmitted spectral radiant power through 12-mm diameter disks of cured RBC. For both shades of RBC, almost no light from the 409-nm LED chip was emitted from the bottom of the 4.0-mm thick specimens of both RBC shades.

Decline in spectral radiant power (mW/nm) through disks of cured RBC that were 0.5, 1.0, 2.0, 3.0, and 4.0-mm thick. Note that almost no light from the violet (409-nm LED) chip was emitted from the bottom of the 4.0-mm thick specimens
Discussion
The purpose of this study was to compare the thickness values of remaining RBC when using two mold materials and three mold diameters. Additionally, the effects of using an organic solvent to remove the uncured RBC were examined. For the two RBCs tested, Fig. 4 reports that the remaining cured composite specimen lengths and DOC values were always greater when using the white Delrin® molds, when compared to values seen using metal molds (p < 0.001). Thus, the first research hypothesis was accepted. Increase in mold diameter significantly increased the length of hard composite and DOC values when made using metal molds and for the Delrin® 6-mm diameter molds compared to the 4-mm diameter Delrin® molds (p < 0.01), but not for the 10-mm diameter Delrin® molds. A similar increase in hardness at the center of RBC specimens has been reported when using 10-mm diameter metal molds compared to 4-mm diameter metal molds [22]. However, for both the 4- and the 6-mm diameter Delrin® molds, an increase in mold diameter to 10-mm did not increase cured composite specimen length. Thus, the second hypothesis that mold diameter would have no effect on cured composite specimen length or DOC was rejected.
As shown in Fig. 4, depending on the mold diameter, the lengths of hard RBC remnants ranged from 5.9 to 8.4-mm in the metal molds and were 8.7 to 12.0-mm long in the white Delrin® molds. Table 1 shows that when divided by two, all the depth of cure values achieved using the Delrin® molds were greater than the 4-mm maximum increment thickness recommended by the RBC manufacturer. Similar increases in the depth of cure using white molds have been previously reported [18, 23]. Use of semi-transparent white Delrin® molds may more accurately represent what occurs in the tooth, compared to when using the completely opaque metal molds. However, once again, the ISO specification is not designed to correlate with any clinical situation.
A previous study using a halogen curing light also reported that the distribution of resin curing in opaque molds was substantially lower at or near the mold walls than at the center, and the depth of cure was dependent on the diameter of the mold [18]. Similarly, the curing pattern observed in the present study was substantially lower near the metal mold walls than at the center, but this effect was not symmetrical. In the 4- and 6-mm-diameter Delrin® molds, the curing pattern produced longer lengths of cured composite near the Delrin® mold walls than at the center for the specimens, but this was not observed in the specimens made using the 10-mm diameter Delrin® molds.
This study used the Bluephase Style with the new light homogenizer tip. Figures 1, 2, and 3 illustrate that the irradiance and emission spectrum “hot spots” associated with the physical locations of the three individual LED chips within the LCU head are less prominent than from previous version of this LCU [28, 34]. However, one “hot spot” can still be attributed to the 409-nm violet-emitting LED chip, and the other two high irradiance areas are correlated with the two 456-nm blue-emitting LED chips. Figure 3 shows that the RBC directly underneath the shorter wavelength, violet chip was cured to a shallower depth and even broke away when subjected to a small load after solvent dissolution. The use of a light tip that was smaller in diameter than the mold minimized any effect of light passing through the semi-transparent mold material, or any interaction between the RBC and the side of the mold [23]. The fiber-to-fiber LCU tip diameter was 9-mm and the diameter of the molds used in Fig. 5 was 12-mm. This provided a 1.5-mm thickness of RBC between the light beam and the walls of the mold. Figure 5 illustrates that for both shades of RBC, although some of the lower wavelengths were transmitted through 3.0-mm of RBC, almost no emission from the 409-nm violet LED chip was detected at the bottom of the 4.0-mm thick samples of either RBC shade and only low irradiance from the 456-nm chip was present in this region. This result confirms previous reports describing the reduced transmission of the shorter wavelengths of light [32, 33] and accounts for the reduced depth of cure below the violet-emitting LED chip that can be seen in Fig. 3.
As seen in Figs. 3 and 5, not all areas of the specimen received the same irradiance and wavelengths of light from the LCU, and both methods of removing the uncured RBC confirmed the presence of uneven curing across the bottom surface of the RBC. This uneven resin polymerization demonstrates that a mold that is wider in diameter than 4-mm is required to demonstrate the effects of beam inhomogeneity on depth of cure. Also instead of only measuring the maximum length of hard RBC remaining, it is necessary to take a cross-section view and report the shape of the hard RBC remaining at the bottom. Only then is it possible to determine if there are any positive or negative effects of light output inhomogeneity on RBC that is intended to fill an entire molar MOD preparation and be adequately cured in a single light exposure. The result shown in Fig. 3 is contrary to the results of a study by Li et al. [14] who reported that beam inhomogeneity (regarding the position of the 410-nm versus that of 470-nm LEDs) did not significantly affect the results for all five RBCs they tested. However, these authors used the LCU on the high-power setting for double the recommended exposure time and failed to measure the beam profile from the Polywave® Bluephase 20i (Ivoclar Vivadent) LCU used in the study. Thus, the reader is unsure whether the light output from the Bluephase 20i was indeed inhomogeneous. In the future, studies should either report the beam profile or refer to a source such as a publication or a manufacturer’s website where the beam profile information is available.
Figure 4 illustrates that the choice of mold diameter significantly affected the maximum length of remaining cured composite. Despite the large volume increase in the total amount of material used in the 10-mm diameter mold compared to the 4-mm diameter ones (from 125.73 to 785.4 mm3) when the RBCs were exposed using the same 10-s time, the thickness of remaining cured composite remnant increased as the mold diameter increased from 4 to 10-mm. This increase is likely attributed to the fact that the 10-mm diameter mold received the entire light output from the LCU, whereas the 4-mm diameter mold only received a small, localized sample of light (wavelengths and irradiance) from the LCU. Although the 6-mm mold was still smaller than the diameter of the light guide, Fig. 1 shows that it was wide enough to capture regions of high irradiance from the LCU. In addition, because the Delrin® mold itself transmitted light, RBCs in the 4 and 6-mm diameter molds received light from the top and laterally down the sides of the specimen. This resulted in longer lengths of hard RBC in the 4- and 6-mm diameter Delrin® molds. This situation could not occur in the opaque metal mold and only partially occurred in the 10-mm Delrin® mold. Figure 1 shows that the 10-mm-diameter Delrin® mold was wider than the 9-mm active tip diameter of the LCU. Thus, not as much additional light could reach the Delrin® in the 10-mm mold and then be transmitted down the mold to reach the sides of the RBC. This difference resulted in shallower depths of cured composite remnants and shorter RBC specimens in the 10-mm Delrin® molds, compared to specimens made using the 4 and the 6-mm diameter Delrin® molds.
While the ISO 4049 test using a 4-mm diameter mold is a simple screening method, it is prone to operator-induced variables and only measures the maximum length of remaining hard RBC. The resulting depth of cure values are thus highly dependent upon this maximum length measurement. Examining the shape of the remaining hard RBC at the bottom of a 10-mm diameter mold may offer more clinically relevant results, especially for bulk-filling RBCs. Although the external profiles of remaining hard RBC appeared similar using the two methods, solvent-dissolved specimens revealed an internal transition zone of porous RBC that was not present in specimens where uncured composite was removed using manual scraping. This porous region and its shape confirm that it is not the maximum length of hard RBC remaining that should be reported as the DOC, but instead some adjustment is required.
The alternative, “no-touch,” solvent-dissolution method to remove uncured RBC was easy to implement. When sectioned, the information from the solvent-dissolved specimens revealed a distinct, internal border between the shiny, apparently well-cured RBC and the peripheral, porous solvent-resistant polymer. This porous, “frosty” region was approximately 1.5 to 2.0-mm thick across the bottom surface, furthest away from the light and followed the profile of the outer hard bottom surface of the RBC (Fig. 3). This region has been previously described as “frosty” [37], and its width appears visually similar to the 2.2-mm difference previously observed between the length of hard RBC after the soft material had been scraped away and the region where differences in the RBC properties have been reported to begin [36]. Additionally, a larger mold size should be used when testing bulk-fill RBCs to examine how well an entire restoration may be polymerized. The porous region that was evident only after placing the RBCs in solvent indicated that the depth of cure of both RBCs was less than 4-mm at the periphery when a 9-mm-diameter light tip was used. This region in the 10-mm diameter mold corresponded to the mesial and distal proximal boxes of a 10-mm-diameter molar MOD restoration where the RBC is furthest away from the light source and where most restoration failures occur. Although a porous inner region was also present in the 4- and 6-mm-diameter specimens, because the 4- and 6-mm molds produced longer specimens, the length of unstained RBC at the edges was longer than 4-mm. Thus, the third hypothesis, that solvent dissolution would reveal additional information about the RBC remnant, was accepted.
A limitation of this study was that it tested only two bulk-fill RBCs from the same manufacturer and did not test the properties of the RBC or the effects of longer exposure times on the DOC. Ongoing microhardness tests and degree of conversion analyses are attempting to identify the nature of polymer along the transition zone at the bottom of the solvent-dissolved RBCs. Future studies will focus on specific guidelines for identifying the “ideal solvent,” the optimal duration of solvent exposure, the best stain to be used, and the preferred type and mold size.
Conclusions
Within the limitations of this study, it may be concluded that the mold material and mold diameter play an important role in determining the depth of cure of RBCs:
-
1.
Specimen thickness was always greater in white Delrin® molds when compared to metal molds (p < 0.001).
-
2.
Increase in mold diameter significantly increased cured composite specimen thickess and the depth of cure when made in the metal molds, and between the 4 and 6-mm diameter Delrin® molds (p < 0.01). However, when compared to the 4 and the 6-mm diameter Delrin® molds, increasing mold diameter to 10-mm did not result in a greater specimen thickness or a greater depth of cure.
-
3.
Remaining RBC thickness beneath the violet LED chip (peak emission 409-nm) was shorter than areas directly under the blue (peak emission 456-nm) LEDs.
-
4.
Solvent-dissolved specimens revealed an internal transition zone of porous and less well-cured RBC that was not present in specimens where soft composite was scraped away.
References
Heintze SD, Rousson V (2012) Clinical effectiveness of direct class II restorations - a meta-analysis. J Adhes Dent 14(5):407–431. doi:10.3290/j.jad.a28390
Lynch CD, Wilson NH (2013) Managing the phase-down of amalgam: part II. Implications for practising arrangements and lessons from Norway. Br Dent J 215(4):159–162. doi:10.1038/sj.bdj.2013.788
Federation FDIWD (2014) FDI policy statement on dental amalgam and the minamata convention on mercury: adopted by the FDI general assembly: 13 September 2014, new Delhi, India. Int Dent J 64(6):295–296. doi:10.1111/idj.12151
Durner J, Obermaier J, Draenert M, Ilie N (2012) Correlation of the degree of conversion with the amount of elutable substances in nano-hybrid dental composites. Dent Mater 28(11):1146–1153. doi:10.1016/j.dental.2012.08.006
Price R, Shortall A, Palin W (2014) Contemporary issues in light curing. Oper Dent 39(1):4–14. doi:10.2341/13-067-LIT
Ferracane JL, Mitchem JC, Condon JR, Todd R (1997) Wear and marginal breakdown of composites with various degrees of cure. J Dent Res 76(8):1508–1516
Shortall A, El-Mahy W, Stewardson D, Addison O, Palin W (2013) Initial fracture resistance and curing temperature rise of ten contemporary resin-based composites with increasing radiant exposure. J Dent 41(5):455–463. doi:10.1016/j.jdent.2013.02.002
Xu X, Sandras DA, Burgess JO (2006) Shear bond strength with increasing light-guide distance from dentin. J Esthet Restor Dent 18(1):19–27 discussion 28
Vandewalle KS, Ferracane JL, Hilton TJ, Erickson RL, Sakaguchi RL (2004) Effect of energy density on properties and marginal integrity of posterior resin composite restorations. Dent Mater 20(1):96–106
Randolph LD, Palin WM, Bebelman S, Devaux J, Gallez B, Leloup G, Leprince JG (2014) Ultra-fast light-curing resin composite with increased conversion and reduced monomer elution. Dent Mater 30(5):594–604. doi:10.1016/j.dental.2014.02.023
Ilie N, Durner J (2014) Polymerization kinetic calculations in dental composites: a method comparison analysis. Clin Oral Investig 18(6):1587–1596. doi:10.1007/s00784-013-1128-7
Czasch P, Ilie N (2013) In vitro comparison of mechanical properties and degree of cure of bulk fill composites. Clin Oral Investig 17(1):227–235. doi:10.1007/s00784-012-0702-8
Marovic D, Taubock TT, Attin T, Panduric V, Tarle Z (2015) Monomer conversion and shrinkage force kinetics of low-viscosity bulk-fill resin composites. Acta Odontol Scand 73(6):474–480
Li X, Pongprueksa P, Van Meerbeek B, De Munck J (2015) Curing profile of bulk-fill resin-based composites. J Dent. doi:10.1016/j.jdent.2015.01.002
Li J, Li H, Fok AS, Watts DC (2009) Multiple correlations of material parameters of light-cured dental composites. Dent Mater 25(7):829–836. doi:10.1016/j.dental.2009.03.011
Price RB, Whalen JM, Price TB, Felix CM, Fahey J (2011) The effect of specimen temperature on the polymerization of a resin-composite. Dent Mater 27(10):983–989. doi:10.1016/j.dental.2011.06.004
Bouschlicher MR, Rueggeberg FA, Wilson BM (2004) Correlation of bottom-to-top surface microhardness and conversion ratios for a variety of resin composite compositions. Oper Dent 29(6):698–704
Erickson RL, Barkmeier WW (2014) Curing characteristics of a composite. Part 2: the effect of curing configuration on depth and distribution of cure. Dent Mater 30(6):134–145. doi:10.1016/j.dental.2014.02.013
International Standard 4049 (2009) Polymer-based restorative materials (2009). ISO, Geneva
Kleverlaan CJ, de Gee AJ (2004) Curing efficiency and heat generation of various resin composites cured with high-intensity halogen lights. Eur J Oral Sci 112(1):84–88
Flury S, Hayoz S, Peutzfeldt A, Husler J, Lussi A (2012) Depth of cure of resin composites: is the ISO 4049 method suitable for bulk fill materials? Dent Mater 28(5):521–528. doi:10.1016/j.dental.2012.02.002
Fan PL, Stanford CM, Stanford WB, Leung R, Stanford JW (1984) Effects of backing reflectance and mold size on polymerization of photo-activated composite resin. J Dent Res 63(10):1245–1247
Harrington E, Wilson HJ (1993) Depth of cure of radiation-activated materials–effect of mould material and cavity size. J Dent 21(5):305–311
Ash MM, Nelson SJ, Ash MM (2003) Wheeler's dental anatomy, physiology, and occlusion, 8th edn. W.B. Saunders, Philadelphia
Vandewalle KS, Roberts HW, Rueggeberg FA (2008) Power distribution across the face of different light guides and its effect on composite surface microhardness. J Esthet Restor Dent 20(2):108–117 discussion 118. doi:10.1111/j.1708-8240.2008.00160.x
Price RB, Labrie D, Rueggeberg FA, Felix CM (2010) Irradiance differences in the violet (405 nm) and blue (460 nm) spectral ranges among dental light-curing units. J Esthet Restor Dent 22(6):363–377. doi:10.1111/j.1708-8240.2010.00368.x
Arikawa H, Kanie T, Fujii K, Takahashi H, Ban S (2008) Effect of inhomogeneity of light from light curing units on the surface hardness of composite resin. Dent Mater J 27(1):21–28
Michaud PL, Price RB, Labrie D, Rueggeberg FA, Sullivan B (2014) Localised irradiance distribution found in dental light curing units. J Dent 42(2):129–139. doi:10.1016/j.jdent.2013.11.014
Haenel T, Hausnerova B, Steinhaus J, Price RB, Sullivan B, Moeginger B (2015) Effect of the irradiance distribution from light curing units on the local micro-hardness of the surface of dental resins. Dent Mater 31(2):93–104. doi:10.1016/j.dental.2014.11.003
Shortall AC, Felix CJ, Watts DC (2015) Robust spectrometer-based methods for characterizing radiant exitance of dental LED light curing units. Dent Mater 31(4):339–350. doi:10.1016/j.dental.2015.02.012
de Magalhaes Filho TR, Weig Kde M, Werneck MM, da Costa Neto CA, da Costa MF (2015) Odontological light-emitting diode light-curing unit beam quality. J Biomed Opt 20(5):55005. doi:10.1117/1.JBO.20.5.055005
Driscoll WG, Vaughan W (1978) Handbook of optics. McGraw-Hill, New York
Jandt KD, Mills RW (2013) A brief history of LED photopolymerization. Dent Mater 29(6):605–617. doi:10.1016/j.dental.2013.02.003
Price RB, Labrie D, Rueggeberg FA, Sullivan B, Kostylev I, Fahey J (2014) Correlation between the beam profile from a curing light and the microhardness of four resins. Dent Mater 30(12):1345–1357. doi:10.1016/j.dental.2014.10.001
Pearson B (1991) Speciality chemicals: innovations in industrial synthesis and applications. Elsevier Science Pub. Co., London; New York
Asmussen E, Peutzfeldt A (2003) Polymer structure of a light-cured resin composite in relation to distance from the surface. Eur J Oral Sci 111(3):277–279
Cole M, Rueggeberg FA, Looney SW, Oxford A, Hassan Z (2009) Variation comparison of depth-of-cure between scraping and chemical removal methods. J Dent Res:88: (Spec Iss A) Abstract 2436, 2009
Price RB, Rueggeberg FA, Labrie D, Felix CM (2010) Irradiance uniformity and distribution from dental light curing units. J Esthet Restor Dent 22(2):86–101. doi:10.1111/j.1708-8240.2010.00318.x
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
This was an unfunded study.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Conflicts of interest
The authors declare that they have no conflicts of interest.
Rights and permissions
About this article

Cite this article
Price, R.B., Rueggeberg, F.A., Harlow, J. et al. Effect of mold type, diameter, and uncured composite removal method on depth of cure. Clin Oral Invest 20, 1699–1707 (2016). https://doi.org/10.1007/s00784-015-1672-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-015-1672-4