
Abstract
Objectives
Maintaining pulpal vitality and achieving long-term restoration success are challenging when treating advanced caries lesions. We aimed at assessing success, survival, and influencing factors of treating advanced lesions in general dental practice.
Methods
Patient record databases from six practices in Germany were assessed. Permanent posterior teeth with lesions radiographically extending into inner dentin with sensible (vital) pulps were retrospectively evaluated. Outcome parameters were success (absence of re-treatment) and survival (absence of extraction). Mean success/survival times were estimated, and effect of treatment modifiers assessed using Lee, Wei, and Amato (LWA) regression.
Results
Two hundred thirty-two patients (308 teeth) were assessed. Lesions (93 %) included proximal surfaces. Eight teeth showed preoperative intermitting or provocation pain. Thirty four % of teeth experienced pulpal exposure during excavation. Mean follow-up time was 74 months. Mean success time was 130 months. Teeth (142/308) required re-interventions, mostly due to secondary caries and restorative or endodontic complications. Only 13 teeth required extraction (mean survival time 307 months). Hazard of failure was significantly reduced in younger patients (<40 years) (hazard ratio (HR) [95 % confidence interval (CI)] 0.57 [0.35/0.91]) and teeth without preoperative pain (0.39 [0.17/0.90]). Compared with teeth receiving amalgams, those restored using cements (2.44 [1.05/3.98]) or composites (1.64 [1.15/2.38]) had higher risk of failure. Hazard of extraction was higher in teeth with pulpal exposure (4.90 [1.36/17.7] or cement restorations (23.6 [5.56/100]).
Conclusion
Teeth with advanced lesions had high risk of failure, while risk of extraction was low.
Clinical relevance
Teeth treated for advanced lesions required re-treatment frequently but were retained long term. Age, pulpal exposure, and restoration type were associated with risk of failure or extraction.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The treatment of advanced caries lesions in teeth with vital pulps is challenging. Due to high risk of pulpal exposure and pulpal complications [1, 2] as well as limited longevity of the placed, extensive, and deep restorations [3], both treatment success and survival are limited [4, 5].
There are only few studies following teeth with advanced lesions after restorative treatment in general dental practice, mostly after stepwise excavation [6, 7]. Such data allows to estimate the long-term treatment success and survival of teeth and placed restorations as well as to investigate the effects of potential treatment modifiers. The present study retrospectively assessed the success (absence of re-treatment) and survival (absence of extraction) of permanent posterior teeth with initially vital pulps which received treatment for advanced caries lesions in general dental practices in Germany.
Methods
Data sources
This study retrospectively assessed patient record databases from general dental practices in Northern and Eastern Germany. A convenience sample of dental practices was chosen according to practice location and the willingness and ability of dentists to participate and provide access to their records. Only practices which existed minimum 10 years and had both clinical and radiographic records fully available for this time period were included.
Overall, six dentists (five males, one female; mean age at treatment 49 [range 31–63] years) from five different places (one small town, two medium-sized cities, one large city, and one metropolis) were included. Approval for database screening and anonymous data extraction was given by the ethics committee of the CAU Kiel (D-414/14). Screening was performed between April 2014 and January 2015.
Databases included clinical records and radiographs (bitewings and/or peri-apical), with digital or analogue radiographs being available, as well as claim data. All available records and radiographs from 1980 onwards were screened manually and/or using software. We included permanent posterior teeth with caries lesions radiographically extending into the inner half of the dentin with vital pulps (positive sensibility test was ascertained by records, and sensibility test performance double-checked via claim data), without spontaneous or permanent pain or sensitivity to percussion. Radiographic depth was assessed by measuring the distance from the enamel-dentin junction to the pulp through the center of the lesion. To avoid confusion of buccal or oral lesions with advanced occlusal-proximal lesions, clinical records were used to ascertain lesion location.
Treatment and data extraction
Treated teeth were premolars or permanent molars. Given the nature of this study, no formal calibration of the participating dentists was possible. Dentists thus used their standard routines with regards to caries removal and restorative procedures and the wider dental care of their patients. Caries lesions were mostly excavated using complete excavation according to the dentists, usually aiming for only hard dentin remaining on the cavity floor. Stepwise excavation was not performed. Cavities were either lined after excavation, or not, and received various restorations. The type and manufacturer of lining and restoration material were recorded. None of the practices used rubber dam. For teeth with pulpal exposure during excavation, direct capping had been provided in all but two cases, which received immediate root canal treatment. Five dentists had stated to use lining or perform direct capping without using any further coverage of the lining/capping material (usually calcium hydroxide), i.e., restorations were placed directly onto the liner/cap. One dentist covered calcium hydroxide with a flowable composite before further restoration. Any follow-up treatment was extracted from the databases and, if possible, substantiated by radiographs. Restorative follow-up treatments were usually performed via restoration renewal, not repair by all but one dentist.
Data was extracted by one reviewer (HK) using a pilot-tested spreadsheet, with continuous, ordinal, and nominal/binary data being recorded. Continuous or ordinal data was transformed into binary data if required for further statistical evaluation. The following items were extracted: practice; time of treatment; patient’s gender, age, and insurance status (publically/socially or privately insured); treated teeth and their location (dental arch, tooth type) and preoperative status (no pain/ mild or intermittent pain or pain on provocation), lesion site (occlusal/occlusal-proximal), and extension (restored surfaces); type of cavity liner used (none, resin-modified glass ionomer, calcium hydroxide, antibiotic lining), occurrence of pulp exposure, used restoration material (amalgams, composite resins, indirect restorations, glass ionomer, or zinc/phosphate cements); events (endodontic complications including pain and swelling, restorative complications including secondary caries and fracture, periodontal or other non-related complications) or last follow-up without event (censoring); and provided treatments (re-restoration/repair, endodontic or periodontal treatment, extraction). If teeth were retained, they were followed up beyond re-treatment as far as records allowed to estimate survival.
Data extraction was controlled for completeness by a second reviewer (FS), and missing data was retrieved by re-visiting the records. Plausibility was controlled independently by the two reviewers; in case of disagreement, consensus was sought by discussion.
Statistical analysis
The unit of statistical analysis was the individual patient allowing for multiple affected teeth per patient, i.e., clustering within patients. This is done using the so called Lee, Wei, and Amato (LWA) model for clustered survival data [8], which is an extension of the Cox proportional hazards model. Outcome parameters were success (absence of any interventions, i.e., no re-treatment) and survival (absence of extraction, i.e., tooth was retained). Success was determined by the time the first re-intervention was provided, while survival was determined by tooth removal regardless of any previous re-treatments. To estimate mean success and survival times, Kaplan-Meier curves were calculated.
To test for effects of potential treatment modifiers, multivariable LWA regression was used, with variables being entered stepwise if p < 0.100. Model fit was assessed using the likelihood ratio test statistic (LRS). Exponentiated regression coefficients (hazard ratios (HRs)) and 95 % confidence intervals (CIs) were used as effect estimates. Statistical significance was assumed if p ≤ 0.05. These calculations were performed with SAS 9.4, proc phreg.
Results
Two hundred thirty-two patients (mean age 28, 47 % male, 53 % female) with 308 posterior treated teeth (38 % premolars, 62 % molars) were assessed. Treatments were provided between 1980 and 2012 and were unevenly distributed between practices. The large majority of treated lesions included proximal surfaces (93 %). For eight teeth, intermitting mild pain or pain on provocation was recorded. Restorations mostly involved two or three surfaces and used amalgam (47 %) or composite resin (33 %) (Table 1). Cavity lining was usually performed (81 %). Of teeth, 34 % experienced pulpal exposure during excavation. Mean follow-up time was 74 (range 0–333) months.
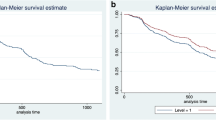
From all 308 teeth, 142 required any kind of invasive intervention during follow-up (Table 2), with mean success time being 130 months. Risk of failure differed between practices (Fig. 1a). Re-interventions were usually required due to secondary caries or restorative failures (54 %) and endodontic complications (37 %, Fig. 1b). Different materials showed different risk of failures (Fig. 1c). Only 13 teeth required extraction during follow-up. Mean survival time was 307 months (Fig. 1d). Reasons for extraction were usually endodontic or periodontal complications/need to re-treat (Table 2, Fig. 1e). Survival differed between differently restored teeth (Fig. 1f).

Kaplan-Meier curves for success (a–c) and survival (d–f). Success was determined by failure, which was defined as any invasive re-treatment. Risk of failure differed significantly between practices (a, different colors: practices) and was due restorative, endodontic, or periodontal/other interventions (b, different colors: reasons for re-treatment). Teeth which received different restorative materials (c, different colors: materials) had significantly different success times. Survival was determined by extraction and did not differ significantly between practices (indicated by different colors) (d). Extraction was required due to various reasons (e) and differed significantly between teeth restored using different materials (f)
Regression analysis found hazard of failure significantly reduced in younger (<40 years) patients (HR [95 % CI] 0.57 [0.35/0.91]) and teeth without any pain before treatment (0.39 [0.17/0.90]). Compared with teeth receiving amalgam restorations, those restored using cement (2.44 [1.05/3.98]) or composite (1.64 [1.15/2.38]) were at higher risk of failure (Table 3). Hazard of extraction was nearly fivefold increased in teeth treated for pulpal exposure (4.90 [1.36/17.7]. For teeth restored using interim materials (glass ionomer cement (GIC) or other cements), this hazard was even greater (23.6 [5.56/100]) compared with amalgam restorations (Table 3).
Discussion
The present study assessed the success and survival of posterior permanent teeth with vital pulps after treatment of advanced caries lesions. Overall, treatments from six general dental practices were evaluated, which had been provided by dentists from different locations, ages, and professional educations. Thus, this study allows to estimate the long-term treatment success and survival of teeth treated for advanced lesions, as well as to investigate the effects of treatment modifiers under selective routine dental care in Germany.
The mode of data extraction—with claim data, clinical records, and supporting radiographs being used—reduces ascertainment bias and increases the robustness of this dataset. However, the performed retrospective analysis has limitations. First, fully ascertaining the recorded clinical status (e.g., preoperative pulpal status) is difficult, and data which would be recorded in prospective studies (like caries risk or socioeconomic status of the patient) are often not available. We confirmed the performance of sensibility tests by claim data. Second, treatments were not provided at random, with indication bias being likely (e.g., GIC or other cement restorations are more often placed in teeth with questionable prognosis than composites or indirect restorations). In that sense, interpretation of potential treatment modifiers should be performed with caution, as the underlying differences might be caused by both individual treatment decisions and disease-related factors. For example, dentists and patients might aim to delay invasive re-treatments in younger patients longer than in older patients [9]. Third, dentists were not chosen at random but by convenience sampling according to practice location and willingness to participate. That heavily biases our sample, as both this willingness and the fact that we chose these practices might be indicators for confounding. However, getting access to practice records is difficult, and sampling at random would likely introduce non-response bias, which might similarly impact on our results. Our findings therefore do not claim representativeness but describe the outcomes of treatments for advanced lesions in selective routine care. Fourth, attrition might confound our results, as patients not returning could have had undetected needs due to absence of symptoms (e.g., undetected loss of vitality) or could have experienced clinical complications and had them mended elsewhere. Thus, censoring might not reflect the true risks of complications. Last, the present study is clustered, with dental practices and patients acting as clusters. We accounted for this clustering using an extension of the Cox model, i.e., the LWA model. Moreover, the sample size per practice varied greatly, with our results being unequally determined by the included studies.
The prevalence of advanced and deep lesions has been assessed in a Swedish population of adolescents, with 22 % of 14- and 15-year olds having untreated deep lesions or deep restorations [10]. The prognosis of teeth with deep restorations is thought to be compromised due to pulpal exposure or, in teeth without exposure, postoperative pulpal or restorative complications [1, 5, 11]. The present study is one of few to quantify both success and survival specifically of teeth with advanced lesions treated in general dental practice. After 10 years, 44 % of the followed teeth were free of any complications. The resulting annual failure rate is significantly higher than that reported for teeth with mostly non-deep lesions or restorations in general practice [12, 13]. It is also higher than that of teeth which had received endodontic treatment in a primary care setting [14]. In our study, the majority of failures (as indicated by provided re-treatments) were restorative or endodontic. Mean time until failure was 130 months (11 years), which is relatively long, but differed greatly between practices. When translating re-treatment into survival, only very few teeth were lost over a mean of 74 months, which demonstrates the ability of retaining teeth when providing appropriate follow-up dental care. Reasons for extractions were mostly endodontic or non-related to the advanced lesion (periodontal, other). Extraction due to restorative complications was rare. In conclusion, the chances of retaining teeth with extensive and deep restorations are higher than expected, if dentists provide tooth-retaining therapies.
We evaluated the impact of potential factors on treatment success or survival. First, teeth which had received glass ionomer or other cement restorations showed significantly higher risk of failure and extraction. While this might reflect indication bias, there is evidence that especially older glass ionomers might be inferior to other restorative materials [15]. Moreover, success was significantly lower for composites than amalgams, which might be due to treated patients having high caries risk (as indicated by the presence of an advanced untreated lesion). For those patients, composites have been shown inferior to amalgam in another practice-based study [12]. Moreover, many teeth received a cavity lining (mostly calcium hydroxide) before placing the composite, which might increase risk of failure [16], especially if no further coverage of the calcium hydroxide was attempted prior placing the composite restoration (as was the case for most teeth). We also found a trend of lower risk of failure of indirect versus direct restorations, which is expectable especially in extensively restored teeth [17–19]. Third, younger patients were at lower risk of failure, possibly reflecting the different pulpal conditions in younger versus older patients [20]. Last, we found pain and pulp exposure to significantly impact on success and survival, respectively. Teeth with intermittent or provocation pain received re-treatment significantly more often than those without, confirming reports that preoperative mild pain reduces success [21, 22].
Teeth with pulp exposure had been extracted significantly more often. Pulp exposure and subsequent direct capping have been shown to predict failure in previous studies [5, 20, 23] and to impact on tooth retention long term [24, 25]. The risk of pulp exposure was in accordance with that reported by randomized trials for those arms, where dentists aimed to “completely” remove all carious dentine in advanced lesions [11].
In conclusion, the present retrospective practice-based study found vital teeth with advanced caries lesions to have relatively high risk of failure, i.e., teeth frequently required re-treatments. Risk of failure varied between practices and was significantly higher in older patients, in teeth restored using glass ionomer or other cement as well as composite restorations, and for teeth with preoperative pain. In contrast, risk of extraction was low, as provided re-treatments allowed to retain teeth long term. Risk of extraction was increased in teeth with pulp exposure during excavation and those restored using cements. While caution is required when interpreting these data due to the associated high risks of bias, avoiding pulpal exposure and immediately placing definitive restorative materials could increase the chances of successfully treating and retaining vital teeth with advanced caries lesions.
References
Schwendicke F, Dörfer CE, Paris S (2013) Incomplete caries removal: a systematic review and meta-analysis. J Dent Res 92:306–314
Schwendicke F, Meyer-Lueckel H, Dorfer C, Paris S (2013) Attitudes and behaviour regarding deep dentin caries removal: a survey among German dentists. Caries Res 47:566–573
Hickel R, Manhart J (2001) Longevity of restorations in posterior teeth and reasons for failure. J Adhes Dent 3:45–64
Whitworth JM, Myers PM, Smith J, Walls AW, McCabe JF (2005) Endodontic complications after plastic restorations in general practice. Int Endod J 38:409–416
Schwendicke F, Stolpe M, Meyer-Lueckel H, Paris S, Dörfer CE (2013) Cost-effectiveness of one- and two-step incomplete and complete excavations. J Dent Res 90:880–887
Bjørndal L (1999) Treatment of deep carious lesions with stepwise excavation. A practice-based study. Tandlaegebladet 103:498–506
Bjørndal L, Thylstrup A (1998) A practice-based study on stepwise excavation of deep carious lesions in permanent teeth: a 1-year follow-up study. Community Dental Oral Epidemiol 26(2):122–128
Lee E, Wei LJ, Amato DA (1992) Cox-type regression analysis for large number of small groups of correlated failure time observation. In: Klein JP, Goel PK (eds) Survival analysis: state of the art. Kluwer Academic, Dordrect, pp 227–247
Burke FJ, Cheung SW, Mjor IA, Wilson NH (1999) Reasons for the placement and replacement of restorations in vocational training practices. Primary Care Dent 6:17–20
Ridell K, Olsson H, Mejare I (2008) Unrestored dentin caries and deep dentin restorations in Swedish adolescents. Caries Res 42(3):164–170
Ricketts D, Lamont T, Innes NP, Kidd E, Clarkson JE (2013) Operative caries management in adults and children. Cochrane Database Syst Rev 28, CD003808
Opdam NJ, Bronkhorst EM, Loomans BA, Huysmans MC (2010) 12-year survival of composite vs. amalgam restorations. J Dent Res 89:1063–1067
Opdam NJ, Bronkhorst EM, Roeters JM, Loomans BA (2007) A retrospective clinical study on longevity of posterior composite and amalgam restorations. Dent Mater 23:2–8
Skupien JA, Opdam N, Winnen R, Bronkhorst E, Kreulen C, Pereira-Cenci T, Huysmans MC (2013) A practice-based study on the survival of restored endodontically treated teeth. J Endod 39:1335–1340
Hickel R, Kaaden C, Paschos E, Buerkle V, García-Godoy F, Manhart J (2005) Longevity of occlusally-stressed restorations in posterior primary teeth. Am J Dent 18:198–211
Pallesen U, van Dijken JWV, Halken J, Hallonsten A-L, Höigaard R (2013) Longevity of posterior resin composite restorations in permanent teeth in public dental health service: a prospective 8 years follow up. J Dent 41:297–306
Plasmans PJJM, Creugers NHJ, Mulder J (1998) Long-term survival of extensive amalgam restorations. J Dent Res 77:453–460
Van Nieuwenhuysen JP, D’Hoore W, Carvalho J, Qvist V (2003) Long-term evaluation of extensive restorations in permanent teeth. J Dent 31:395–405
Burke FJ, Wilson NH, Cheung SW, Mjor IA (2001) Influence of patient factors on age of restorations at failure and reasons for their placement and replacement. J Dent 29(5):317–324
Aguilar P, Linsuwanont P (2011) Vital Pulp therapy in vital permanent teeth with cariously exposed pulp: a systematic review. J Endod 37:581–587
Bjørndal L, Reit C, Bruun G, Markvart M, Kjaeldgaard M, Nasman P, Thordrup M, Dige I, Nyvad B, Fransson H, Lager A, Ericson D, Petersson K, Olsson J, Santimano EM, Wennstrom A, Winkel P, Gluud C (2010) Treatment of deep caries lesions in adults: randomized clinical trials comparing stepwise vs. direct complete excavation, and direct pulp capping vs. partial pulpotomy. Eur J Oral Sci Eur J Oral Sci 118:290–29722
Dammaschke T, Leidinger J, Schafer E (2010) Long-term evaluation of direct pulp capping—treatment outcomes over an average period of 6.1 years. Clin Oral Investig 14:559–567
Schwendicke F, Stolpe M (2014) Direct pulp capping after a carious exposure versus root canal treatment: a cost-effectiveness analysis. J Endod 40:1764–1770
Barthel CR, Rosenkranz B, Leuenberg A, Roulet J-F (2000) Pulp capping of carious exposures: treatment outcome after 5 and 10 years: a retrospective study. J Endod 26:525–528
Al-Hiyasat AS, Barrieshi-Nusair KM, Al-Omari MA (2006) The radiographic outcomes of direct pulp-capping procedures performed by dental students. J Am Dent Assoc 137:1699–1705
Acknowledgments
We thank the dentists and their staff for allowing screening of databases and data extraction within their premises.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding statement
This study was funded the authors and their institutions.
Conflict of interest
The authors have no conflict of interest to declare.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Approval for database screening and anonymous data extraction was given by the ethics committee of the CAU Kiel (D-414/14).
Rights and permissions
About this article

Cite this article
Schwendicke, F., Krüger, H., Schlattmann, P. et al. Restoration outcomes after restoring vital teeth with advanced caries lesions: a practice-based retrospective study. Clin Oral Invest 20, 1675–1681 (2016). https://doi.org/10.1007/s00784-015-1654-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-015-1654-6