
Abstract
Objectives
This study aimed to investigate the root canal morphology of mandibular first premolar teeth in a population from southwestern China by micro-computed tomography (micro-CT).
Materials and methods
Human mandibular first premolars (115) were selected and prepared for micro-CT analysis with a slice thickness of 30 μm. Details of root canal orifices, canals, accessory canals, apical foramina–apical delta intercanal communication, loops and isthmuses, and mesial invagination were analyzed from reconstructed three-dimensional (3D) images.
Results
Canal patterns categorized according to the classification defined by Vertucci (Endod Top 10:3–29, 2005) as types I (65.2 %), III (2.6 %), V (22.6 %), and VII were identified (0.9 %). Accessory canals were present in 35.7 % of the samples and were predominantly located in the apical third of the root. A single apical foramen was observed in 50.4 % of the samples and two or three foramina in 28.7 % and 14.8 %, respectively. Apical delta was identified in 6.1 % of the samples and the prevalence of intercanal communication and loops was 3.5 % and 7 %, respectively. Mesial invagination of the root was identified in 27.8 % of the samples, the majority of which contained multiple canals.
Conclusions
The data obtained in this study revealed complex root morphology with high prevalence of multiple canals, more than half of which exhibited type I canal patterns.
Clinical relevance
Micro-CT was used as a noninvasive technique for 3D investigation of root canal morphology in the mandibular first premolars of a population from southwestern China. Furthermore, data obtained revealed complex anatomy of various types.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The wide variety and complexity of root canal systems was first reported by Hess in 1925. Accessory canals, intercanal communication, apical delta, multiple foramina, and multiple canals were commonly identified. Variation in root canal morphology is now considered normal and it is generally accepted that a major cause of endodontic failure results from the inability to locate, debride, shape, and obturate all canals of the root system in three dimensions. Therefore, it is critical to gain a thorough understanding of the morphology of the root canal system and its variations in order to achieve successful therapy.
A number of techniques have been used to study the morphologic characteristics of the root canal system. Traditional methods such as radiography [1], cross-sectioning [2], staining and root clearing [3, 4], scanning electron microscopy [5], and stereomicroscopy [6] are either destructive or provide only two-dimensional information. Micro-computed tomography (micro-CT) provides a noninvasive technique for more precise investigation of the root canal system [7–16]. Three-dimensional (3D) imaging of the root canal by micro-CT was first described by Dowker [17]. This technique facilitates detailed investigation of both the external and internal anatomy of the tooth which can be observed simultaneously or separately from different angles by reconstructing the 3D images. Furthermore, the characteristic of the tooth can be assessed both qualitatively and quantitatively [7, 8, 17].
Previous reports of the use of micro-CT for the investigation of the root canal system have focused on the morphology of mandibular and maxillary molars [11], with only three reports describing the root canal morphology of the mandibular first premolar [2, 9, 14]. The complexity and variety of the root canal anatomy in the first mandibular premolar is frequently neglected by endodontists and it has been reported that treatment of the mandibular first premolar has the highest failure rate resulting from an inability to recognize and treat all canals adequately [18].
Although more than half of mandibular first premolars have one canal, multiple canals have been reported with more complex classification [19–21].The aim of this study was to investigate the complexity of the root canal morphology of the mandibular first premolar in a population from southwestern China by micro-CT.
Materials and methods
Specimen selection and preparation
Human mandibular first premolars (115) were selected for micro-CT analysis from a pool of teeth extracted for orthodontic and periodontal reasons from a population from southwestern China. To ensure that all teeth examined were first premolars, detailed information of the teeth used in this research was recorded, such as the gender, age, position information, and reasons for extraction. The teeth extracted were stored in separate ampoules. Specimens were stored in 10 % neutral buffered formalin and cleaned in 5 % sodium hypochlorite solution for 24 h before being debrided of periodontal tissue and calculus. The criteria for selection were as follows: fully formed apices, no restorations with intact crowns, and no defect or carious lesions. Specimens were attached to the specimen holder (15 mm diameter) of the micro-CT equipment via an acrylic custom-made accessory. Samples were analyzed in two stages consisting of 2 h for scanning and 2 h for the reconstruction procedure.
Scanning of samples and 3D reconstruction
All samples were scanned using a desktop X-ray microfocus CT scanner (Siemens Inveon CT, Munich, Germany) and the scanning procedure was performed using 80 kV and 500 μA with a 500-ms exposure time. A 360° scan of each specimen was performed around the tooth axis with a pixel size of 14.97 × 14.97 × 14.97 μm at a distance of 30.0 μm between each cross-section. Digital data were transferred to Mimics 10.01 software (Materialise, Leuven, Belgium). The anatomy of each mandibular first premolar and root canal system was reconstructed three-dimensionally according to the instructions provided by the manufacturer with a semiautomatic threshold-based segmentation approach combined with manual editing of the slices. The transparency of the image was adjusted to render the tooth transparent while the root canal system was opaque.
Observation of root canal morphology
Reconstructed image analysis was performed by a single observer. The following observations were recorded: number and shape of root canal orifices; number and type of canals present; presence of accessory canals (defined as any branch of the main pulp canal or chamber that communicated with the external surface of the root); number of apical foramina (defined as the circumference or rounded edge, like a funnel or crater, that differentiates the termination of the cemental canal from the exterior surface of the root) [22]; number and location of intercanal communication between a second or third canal, where present (defined as a branch of the pulpal space between the main canals that did not communicate with the root surface) [22]; presence and location of loops (defined as a branch of the main canal that divides from it and then rejoins the original canal) [22]; presence of isthmus (defined as a narrow, ribbon-shaped communication between two root canals that contains pulp tissue) [23]; presence of an apical delta in the apical third of the root canal (defined as a complex ramification of branches of the pulp canal located near the anatomical apex with a main canal not being discernible).
Results
Number and shape of root canal orifices
At least one canal orifice was identified in all specimens. The shape of the canal orifice was oval in 84.3 % (97 of 115) (Fig. 1a), flattened ribbon-shaped in 7.0 % (8 of 115) (Fig. 1b), eight-shaped in 7.0 % (8 of 115) (Fig. 1c), and triangular in 1.7 % (2 of 115) (Fig. 1d).

Shapes of root canal orifices. a Oval, 84.3 %; b flattened ribbon, 7.0 %; c eight-shaped, 7.0 %; d triangular, 1.7 %. The arrow indicates the margin of the enamel–cementum junction
Canal type
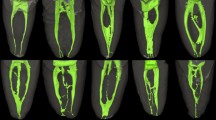
The percentages of root canal configurations in the mandibular first premolars examined are presented in Table 1. Variable root canal configurations were observed in the mandibular first premolars. Of the 115 specimens, 65.2 % (75 of 115) was identified as type I (1-1) (Fig. 2a), 22.6 % (26 of 115) as type V (1-2) (Fig. 2c), 2.6 % (3 of 115) as type III (1-2-1) (Fig. 2b), and 0.9 % (1 of 115) as type VII (1-2-1-2) (Fig. 2d). Ten specimens did not fit Vertucci’s classification. Additional types identified included: 2.6 % (3 of 115) type 1-3-2 (Fig. 2e), 5.2 % (6 of 115) type 1-3(Fig. 2f), and 0.9 % (1 of 115) type 1-2-3 (Fig. 2g).

Canal patterns in mandibular first premolars categorized by Vertucci’s classification. a Type I (1-1); b type III (1-2-1); c type V (1-2); d type VII (1-2-1-2). Additional types: e 1-3-2; f 1-3; g 1-2-3
Accessory canals
Accessory canals were present in 35.7 % (41 of 115) of the specimens. The majority of accessory canals (92.7 %, 38 of 41) were located in the apical third of the root (Table 3). Accessory canals were identified in the middle third of the roots in only three specimens. No accessory canals were observed in the cervical region. Of the specimens identified with accessory canals, the majority of specimens had a single accessory canal (87.8 %, 36 of 41), while four specimens (9.8 %, 4 of 41) had two accessory canals and one (2.4 %, 1 of 41) specimen had four accessory canals (Table 2; Fig. 3).

Accessory canals located in the apical and middle third of the root
Apical foramina and delta
Most apical foramina were located laterally (77.4 %, 89 of 115). A single apical foramen was identified in approximately half (50.4 %, 58 of 115; Fig. 4a) of the specimens. Two apical foramina were detected in 28.7 % (33 out 115) of specimens, three in 14.8 % (17 of 115), and four in 6.1 % (7 of 115; Fig. 4b; Table 2). Apical delta was present in 6.1 % (7 of 115) of specimens (Fig. 5).

Apical foramen. a Single apical foramen; b four apical foramina

a, b Apical delta, the complex structure in the tip of the root canal
Intercanal communication, loop, and isthmus
Intercanal communications were observed in 3.5 % (4 of 115) of the specimens (Fig. 6). Loops were present in 7.0 % (8 of 115) of specimens (Fig. 7). Three were located in the apical third of the root and five in the middle third. An isthmus was identified in only two specimens. These were located the middle and apical third of these specimens (Table 3).

Intercanal communication and isthmus. a Multiple intercanal communication and an uncompleted isthmus in the middle third of the root; b intercanal communication in cross-section; c an isthmus between the buccal and lingual canals; d isthmus viewed in cross-section

a Loops in the middle and b apical third of the root canal
Mesial invagination
According to Ash [24], mesial invagination is a deep developmental groove in the mesial surface of the root formed during embryogenesis, which is commonly observed in mandibular premolars. Mesial invagination of the root was observed in 27.8 % (32 of 115) of specimens. All were located in the mesial–lingual third of the root surface. These were categorized according to the classification defined by Vertucci [32] as type V (1-2) (21 of 32; Fig. 8a–d), type I (1-1) (2 of 32), type III (1-2-1) (2 of 32; Fig. 8e–h), and type VII (1-2-1-2) (1 of 32). Additional types identified included type 1-2-3 (1 of 32; Fig. 8i–l), type 1-3 (2 of 32; Fig. 8m–p), and type 1-3-2 (3 of 32; Fig. 8q–t; Table 4). Of those specimens with mesial invagination, 93.8 % (30 of 32) had two canals or more. The majority of invaginations were located in the middle third of the root and extended to the apical third with a minority dividing into two roots at the tip. Invaginations originated in the middle third of the root in 87.5 % (28 of 32) of these specimens, at the coronal third, extending to the middle and apical third of the root in 6.3 % (2 of 32), and at the apical third, extending to the tip of the root in 6.3 % (2 of 32).

Mesial invagination and corresponding root canal patterns. a–d Type V (1-2), e–h type III (1-2-1) canal with mesial invagination. Additional types include: i–l 1-2-3; m–p 1-3; q–t 1-3-2. a, e, i, m, q Contour image of the mesial surface; b, f, j, n, r 3D reconstruction of tooth; c, d, g, h, k, l, o, p, s, t C-shaped canal in cross-section
Discussion
This study investigated root canal morphology in mandibular first premolar teeth in a population from southwestern China by micro-CT. This nondestructive technique provides detailed and accurate information for the evaluation of the external and internal anatomy of the root canal system through reconstruction of 3D images.
Previous reports of aberrant morphology in the root canal of first mandibular premolars have attributed variation in the number and pattern of first premolar root canal morphology to racial or genetic factors and the investigative technique employed [25]. The occurrence of a single canal in the mandibular first premolar was reported from 54 to 88.5 %, while multiple canals were reported from 11.5 to 46 % [6, 26]. In this study, variable root canal configurations were identified. Canal type I (1-1) was the most common pattern occurring in 64.3 % of specimens and multiple canals were identified in 35.7 %. Approximately 91.3 % (105 of 115) of specimens were defined according to the traditional Vertucci [22] classification of canal configurations, while 8.7 % (10 of 115) were classified as additional types. In this study, canal orifices were identified in all samples, although type II and type IV patterns were not identified. A higher incidence of single (65.2 vs. 54 %) and double (26.1 vs. 22 %) canal patterns was observed in this study compared with the study carried out on a Chinese population by Lu et al. [21]. However, the data presented here are consistent with other reports of studies conducted among the Chinese population such as those reported Lin [27] (65.6 and 24.5 %) and Xu [28] (69.1 and 26.3 %). In contrast, a study of a Japanese population conducted using radiography and cleaning methods reported a much higher occurrence (80.6 %) of the single canal type compared with this study [20]. Other studies conducted in a Jordanian population using the cleaning method [29] and in an Iranian population using the cross-sectioning and radiography methods [26] reported the identification of type I canals with incidences of 58.2 and 88.5 %, respectively. These data indicate that root canal morphology is affected by racial factors and that multiple canals occur with a moderate frequency in the Chinese population investigated in this study. It can also be speculated that the results are influenced by the techniques employed for the investigation.
Radiography, cross-sectioning and staining, and root clearing have been the most commonly used techniques for the analysis of premolar root canal morphology. These techniques are limited to the acquisition of two-dimensional data and there are few previous reports of the use of micro-CT for the 3D investigation of premolar root morphology [2, 9, 14, 30].
In this study, accessory canals were present in 35.7 % of specimens, with most located at the apical third of the root canal. An isthmus is a narrow, ribbon-shaped communication between two root canals that contains pulp tissue or pulpally derived tissue. In this study, isthmuses were identified in 1.7 % in the middle and apical canals. The low incidence of these structures also represents a challenge to successful endodontic therapy for its complexity.
The number of apical foramen was not consistent with the root canal configuration. A relatively low percentage (76 %) of single canal foramen existed in specimens of type I canal. Multiple foramina might be the result of the existence of accessory canal and apical delta. A foramen was unusually identified on the root surface without a connection to the root canal. Approximately 77.4 % of apical foramina were located laterally, thus indicating that particular attention should be paid by clinicians to the relationship between the working length and the root length measured by X-ray imaging.
Apical delta, the most complex structure in the root canal system, was identified with an incidence of 6.1 % in this study (three specimens with one canal and four specimens with multiple canals), which was similar to the observations of Lu et al. [21]. However, the incidence of apical delta has been reported in other populations with variable frequency ranging from 5.7 % [31], 16.9 % [3], and 15.5 % [19] in Turkish populations and 29.2 % in Jordanian populations [29]. A recent study of the apical anatomy of premolars using micro-CT demonstrated that the presence of an apical delta was not an uncommon occurrence, even in a single, straight root canal [32].
Mesial invagination is a developmental groove in the mesial surface of the root, which is commonly observed in premolars. Reports have observed external developmental grooves or deep invaginations on the mesial surface in 17.6 % of first mandibular premolars [29] and mesial invagination in 14 % [33]. Furthermore, a relationship between invagination and C-shaped canal morphology has been postulated [6, 21]. In this study, a high incidence (27.8 %) of invaginations was detected, although the point of initiation and the depth of the invagination varied. Some anatomical correlations between canal configurations and invaginations were also noted. The invaginations were closely associated with canal configurations comprising multiple canals. Among the 32 specimens with mesial invaginations, only 2 were type I canals, with the highest incidence of canal configurations identified as type V (1-2) with a 65.6 % ratio (21 of 32). Others specimens were associated with more complicated canal types such as type III, type VII, and all additional types described in this study. Among the 40 specimens presenting with multiple canals, 75.0 % (30 of 40) exhibited mesial invaginations, while only 2 specimens with a single canal had invaginations. These data indicate the existence of a close correlation between invagination and a complex canal system which represents a significant challenge for endodontic therapy. Furthermore, it was observed that invaginations, particularly deep invaginations, were predominantly associated with a C-shaped canal, although this relationship requires further analysis. There is no doubt that micro-CT offers exciting potential for 3D assessment of the root canal system in great detail. As with traditional methods, micro-CT is limited to ex vivo applications only and not suitable for clinical use at the current situation. Cone beam CT (CBCT) provides the clinician with an imaging modality that is capable of achieving a 3D representation of the maxillofacial region, from anatomical tooth anomalies to the composition of periodontal defects [34]. Thus, CBCT is a great aid in dentistry to optimize clinical endodontic procedures.
Conclusion
In this study, micro-CT was used as an accurate and noninvasive technique for the investigation of root canal morphology in a population from southwestern China. Data obtained revealed the complex anatomy of various types. The most common root canal pattern was identified as type I, although multiple root canals also presented with high incidence. Furthermore, the existence of an anatomical correlation between the presence of multiple root canals in first mandibular premolars and mesial invaginations was also identified.
References
Gomes BP, Rodrigues HH, Tancredo N (1996) The use of a modeling technique to investigate the root canal morphology of mandibular incisors. Int Endod J 29:29–36
Fan B, Yang J, Gutmann JL, Fan M (2008) Root canal systems in mandibular first premolars with C-shaped root configurations. Part I: microcomputed tomography mapping of the radicular groove and associated root canal cross-sections. J Endod 34:1337–1341
Calişkan MK, Pehlivan Y, Sepetçioğlu F, Türkün M, Tuncer SS (1995) Root canal morphology of human permanent teeth in a Turkish population. J Endod 21:200–204
Neelakantan P, Subbarao C, Subbarao CV, Ravindranath M (2010) Root and canal morphology of mandibular second molars in an Indian population. J Endod 36:1319–1322
Vertucci FJ, Anthony RL (1986) A scanning electron microscopic investigation of accessory foramina in the furcation and pulp chamber floor of molar teeth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 62:319–326
Baisden MK, Kulild JC, Weller RN (1992) Root canal configuration of the mandibular first premolar. J Endod 18:505–508
Bjorndal L, Carlsen O, Thuesen G, Darvann T, Kreiborg S (1999) External and internal macromorphology in 3D-reconstructed maxillary molars using computerized X-ray microtomography. Int Endod J 32:3–9
Grande NM, Plotino G, Pecci R, Bedini R, Pameijer CH, Somma F (2008) Micro-computerized tomographic analysis of radicular and canal morphology of premolars with long oval canals. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 106:70–76
Cleghorn BM, Christie WH, Dong CC (2008) Anomalous mandibular premolars: a mandibular first premolar with three roots and a mandibular second premolar with a C-shaped canal system. Int Endod J 41:1005–1014
Fan B, Yang J, Gutmann JL, Fan M (2008) Root canal systems in mandibular first premolars with C-shaped root configurations. Part I: microcomputed tomography mapping of the radicular groove and associated root canal cross-sections. J Endod 34:1337–1341
Somma F, Leoni D, Plotino G, Grande NM, Plasschaert A (2009) Root canal morphology of the mesiobuccal root of maxillary first molars: a micro-computed tomographic analysis. Int Endod J 42:165–174
Verma P, Love RM (2010) A Micro CT study of the mesiobuccal root canal morphology of the maxillary first molar tooth. Int Endod J 44:210–217
Gu Y, Lu Q, Wang P, Ni L (2010) Root canal morphology of permanent three-rooted mandibular first molars: part II—measurement of root canal curvatures. J Endod 36:1341–1346
Aboshi H, Takahashi T, Komuro T (2010) Age estimation using microfocus X-ray computed tomography of lower premolars. Forensic Sci Int 200:35–40
Peters OA, Laib A, Ruegsegger P, Barbakow F (2000) Three-dimensional analysis of root canal geometry by high-resolution computed tomography. J Dent Res 79:1405–1409
Oi T, Saka H, Ide Y (2004) Three-dimensional observation of pulp cavities in the maxillary first premolar tooth using micro-CT. Int Endod J 37:46–51
Dowker SE, Davis GR, Elliott JC (1997) X-ray microtomography: non-destructive three-dimensional imaging for in vivo endodontic studies. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 83:510–516
Ingle JI, Taintor JF (1985) Endodontics: modern endodontic therapy. Lea & Febiger, Philadelphia
Sert S, Bayirli GS (2004) Evaluation of the root canal configurations of the mandibular and maxillary permanent teeth by gender in the Turkish population. J Endod 30:391–398
Yoshioka T, Villegas JC, Kobayashi C, Suda H (2004) Radiographic evaluation of root canal multiplicity in mandibular first premolars. J Endod 30:73–74
Lu T-Y, Yang S-F, Pai S-F (2006) Complicated root canal morphology of mandibular first premolar in a Chinese population using the cross section method. J Endod 32:932–936
Vertucci FJ (2005) Root canal morphology and its relationship to endodontic procedures. Endod Top 10:3–29
Weller RN, Niemczyk SP, Kim S (1995) Incidence and position of the canal isthmus. Part 1. Mesiobuccal root of the maxillary first molar. J Endod 21:380–383
Ash M (1999) Wheeler’s dental anatomy, physiology and occlusion. In: Ash M (ed) The permanent mandibular incisors, 7th edn. Saunders, Philadelphia, pp 228–229
Cleghorn BM, Christie WH, Dong CC (2007) The root and root canal morphology of the human mandibular first premolar: a literature review. J Endod 33:1031–1037
Khedmat S, Assadian H, Saravani AA (2010) Root canal morphology of the mandibular first premolars in an Iranian population using cross-sections and radiography. J Endod 36:214–217
Lin ZM, Fang YY, Ling JQ (2008) Morphological characteristics of the mandibular first premolars in people from Pearl River Delta region in Guangdong province. Hua Xi Kou Qiang Yi Xue Za Zhi 26:526–530
Xu Q, Xiao XF, Zhou YF, Chen M, Ling JQ (2009) Root canal morphology of mandibular incisors and mandibular first premolars in vitro. Chin J Conserv Dent 19:73–76
Awawdeh LA, Al-Qudah AA (2008) Root form and canal morphology of mandibular premolars in a Jordanian population. Int Endod J 41:240–248
Sandhya R, Velmurugan N, Kandaswamy D (2010) Assessment of root canal morphology of mandibular first premolars in the Indian population using spiral computed tomography: an in vitro study. Indian J Dent Res 21:169–173
Vertucci FJ (1978) Root canal morphology of mandibular premolars. J Am Dent Assoc 97:47–50
Plotino G, Grande NM, Pecci R, Bedini R, Pameijer CH, Somma F (2006) Three-dimensional imaging using microcomputed tomography for studying tooth macromorphology. J Am Dent Assoc 137:1555–1561
Velmurugan N, Sandhya R (2009) Root canal morphology of mandibular first premolars in an Indian population: a laboratory study. Int Endod J 42:54–58
Maret D, Molinier F, Braga J, Peters OA, Telmon N, Treil J, Inglèse JM, Cossié A, Kahn JL, Sixou M (2009) Accuracy of 3D reconstructions based on cone beam computed tomography. J Dent Res 89(12):1465–1469
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Additional information
Na Liu and Xiangjie Li contributed equally to this work as co-first authors.
Rights and permissions
About this article
Cite this article
Liu, N., Li, X., Liu, N. et al. A micro-computed tomography study of the root canal morphology of the mandibular first premolar in a population from southwestern China. Clin Oral Invest 17, 999–1007 (2013). https://doi.org/10.1007/s00784-012-0778-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-012-0778-1