
Abstract
Objectives
The aim of this study was to evaluate the image quality and dose exposition of different cone-beam computed tomography (CBCT) and low-dose multislice spiral CT (MSCT) scanners.
Materials and methods
A human cadaver head was examined with three MSCT and five CBCT scanners. The radiation dose was measured using an Alderson RANDO phantom. Standard protocols were used to obtain the CBCT data. For the MSCT devices, the tube voltage and tube current were modified to obtain acceptable image quality while keeping the radiation dose as low as possible. The image quality of MSCT and CBCT devices was determined by examining the enamel–dentin and dentin–pulp interface and the periodontal ligament space of 22 teeth.
Results
Inter- and intra-observer agreement was found for the different groups of raters. CBCT systems were rated superior to MSCT devices in terms of image quality for all dental structures. The differences in image quality among the studied CBCT and MSCT scanner groups did not turn out to be significant but were significant between CBCT and MSCT devices. The organ dose varied considerably between the different CBCT and MSCT devices. The differences concerning the organ dose were notably pronounced in the area of the eye lens.
Conclusions
The tested devices exhibited significant differences with respect to the organ dose. The variance was particularly pronounced in the CBCT devices. With a dose exposition equal or lower than the CBCT, the image quality in the MSCT devices was judged to be significantly worse.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Sectional imaging is an essential component not only for the medical assessment of teeth and the surrounding bone but also for the therapy planning of pathologies of the viscerocranium and the interdisciplinary treatment planning in orthodontics and oral/maxillofacial surgery.
High-resolution three-dimensional overlap-free representation for complex medical problems has usually been carried out by means of multislice computed tomography (MSCT) [1]. With cone-beam CT (CBCT), a new imaging modality is increasingly being used in dental imaging [2–7]. In CBCT, a small C-arm-type tube detector configuration is rotated around the patient’s head. The scan geometry results in a scanning range with a more restricted field of view (FOV) than in MSCT. The size of the cylindrical FOV can vary from small fields for the imaging of selected teeth to larger fields for the imaging of the entire craniofacial area [8, 9]. In the past, various studies have concerned themselves with various CBCT scanners, whose advantage over conventional MSCT devices—that the effective radiation exposure for the patient is up to 15 times lower [10–12] with a comparable diagnostic value—was confirmed [6, 7, 9, 13–15]. The lower effective dose is due to technical features of CBCT devices, such as cone-beam geometry, low tube current values, and detector properties [16]. Furthermore, the cone-beam technique provides a rapid decrease in the dose from the area of the primary beam to the direct vicinity with a relatively clear delineation to scatter radiation [17]. Only a few studies have dealt with the comparison of image quality in dental MSCT and CBCT devices. Such comparisons were usually based on patient data [2, 8, 15, 18]; more rarely, test specimens and phantoms have been used [19, 20]. In the previous studies, however, very different protocols were usually used in the comparison of MSCT and CBCT devices, which do not permit a fair comparison. While little can be changed in the settings of CBCT devices, MSCT scanners offer the radiologist the ability to precisely adapt the scan parameters to the diagnostic problem, which can have a substantial influence on the dose.
Kyriakou et al. [20] compared different CBCT scanners in their standard settings with a low-dose MSCT and determined that a reduction of the effective dose—even below the level of a CBCT examination—was possible without sacrificing image quality. However, it is important to bear in mind that this is only valid for CBCTs with large fields and relatively high exposure. In the study by Kyriakou et al. [20], the image quality was assessed using various physical phantoms. The aim of our study was to evaluate the image quality on the basis of a complete human cadaver head, taking into account very fine-scale dental structures. Furthermore, the organ doses of the five studied CBCT units with standard settings and three MSCT devices with customized investigation parameters were to be compared.
Methods
Skull phantom
A fresh frozen cadaver head of a female Caucasian adult, provided by the Institute of Anatomy, xxxx, was used as a phantom for imaging by various CBCT and MSCT scanners. The tooth status of the patient revealed filling-free teeth as well as different metal crowns and fixed partial dentures in the upper and lower jaw. The number of teeth totaled 22. All the upper teeth (three molars, two premolars, two canines, and four front teeth) as well as two molars and one premolar in the lower jaw had metal crown restorations; apart from that, the other teeth (two premolars, two canines, and four front teeth) in the lower jaw had no restoration at all. All teeth were evaluated separately to compare the image quality of the different CBCT and MSCT scanners.
Radiation dose assessment
Radiation exposure was determined using an anthropomorphic head and neck Alderson RANDO (The RANDO® Phantom, Alderson Research Laboratories Inc., Stamford, CT, USA). This phantom consists of a human skull embedded in an isocyanic rubber equivalent to human soft tissues in terms of the anatomic number and a specific density of 0.985 g/cm3. Absorption and spread regarding radiation match that of human tissue. The phantom consists of ten axial sections with a thickness of 2.5 cm; each section is provided with holes in which lithium fluoride thermoluminescent dosimeters (LiF-TLDs; The Harshaw Chemical Company, Crystal and Electronics Products Department, Solon, OH, USA) were inserted (TLD-100 rods, diameter 1 mm, height 6 mm). For all examinations, sections 0 to 9 were equipped with TLDs. TLDs were placed at specific anatomical positions to define the radiation dose of the level of the TLD locations of selected organs (cerebrum, eye lens, thyroid gland, etc.). All dosimeters were gauged with the corresponding radiation quality. Thirty-six TLDs were positioned at 13 defined organ regions (Table 1) for each measurement (~3 TLDs per organ). Within 15–18 h after exposure, the readout of the thermoluminescent dose values was obtained with a UD 505 A TLD reader (Matsushita Electric, Osaka, Japan). In order to measure above the detection limit of the TLDs, the phantom was exposed three times and the resulting values were divided by 3. The organ dose results were the average value of the evaluated data of the three TLD rods per measuring point. Dose values (in milligray) were calculated by applying a calibration factor of 0.47 mGy/nC. Thereby, the light emission (measured in coulomb) of each individual LiF-TLD was evaluated by the readout device and multiplied with the calibration factor. The calibration factor was measured by applying a well-defined radiation exposure under laboratory conditions. No organ fractions where used throughout the whole evaluation. The individual LiF-TLD positions were weighted equally.
Imaging systems
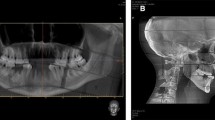
The following CBCT scanners were evaluated: 3D Accuitomo 170 (J. Morita Inc., Japan), 3D eXam (KaVo Dental GmbH, Germany), Pax Zenith 3D, Pax Reve 3D, and Picasso Trio 3D (E-Woo, South Korea). Standard protocols recommended by the manufacturer were used with all CBCT units (Table 2). Some scanners offered additional parameters to increase the radiation dose (i.e., for reducing metal artifacts or for high resolution), but these dedicated protocols were disregarded. The head and the RANDO® phantom were positioned using the built-in laser orientation guide in each unit so that the occlusal plane was parallel to the scan plane in the center of the scan field. MSCT scanning was performed on a 10-, 64-, and 128-slice CT system (SOMATOM Sensation 10, SOMATOM Sensation 64, SOMATOM Definition Flash; all from Siemens Healthcare, Forchheim, Germany) to represent different generations of MSCT systems (Fig. 1, Table 3). Anatomy-based online tube current modulation was used as appropriate. An identical reference tube current, tube voltage, rotation time, and pitch factor were employed with the goal of attaining the lowest possible radiation dose. Because minimum slice thickness varied between the MSCT systems, all raw data were reconstructed uniformly with 0.75 mm every 0.3 mm using a bone kernel (H 60 s).

Presentation of the assessed dental and periodontal structures (Table 3). a 3D Accuitomo 170 (J. Morita Inc., Japan), b 3D eXam (KaVo Dental GmbH, Germany), c Pax Reve 3D, d Pax Zenith 3D, e Picasso Trio (all from E-Woo, South Korea), f SOMATOM Definition Flash, g SOMATOM Sensation 10, and h SOMATOM Sensation 64 (all MSCT devices were from Siemens AG, Healthcare Sector, Germany)
Data transfer and image quality assessment
The volume data sets were stored in DICOM format. Since not all data sets could be transferred to our regular PACS viewer because of inconsistencies of the DICOM format, the data sets were evaluated on a dedicated 3D workstation using the software OsiriX v5.0.0 (OsiriX). The workstation was connected with a 2-megapixel grayscale monitor (RadiForce® GX240, EIZO Nanao AG, Wädenswil, Schweiz), and MPR, windowing (center/WW), and zooming were freely available. The window level sets were optimized before analysis for each different data set and could be manipulated during the assessment at the reader’s discretion. For image quality evaluation, the method proposed by Holberg et al. [3] and Liang et al. [15] was used (Tables 4 and 5). The data sets were evaluated in consensus by two experienced observers (one dentist and one radiologist, group 1). Two additional observers analyzed image quality in a separate reading session to test for reproducibility of the results (groups 2 and 3). The evaluation of the data took place on two different examination days, which were separated by an interval of at least 4 weeks. All observers were highly experienced in the analysis of CBCT and MSCT scans and were blinded to all image acquisition details. The image quality of five different dental and periodontal structures (Table 5) was assessed.
Statistical analysis
The image quality was measured by the raters using an ordinal performance scale with five levels (Table 5). This scale was used for all five dental and periodontal parameters as the enamel–dentine junction; the dentine–pulp border; and the cervical, middle, and apical thirds of the periodontal space (Table 4). A generalization of Cohen’s kappa coefficient (iota coefficient) was used to estimate the agreement between raters (inter- and intra-rater agreement) [21, 22]. The iota coefficient is a generalization of Cohen’s kappa to multiple raters and multiple outcome variables (here, the five dental and periodontal structures). Because it is essentially a weighted average of pairwise kappa values, the range of the iota coefficient is the same as for Cohen’s kappa. Specifically, it equals 1 if agreement between raters is perfect. Conversely, an iota value of 0 indicates agreement expected by chance. Interested readers are referred to reference [22] for a detailed mathematical derivation of the iota coefficient. For each of the eight devices, the image quality was summarized using descriptive statistical methods such as arithmetic means, medians, and standard deviations. Friedman tests were used to detect significant differences between the image quality ratings obtained from the MSCT and CBCT devices.
Significant results obtained from the Friedman test indicated that some of the devices showed significant differences in image quality. On the other hand, the Friedman test does not provide information about which devices are different but merely indicates that there is some difference in scoring. Therefore, in order to assess which pairs of devices showed significant differences in image quality, Wilcoxon–Nemenyi–McDonald–Thompson tests were applied [23]. p values of this procedure were adjusted for multiple comparisons. A two-sided significance level of 0.05 was used for all hypothesis tests.
Results
Inter-rater agreement
Agreement between the different groups of raters was substantial according to Landis and Koch [24] (iota coefficient of group 1 versus group 2: k 1/2 = 0.88, 95 % confidence interval [0.48, 0.92]; iota coefficient of group 1 versus group 3: k 1/3 = 0.87, 95 % confidence interval [0.47, 0.89]; iota coefficient of group 2 versus group 3: k 2/3 = 0.83, 95 % confidence interval [0.40, 0.90]). This result guaranteed the comparability of image quality ratings even if they were obtained from different raters. Average kappa values for the parameters were 0.788 (group 1 versus group 2, median 1), 0.71 (group 1 versus group 3, median 0.93), and 0.67 (group 2 versus group 3, median 0.78).
Intra-rater agreement
Concerning the intra-rater agreement, the agreement was very high and could be rated as almost perfect according to Landis and Koch [24] (iota coefficient of group 1: 0.998, 95 % confidence interval [0.995, 1]; iota coefficient of group 2: 0.995, 95 % confidence interval [0.946, 0.998]; iota coefficient of group 3: 0.998, 95 % confidence interval [0.971, 1]) Mean kappa values were 0.980 (group 1, median kappa 1), 0.9 (group 2, median kappa 1), and 0.959 (group 3, median kappa 0.78).
Image quality
The results obtained from the descriptive statistical analysis are summarized in Table 6. Image quality for all CBCT systems were rated higher than for MSCT. This result was uniformly observed in all five examined dental and periodontal variables. While the average quality ratings obtained from the CBCT ranged between 3.00 and 4.86 (moderate to excellent quality), the corresponding ratings obtained from the MSCT ranged between 1.55 and 2.63 (insufficient to moderate quality). The results obtained from the descriptive statistical analysis were further confirmed by the graphical analysis presented in Fig. 2. Within the group of MSCT devices, the best image quality was obtained from the SOMATOM Definition Flash (mean values between 2.33 and 2.63) while the worst image quality was obtained from the SOMATOM Sensation 10 (mean values between 1.55 and 2.02). Again, this result was uniformly observed in all five dental and periodontal parameters.

Error bar plot for the enamel–dentin border (a), the dentin–pulpal border (b), and the apical third of the periodontal space (c) showing means (dots) and standard deviations (±) of the image quality ratings
For all outcome variables, Friedman tests resulted in p values smaller than 0.001, suggesting that the devices differed significantly in image quality. Pairwise comparisons of the eight devices revealed that the SOMATOM Sensation10 and Sensation 64 performed significantly worse than the five CBCT devices (adjusted p values of Wilcoxon–Nemenyi–McDonald–Thompson tests <0.05, Table 7). This result was obtained for all dental and periodontal parameters. Differences between the SOMATOM Definition Flash (being the best of the examined MSCT devices) and the CBCT devices were not found to be uniformly significant. Nevertheless, most of the pairwise comparisons between the SOMATOM Definition Flash and the CBCT devices resulted in significant differences in image quality.
Organ dose
The measured organ doses at the level of the TLD locations of the different irradiated organs in the RANDO phantom are presented in Table 8 together with the irradiated tissue. The 3D Accuitomo 170 showed the highest dose for the TLDs located in the area of the brain and the eye lens (TLD levels 1–4, see Table 1), whereas for all organs considered in this study, the Picasso Trio displaced the lowest doses for the irradiated organs. Concerning the dose for the TLDs located in the area of the thyroid gland (TLD levels 8–9), the discrepancy between the chosen devices was enormous. The highest dose was measured for the Pax Reve 3D (2.78 mSv), with the SOMATOM Sensation 64 (2.12 mSv) concisely below. All the other devices displayed a distinctly lower dose (0.43–1.54 mSv).
Discussion
The objective of this study was to compare the image quality and the radiation dose of CBCT images using standard settings with deliberately strongly reduced low-dose MDCT devices. While numerous studies comparing the image quality or dose of CBCT and MSCT devices in standard protocols exist [2, 5, 8, 15, 16, 18, 19, 25], only a few investigators [16, 20, 26] have addressed the comparison of the image quality of CBCT devices with low-dose MSCT devices. Only Kyriakou et al. [20] used the method of investigating the image quality of both types of devices at the same dose levels (CT dose index, CTDI). In this case, the dose measurement was performed in an ionization chamber in a cylindrical PMMA phantom; the image quality was examined using established phantoms to determine the spatial resolution, the contrast behavior, and the pixel noise. Since the physical principles have been studied exhaustively using phantoms [20], we decided on a method of examination that was as practical as possible. Due to reasons of radiation hygiene, the implementation of the various procedures is forbidden in living subjects. Since anatomical conditions influence the weakening of the X-rays and thus the image quality [6], we decided to use a freshly frozen complete human cadaver head as the subject of our investigation.
Image quality
With regard to the representation of skeletal structures, numerous studies indicate that CBCT devices have high imaging precision; significant differences have been found between different CBCT device types [2, 9, 15, 18, 19, 27–30]. This is also in agreement with our experience: In terms of the investigated dental and periodontal parameters, there were marked differences in image quality within the group of CBCT devices; however, these did not prove to be statistically significant. The same is true for the group of MSCT devices. But the difference between the individual CBCT systems and the strongly low-dose MSCT examinations did prove to be significant. This is shown by clear differences within the groups with respect to image quality. The observed significances were found to be independent of the examined anatomic structure and were correlated solely with the corresponding device. To keep the dose to a minimum in the MSCT investigations, a very low tube voltage (80 kV) was deliberately used under experimental conditions. This accepted the fact that the low tube voltage results in an increase in image noise, which explains the relatively insufficient image quality compared to the CBCT devices in the assessment of extremely fine structures such as the periodontal ligament. The delineation of very dense materials such as dentine and enamel deteriorates drastically at low kilovolt values. The image quality can be significantly improved by using higher energy X-rays, but at the expense of the dose. The nominal voxel size in the present study was 0.29 mm for the MSCT data sets and 0.125 mm (3D Accuitomo 170) to 0.3 mm (3D eXam) for the CBCT data sets. The voxel size of the devices used apparently did not have a direct influence on the image quality results, which agrees with the results of Damstra et al. [31]. Kyriakou et al. [20] found that CBCT devices supply significantly more inhomogeneous images than MSCT devices. A further study found that another disadvantage of CBCT devices is the insufficient calibration of the CT values, which prevents quantitative assessments of bone density [32]. Causes for this include physical effects such as hardening, scattered radiation, and detector weaknesses [20].
CBCT radiation dose
As has already been observed by Pauwels et al. [33], the differences in the organ dose depending on the type of instrument used among the investigated CBCT scanners were striking. A direct comparison of the absolute values of the organ dose between the different devices was possible only to a restricted degree, however, since the organ dose depends not only on the detector size and the FOV but also on other factors, such as the type of detector material and the selected investigation parameters. The investigated CBCT devices with the standard settings regarding dose-related parameters (FOV, tube current time product (in milliampere-second), tube voltage (in kilovolt)) used in this study differ significantly [7, 20, 25, 29, 34]. Because of the different detector size in the CBCT devices, there are clear differences in the FOV and thus also in the dose. Depending on the positioning of the FOV, this can lead to large differences in the radiation dose of the individual radiosensitive organs in the same investigated device. A direct comparison of the organ dose determined here with previously published studies did not appear reasonable because the phantoms used in each study differed significantly in terms of the number and positioning of the TLDs as well as the settings used [7, 9, 10, 14, 25, 29, 33]. If the number of TLDs is too low, for example, the outcome of the dose measurement can be incorrect by up to 80 % [33].
MSCT radiation dose
Particularly among the low-dose MSCT devices, a comparison with the literature was not possible due to the extreme choice of parameters. Despite the fact that the FOV, tube voltage, and tube current were identical, the doses of the three MSCT devices differed due to different detector geometries and material, pre-filtering, and tube current modulation. This can be seen in the varying CTDI values [1]. A reduction of the tube current time product (in milliampere-second) and tube voltage (in kilovolt) leads to a reduction in radiation exposure. Reducing the tube current time product (in milliampere-second) by half also decreases the applied dose by 50 %, and the contrast-to-noise ratio is reduced by the square root of 2. This means that when the dose decreases and the tube current time product is reduced, noise increases disproportionally [7]. Suomalainen et al. [7] and Kyriakou et al. [20] determined that the use of low-dose protocols led to a similar high-contrast resolution with CBCT and MSCT devices at comparable organ doses.
CBCT–MSCT comparison
We did not believe that a consideration of the effective dose was reasonable because of the significant differences regarding the field of view specified by the manufacturer for the CBCT. Furthermore, we only used the head part of the RANDO Phantom, because our initial measurements have shown that all other organ doses are neglectable. Therefore, we can only give organ dose values. If the dose values for the individual studied radiosensitive organs are examined, significant differences with respect to the organ dose become apparent, particularly in the area of the cerebrum; these can be mainly explained by the different z-coverage of the devices tested. Due to the low coverage in the z-direction, i.e., in the area of the longitudinal body axis, only very low organ doses were measured when focusing on the dental area in the cerebrum and the cerebellum—as is the case for the eye lenses using the Picasso Trio—since only scattered radiation is involved here. The height of scan might also be the reason why for the Picasso Trio only relatively low organ doses were measured.
For the other CBCT units—which exhibited a larger scan volume in the z-direction, which resulted in parts of the brain lying directly in the beam path—markedly higher dose levels were measured in the area of the brain. The differences between the studied CBCT and MSCT devices with similar FOVs were especially striking in the area of the eye lens: Particularly for the 3D Accuitomo 170, a dose of 8.30 mSv was measured for the TLDs located in the area of the eye lenses (TLD location 3, see Table 1). Interestingly, the Pax Zenith 3D, the Pax Reve 3D, and the 3D eXam, which show a comparable height of scan, displayed enormous differences regarding the dose measured at TLD location 3 (Table 1). Whereas the dose for the eye lenses was relatively low in the Pax Reve 3D (0.54 mSv), all the other TLD doses in the Pax Reve 3D were decisively higher compared to the Pax Zenith 3D and the 3D eXam. According to the Federal Office for Radiation Protection in Germany, the dosage limit for the populace in the area of the eye lens is 15 mSv [35].
Similar results were visible for the thyroid gland. Here, the dose measured at the TLD location of the thyroid gland (TLD locations 8 and 9) was highest for the Pax Reve 3D (2.78 mSv). Devices with a similar or even higher coverage in the z-direction displayed a distinctly lower dose.
If the radiation doses for the investigated MSCT devices are examined, it becomes apparent that these are nearly identical for the SOMATOM Sensation 64 and the SOMATOM Definition Flash, whereas the SOMATOM Sensation 10 displayed slightly higher dose values. The higher dose values—compared to the other two MSCT devices—for the SOMATOM Sensation 10 are caused by a tube-side preliminary filter for examinations of the head in this device. In addition, this device has a smaller distance between the focus and the detector.
Metal artifacts
In the presence of metal restorations (crowns or amalgam fillings), the resulting artifacts appeared to be less pronounced in the examined CBCT devices than in the MSCT devices, corresponding to the observations of Carrafiello [16] and Pauwels [4]. According to Kyriakou et al. [20] and Schulze et al. [36], the differences in regard to the metal artifacts between the two groups of devices are due to different scanning and scatter radiation conditions. The metal artifacts within the CBCT group were represented quite homogeneously. However, there were significant differences in the artifact behavior within the MSCT group: In the SOMATOM Definition Flash, the diagnosis of adjacent structures by light and dark stripes was disturbed less than in the SOMATOM Sensation 10 and Sensation 64.
Summary and clinical conclusions
The results make it clear that CBCT systems are a very heterogeneous group of devices which differ significantly despite a largely similar FOV, resulting in a comparable range of indications in the standard settings recommended by the manufacturer. In the present study, this manifests itself especially in significant differences in the organ doses with a similar image quality. In most of the scanners used in this study, only a slight modification of the investigation parameters is possible, whereas the 3D Accuitomo 170 allows a larger individual selection of parameters.
In contrast, the MSCT technology provides the opportunity to create an optimized investigation protocol according to medical indications [10, 20]. In our study, we decided on an extremely low-dose protocol; as a result, the organ doses for the patient were in the middle of the field for CBCT devices. However, this was significantly lower than the organ dose values of the 3D Accuitomo 170, which were in the range of a normal MSCT examination protocol [5, 11]. Yet this significant reduction in the tube current time product (in milliampere-second) and tube voltage (in kilovolt) in the MSCT devices resulted in an increase in image noise and thus to a lower picture quality compared with CBCT devices. This made it more difficult to diagnose the investigated dental structures in our study. In their study, Kyriakou et al. [20] came to the conclusion that at the same or lower radiation exposure, MSCT devices can produce more homogeneous images of equivalent quality than CBCT devices. It can be seen in our study that if the tube voltage and the tube current are reduced further, the diagnosis of delicate structures is made more difficult due to a significant increase in noise. Depending on the clinical problem, however, a critical examination must be made whether the increase in image quality, which is usually associated with a higher radiation dose for the patient, is relevant to the therapy and is therefore justified. Especially in the study of system anomalies and craniofacial malformations in children using appropriate MSCT low-dose examination protocols, exposure should be reduced as much as possible.
When choosing the adequate device for creating a 3D radiographic dataset for a given patient, several others factors apart from the radiation dose, such as the availability or the costs of the generation of a 3D data set, must be taken into account. Another important factor is surely the positioning of the patient when taking a picture and the time necessary to create the image.
From the radiological point of view, the adjustment of similar scan parameters would have been reasonable for the organ dose measurement and the investigation of the image quality. Because of the heterogeneity of the investigated devices, this was not possible.
References
Kalender WA (2005) Computed tomography: fundamentals, system technology, image quality, applications, 2nd edn. Publicis, Erlangen
Lascala CA, Panella J, Marques MM (2004) Analysis of the accuracy of linear measurements obtained by cone beam computed tomography (CBCT-New Tom). Dentomaxillofac Radiol 33:291–294
Holberg C, Steinhäuser S, Geis P, Rudzki-Janson I (2005) Cone beam computed tomography in orthodontics: benefits and limitations. J Orofac Orthop 66:434–444
Pauwels R et al (2011) Quantification of metal artifacts on cone beam computed tomography images. Clin Oral Implants Res. doi:10.1111/j.1600-0501.2011.02382.x
Coppenrath E, Draenert F, Lechel U, Veit R, Meindl T, Reiser M et al (2008) Schnittbildverfahren zur dentomaxillofacialen Diagnostik: dosisvergleich von Dental-MSCT und New Tom 9000 DVT. Fortschr Röntgenstr 180:396–401
Periago D, Scarfe W, Moshiri M, Scheetz JP, Silveira AM, Farman AG (2008) Linear accuracy and reliability of cone beam derived 3-dimensional images constructed using an orthodontic volumetric rendering program. Angle Orthod 78:387–395
Suomalainen A, Kiljunen T, Käser Y, Peltola J, Kortesniemi M (2009) Dosimetry and image quality of four dental cone beam computed tomography scanners compared with multislice computed tomography scanners. Dentomaxillofac Radiol 38:367–378
Arai Y, Tammisalo E, Iwai K, Hashimoto K, Shinoda K (1999) Development of a compact computed tomographic apparatus for dental use. Dentomaxillofac Radiol 28:245–248
Ludlow JB, Davies-Ludlow LE, Brooks SL, Howerton WB (2006) Dosimetry of 3 CBCT devices for oral and maxillofacial radiology: CB Mercuray, NewTom 3 G, i-Cat. Dentomaxillofac Radiol 35:219–226
Ludlow JB, Davies-Ludlow LE, White SC (2008) Patient risk related to common dental radiographic examination: the impact of 2007 International Commission on Radiological Protection recommendations regarding dose calculations. J Am Dent Assoc 139(9):1237–1243
Loubele M, Bogaerts R, Dijck V, Pauwels R, Vanheusden S, Suetens P et al (2009) Comparison between effective radiation dose of CBCT and MSCT scanners for dentomaxillofacial applications. Eur J Radiol 71:461–468
Okano T, Harata Y, Sugihara Y, Sakaino R, Tsuchida R, Iwai K et al (2009) Absorbed and effective doses from cone beam volumetric imaging for implant planning. Dentomaxillofac Radiol 38:79–85
Schulze D, Heiland M, Thurmann H, Adam G (2004) Radiation exposure during midfacial imaging using 4- and 16-slice computed tomography, cone beam computed tomography systems and conventional radiography. Dentomaxillofac Radiol 33:83–86
Tsiklakis K, Donta C, Gavala S, Karayianni K, Kamenopoulou V, Hourdakis CJ (2005) Dose reduction in maxillofacial imaging using low dose cone beam CT. Eur J Radiol 56(3):413–417
Liang X, Jacobs R, Hassan B, Li L, Pauwels R, Corpas L et al (2010) A comparative evaluation of cone beam computed tomography (CBCT) and multi-slice CT (MSCT). Part I: on subjective image quality. Eur J Radiol 75:265–269
Carrafiello G, Dizonno M, Colli V, Strocchi S, Taubert SP, Leonardi A et al (2010) Comparative study of jaws with multislice computed tomography and cone-beam computed tomography. Radiol med 115:600–611
Pauwels R, Theodorakou C, Walker A, Bosmans H, Jacobs R, Horner K, Bogaerts R, The SEDENTEXCT Project Consortium (2012) Dose distribution for dental cone beam CT and its implication for defining a dose index. Dentomaxillofac Radiol 41(7):583–593
Hashimoto K, Kawashima S, Kameoka S, Akiyama Y, Honjoya T, Ejima K et al (2007) Comparison of image validity between cone beam computed tomography for dental use and multidetector row helical computed tomography. Dentomaxillofac Radiol 36:465–471
Loubele M, Maes F, Jacobs R, van Steenberghe WSC, Suetens P (2008) Comparative study of image quality for MSCT and CBCT scanners for dentomaxillofacial radiology applications. Radiat Prot Dosim 129:222–226
Kyriakou Y, Kolditz D, Langner O, Krause J, Kalender W (2010) Digital volume tomography (DVT) and multislice spiral CT (MSCT): an objective examination of dose and image quality. Fortschr Röntgenstr 183:144–153
Fleiss JL, Cohen J (1973) The equivalence of weighted kappa and the intraclass correlation coefficient as measures of reliability. EPM 33:613–619
Janson H, Olsson U (2001) A measure of agreement for interval or nominal multivariate observations. EPM 61:277–289
Hollander M, Wolfe DA (1999) Nonparametric Statistical Methods, 2nd edn. Wiley, New York
Landis JR, Koch GG (1977) The measurement of observer agreement for categorical data. Biometrics 33:159–174
Ludlow JB, Ivanovic M (2008) Comparative dosimetry of dental CBCT devices and 64-slice CT for oral and maxillofacial radiology. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 106:930–938
Hofmann E, Medelnik J, Fink M, Lell M, Hirschfelder U (2011) Three-dimensional volume tomographic study of the imaging accuracy of impacted teeth: MSCT and CBCT comparison—an in vitro study. Eur J Orthod. doi:10.1093/ejo/cjr030
Rustemeyer P, Streubühr U, Suttmoeller J (2004) Low-dose dental computed tomography: significant dose reduction without loss of image quality. Acta Radiol 45:847–853
Mozzo P, Procacci C, Tacconi A, Martini PT, Andreis IA (1998) A new volumetric CT machine for dental imaging base on the cone-beam technique: preliminary results. Eur Radiol 8:1558–1564
Mah JK, Danforth RA, Bumann A, Hatcher D (2003) Radiation absorbed in maxillofacial imaging with a new dental computed tomography device. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 96:508–513
Kobayashi K, Shimoda S, Nakagawa Y, Yamamoto A (2004) Accuracy in measurement of distance using limited cone-beam computerized tomography. Int J Oral Maxillofac Implants 19:228–231
Damstra J, Fourie Z, Huddleston Slater JJ, Ren Y (2010) Accuracy of linear measurements from cone-beam computed tomography-derived surface models of different voxel sizes. Am J Orthod Dentofacial Orthop 137:16.e1–16.e6, discussion 16–7
Hirschfelder U (2008) Stellungsnahme: Radiologische 3D-Diagnostik in der Kieferothopädie (CT/DVT). J Orofac Orthoped 69:484–487
Pauwels R, Beinsberger J, Collaert B, Theodorakou C, Rogers J, Walker A et al (2011) Effective dose range for dental cone beam computed tomography scanners. Eur J Radiol 81(2):267–271. doi:10.1016/j.ejrad.2010.11.028
Swennen G, Schutyser F (2006) Three-dimensional cephalometry: spiral multi-slice vs. cone-beam computed tomography. Am J Orthod Dentofac Orthop 130:410–416
Bundesamt für Strahlenschutz (2010) http://www.bfs.de/de/ion/wirkungen/grenzwerte.html
Schulze R, Heil U, Groß DD, Dranischnikow E, Schwanecke U, Schoemer E (2011) Artefacts in CBCT: a review. Dentomaxillofac Radiol 40:265–273
Acknowledgments
This study was financially supported by the Johannes und Frieda Marohn Foundation, Friedrich-Alexander University of Erlangen-Nuremberg, Germany. Further, the authors would like to thank Prof. Winfried Neuhuber and his staff at the Institute of Anatomy for the provision of the specimen. Our special thanks to the colleagues who helped us make the measurements for the CBCT devices and who advised us during the scans: Prof. Friedrich Neukam, Erlangen; Dr. Stephan Eulert, Bayreuth; Dr. Thomas Frank, Erlangen; Dr. Stefan Kleinmayer, Amberg; Dr. Jürgen Medelnik, Erlangen; Dr. Alexander von Moller, Bamberg; Dr. Eike Palluck, Bayreuth; Drs. Thomas Kuehnel and Frank Schmidt, Forchheim; and Dr. Gilbert Vanderborght, Fürth.
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Hofmann, E., Schmid, M., Sedlmair, M. et al. Comparative study of image quality and radiation dose of cone beam and low-dose multislice computed tomography - an in-vitro investigation. Clin Oral Invest 18, 301–311 (2014). https://doi.org/10.1007/s00784-013-0948-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-013-0948-9