
Abstract
The aim of this in vitro study was to compare the performance of two laser fluorescence devices (LF, LFpen), conventional visual criteria (VE), ICDAS and radiographic examination on occlusal surfaces of primary teeth. Thirty-seven primary human molars were selected from a pool of extracted teeth, which were stored frozen at −20°C until use. Teeth were assessed twice by two experienced examiners using laser fluorescence devices (LF and LFpen), conventional visual criteria, ICDAS and bitewing radiographs, with a 2-week interval between measurements. After measurement, the teeth were histologically prepared and assessed for caries extension. The highest sensitivity was observed for ICDAS at D1 and D3 thresholds, with no statistically significant difference when compared to the LF devices, except at the D3 threshold. Bitewing radiographs presented the lowest values of sensitivity. Specificity at D1 was higher for LFpen (0.90) and for VE at D3 (0.94). When VE was combined with LFpen the post-test probabilities were the highest (94.0% and 89.2% at D1 and D3 thresholds, respectively). High values were observed for the combination of ICDAS and LFpen (92.0% and 80.0%, respectively). LF and LFpen showed the highest values of ICC for interexaminer reproducibility. However, regarding ICDAS, BW and VE, intraexaminer reproducibility was not the same for the two examiners. After primary visual inspection using ICDAS or not, the use of LFpen may aid in the detection of occlusal caries in primary teeth. Bitewing radiographs may be indicated only for approximal caries detection.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In most industrialised nations over the last decades, there has been a general decline in the prevalence of caries [1]. In children and adolescents its detection has become difficult due to the widespread use of fluorides with superficial remineralisation potential. In order to provide efficient preventive measures for primary molars, it is of utmost importance that clinicians detect occlusal caries early [2].
Dentists have several options at their disposal for the clinical detection of occlusal dental caries, including visual-tactile examination, radiographs, fluorescence methods and electrical conductance measurements [3]. While visual inspection naturally is and should be the primary method of detection and diagnosis of dental caries, it must be kept in mind that caries detection by eyesight is better at an advanced stage than early [4]. As therefore a ’true’ diagnosis of the caries process by visual inspection is limited, there is a need to detect or quantitatively monitor such lesions in order to support treatment decisions. Auxiliary methods therefore have been tested as an adjunct to conventional examination for identifying and quantifying such lesions.
Meticulous visual inspection with a good operation light, a dry tooth and a sharp probe can render good sensitivity and specificity values of approximately 80% [5, 6]. Currently, there are primarily three systems for meticulous visual inspection in use: the Nyvad criteria [7] and International Caries Detection and Assessment System (ICDAS) [8] and UniViSS [9]. The former is useful because it integrates lesion activity characteristics. The latter is a promising tool for enhancing visual inspection because it considers the varying refraction of dry and wet enamel (important for detecting early stages of caries) and because dentin caries are subdivided into four classes. The ICDAS system has been proven to be sensitive enough to monitor progression of enamel caries in a cohort of 788 children, aged 1–5 years [10]; additionally, its combination with bitewing radiographs (BW) showed good performance in detecting occlusal dentin caries in permanent teeth [11]. This system also presented good reproducibility and accuracy in detecting occlusal caries in the outer half of the enamel in permanent teeth [12].
A laser fluorescence device (LF; DIAGNOdent, KaVo, Biberach, Germany) was introduced some years ago for caries detection [13]. More recently, a pen-type LF device (LFpen) was developed and has been tested. Both the first LF and more recent pen-type LF pen function on the same principle of excitation of a 655-nm monochromatic light and measurement of back-scattered fluorescence. At this wavelength, apart from auto-fluoresceing tooth substance fluorescing objects have been identified as bacterial protoporphyrines [13, 14].
The performance of the LF device in primary teeth was recently evaluated in vivo [15] and in vitro [16], and the results showed that this device had high reliability for detection of occlusal caries in primary teeth, and that its performance was similar to visual and radiographic examinations. However, a recent study with extracted primary molars showed that LF is better for occlusal caries extending into dentin than for occlusal enamel caries [17]. Therefore, it was recommended to be considered as a complementary tool in the detection of caries in primary teeth [18].
However, no study has tested the performance of both the LFpen and the ICDAS and compared the two with other methods for detecting occlusal caries in primary molars. Therefore, the aim of this in vitro study was to compare the benefit of additional diagnostic methods (BW, LF and LFpen) to the conventional visual criteria and ICDAS on occlusal surfaces of primary teeth.
Material and methods
Sample selection
Thirty-seven primary human molars (16 first and 21 second molars) were selected from a pool of extracted teeth. Teeth were stored frozen at −20°C until use because this storage method does not change the red fluorescence significantly [19]. The teeth were extracted by Swiss private dental practitioners (no water fluoridation; 250 ppm F- in children’s dentifrice and table salt). Prior to extraction, the patients were informed about the use of their teeth for research purposes, and their consent was obtained. After defrosting for 3 h, the teeth were thoroughly cleaned for 15 s with a toothbrush (Trisa Diamont, Triengen, Switzerland) and tap water. Periodontal remnants were removed with a Gracey curette no. 13/14, and the fissure system was additionally cleaned with sodium bicarbonate powder and water-powder-blasting device (Airflow, EMS, Switzerland) for 10 s. Powder remnants in the fissure system were removed by rinsing with a 3-in-1 syringe for 10 s [20]. During measurements, teeth were stored at 100% humidity. The occlusal surfaces were photographed at ×6.25 magnification, and one spot from each tooth was selected in the fissure surface (test site). The test site on each photograph was covered with a sticker in order not to reveal any details. All assessments with conventional and new techniques were carried out twice by two experienced examiners, with a 2-week interval between measurements.
Visual examination—ICDAS and conventional criteria
Visual examination (VE) was performed following the ICDAS criteria [8, 11, 12, 21], with direct visualisation of the teeth under illumination and coding as follows: (0) sound tooth surface, (1) first visual change in dry enamel, (2) distinct visual change in moist enamel, (3) localised enamel breakdown due to caries with no visible dentin or underlying shadow, (4) underlying dark shadow in dentin with or without localised enamel breakdown, (5) distinct cavity with visible dentin and (6) extensive distinct cavity with visible dentin. After 2 weeks, dry, clean surfaces were inspected by direct visualisation and under excellent illumination, without probing, and the visual examination was coded as: (0) sound tooth surface, (1) superficial caries lesion on enamel, (2) deep caries lesion on enamel and (3) dentin caries lesion. The teeth were examined in the same room with the aid of a light reflector and a 3-in-1 air syringe. The cut-off scores for both ICDAS and conventional visual criteria were 1 (D1) and 3 (D3).
Assessments with LF devices
The test sites were assessed using two laser fluorescence devices: LF (DIAGNOdent 2095, KaVo, Biberach, Germany) and LFpen (DIAGNOdent 2190). Both devices were first calibrated for each tooth using a ceramic standard, in accordance with the manufacturer’s instructions. The fluorescence value of a sound part of the cuspal area on the buccal surface (zero value) was then recorded for later subtraction from the peak value. For measurements, tip A (for the LF device) and a cylindrical sapphire fibre tip for occlusal surfaces (for the LFpen device) were used. The device was moved around the test site until the highest value was obtained. The peak values were recorded, and the zero value of fluorescence was subtracted [11]. The cut-off values at D1 and D3 were determined by the highest sum of specificity and sensitivity.
Bitewing radiographs
Standardised BW of all the teeth were taken using an X-ray machine (HDX Dental EZ, USA) and double Kodak Insight films (22 × 35 mm, Kodak, Rochester, MN, USA) at 65 kV, 7 mA and an exposure time of 0.09 s. An automatic XR 24 Pro X-ray film developer (Dürr Dental, Germany) was used to process the films. The radiographs were then examined independently using an X-ray viewer (Imatec Röntgentechnik, Switzerland) and an X-ray film magnifier (magnification 2; Svenska Dental Instrument, Sweden) in a dark room and were coded as follows: (0) no radiolucency, (1) radiolucency in enamel, (2) radiolucency in the outer half of dentin and (3) radiolucency in the inner half of dentin. The cut-off scores used were 1 (D1) and 2 (D3)
Validation
After the assessments, the teeth were ground longitudinally until 1 mm before the site of measurement on a Knuth-Rotor polishing machine with silicon carbide paper of grain size of 60 µm cooled under tap water. When the periphery of the site was reached by the grinding process, papers of grain size 30, 18, 8 and 5 µm were used. Subsequently, the cut surfaces were cleaned and dehydrated in solutions of increasing alcohol concentration, with the addition of basic fuchsin 0.5% (Inselspital-Apotheke, Bern, Switzerland) to achieve block staining. The alcohol was removed with acetone, and the teeth were embedded in methylmethacrylate. Each section was contrast-stained with acetic light green for 2 min. Slices of 300 µm thickness were obtained and photographs of the cut coloured surfaces were taken (Leica DC300 camera, Leica, Heerbrugg, Switzerland). Two examiners assessed the sites independently to classify the lesions. When there was disagreement, a consensus was reached. Sites were assessed for caries extension (magnification ×10) and coded as follows: (0) caries-free, (1) caries extending up to halfway through the enamel, (2) caries extending into the inner half of enamel and (3) caries in dentin.
Statistical analyses
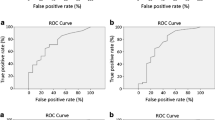
Sensitivity, specificity, accuracy and area under the ROC curve (AUC) were calculated (SPSS 14 for Mac, SPSS, Chicago, IL, USA) at D1 (caries detection) and D3 (dentin caries detection) thresholds for all methods. For this calculation, the averages of four LF and LFpen assessments, and all the scores of ICDAS and BW were used. The McNemar test was performed to verify statistically significant differences between the methods for each threshold. The optimal cut-off limits for LF and LFpen devices were determined by the point at which the sum of sensitivity and specificity was maximal.
Using the separate LR+ values for each method, the post-test probability for combinations of the methods was calculated to assess the relative value of using the different methods separately and in combination. LR+ can be used to calculate the post-test odds of a test, which then become the pretest odds for a second independent test with a known LR+, resulting in the post-test probability (odds of correct diagnostics) of their combination [11, 22].
Intraclass correlation (ICC) and Cohen’s unweighted kappa (k) values were used to assess inter- and intraexaminer reproducibility. For LF and LFpen, the Bland and Altman method was applied to identify systematic differences [23].
Results
Histological examination revealed that of the 37 occlusal test sites, 10 were caries-free, seven had caries extending up to halfway through the enamel, 11 had caries extending into the inner half of enamel and nine had caries in dentin.
Specificity, sensitivity, accuracy and AUC are shown in Table 1. The highest sensitivity values were observed for ICDAS at D1 and D3 thresholds, with no statistically significant difference when compared to the LF devices, except at D3 threshold. Additionally, bitewing radiographs presented the lowest values of sensitivity (p < 0.05). Specificity was higher for the LFpen at D1 (0.90) and for VE at D3 (0.94). The optimal cut-off limits found for the LF were 10 (D1), 12 (D2) and 17 (D3) and for the LFpen 14 (D1), 17 (D2) and 31 (D3), shown in Table 2.
Table 3 gives an overview of the probabilities of correct detection at D1 and D3 thresholds when the methods were used independently and in combination. When VE was combined with the LFpen, the post-test probabilities were the highest (94.0% and 89.2% at D1 and D3 thresholds, respectively). High values were observed for the combination of ICDAS and the LFpen (92.0% and 80.0%, respectively).
Reproducibility values are represented in Table 4. LF and LFpen showed the highest ICC values for interexaminer reproducibility. However, the intraexaminer correlation was not the same for both examiners. ICC and kappa values were higher for examiner A than for examiner B. Regarding intraexaminer reliability, the mean difference in LF measurements was 0.4 (examiner A) and 1.9 (examiner B), respectively; for LFpen the mean was 0.4 (examiner A) and 2.5 (examiner B), respectively. The intervals of ±1.96 standard deviations (SD) 21.3/ 43.4 for LF and 38.1/ 37.8 for LFpen. Regarding interexaminer reproducibility, the mean difference was −3.7 for LF and −4.1 for LFpen, respectively. The intervals of ±1.96 SD were found to be 29 for LF and 36.1 for LFpen, respectively.
Discussion
Recently, there has been some criticism of the use of the overall accuracy to pinpoint the validity of a given diagnostic test, because of its prevalence-dependent nature [24]. It was concluded that there is a systematic distortion of the overall accuracy when the prevalence is far from 50% or when sensitivity and specificity differ greatly. Regarding the prevalence in this study, it is remarkable that the distribution of caries severity happened to be almost equal. This distribution did not occur in many other diagnostic studies, which typically showed a higher prevalence of easier-to-detect D3 lesions [25–27]. Regarding the equal distribution of caries grades in this study, the use of accuracy in addition to sensitivity, specificity and AUC seems justified to generate a single summary estimate of the validity of the methods used. In this in vitro study, a relatively low number (37) of teeth was used, being about three [15] to four [17] times less than other studies. However, compared to those studies, in this study frozen primary teeth were used. It was shown that frozen teeth maintain the fluorescence signal much better than other storage methods [19]. Thus, despite of the number of teeth in this study its design may represent clinical conditions better.
This in vitro study is the first to evaluate the performance of the LFpen device and the ICDAS criteria in the detection of occlusal caries in primary teeth. LF devices, like any tool in caries diagnostics, should ideally be highly sensitive and highly specific. Within the limitations of an in vitro study, it was observed that the ICDAS performed better and presented the highest values of sensitivity at the thresholds evaluated, although statistically significant differences were only found at D3. In a previous assessment of permanent teeth, ICDAS and LFpen presented similar results, showing no significant difference in the values of sensitivity at the D3 threshold [11]. Visual examination alone was shown to have low sensitivity, but high specificity. ICDAS showed the best correlation with histology, and this method has been previously suggested to be the best for detecting changes in enamel [11]. First clinical results of the new ICDAS criteria seem to be promising, because they provide an acceptable prediction of caries depth [21, 28].
LF and LFpen devices demonstrated high sensitivity on the occlusal surfaces of the primary teeth at both thresholds evaluated. The performance was similar to that found by Lussi and Francescut [29] and Attril and Ashley [30] using the first LF device in primary teeth. However, in the literature, most studies assessed permanent teeth, and the comparison of such results to those obtained assessing primary teeth must be made with caution. Braga et al. [17] assessing occlusal caries in primary teeth concluded that the LF device performs better at the dentine threshold as its capability to detect enamel caries was found to be poor.
Some morphological characteristics of primary teeth could lead to differences in fluorescence results when compared to permanent teeth, as the greater enamel porosity of the primary teeth could scatter the light more, decreasing the fluorescence values. The LF device readings may have also been influenced by several factors such as calculus, plaque and prophylactic pastes. These possible biases have been eliminated as much as possible by using strict inclusion criteria and a consistent cleaning procedure of the occlusal surfaces. The combination of visual inspection and bitewing radiography (BW) could enhance the correct diagnosis of dentin caries in permanent teeth [11]. In an in vitro study, the combination of visual inspection and bitewing radiography led to correct classification of 91% of second primary molars as being without either enamel or dentin caries [31]. However, when compared to meticulous visual inspection, bitewing radiography seems to be of limited surplus value in lesion detection when enamel caries with sound surfaces are included [32]. In the present investigation, BW showed lower sensitivity than the conventional visual criteria at the dentin level. For occlusal enamel caries detection, the BW was found to be inappropriate as it showed the lowest sensitivity. This was expected, as enamel caries lesions are very difficult to detect by radiographic examination [33]. On the D3 level, BW performed worst although not statistically different from all other methods.
The AUC confirmed the good performance of all methods in detecting either the presence or the absence of occlusal dentin caries. The conventional visual criteria and bitewing radiographs showed the lowest values. In our study, both LF devices showed the highest AUC values at the thresholds evaluated when compared to the other methods. However, this value was statistically different only from the BW AUC value (at D1), in agreement with Rodrigues et al. [11]. Barbería et al. [18] also found high values when assessing first and second primary molars in vivo. Burin et al. [34] did not find a statistical difference in AUC between LF, visual and radiographic examination.
As described earlier, the LR+ can be used to calculate the post-test odds of a test, which then become the pretest odds for a second independent test with a known LR+, resulting in the post-test probability of their combination [11, 22]. Such combinations seem to improve the process of pit-and-fissure caries detection. It is noteworthy that the calculated combinations were better when the visual methods were associated with LF and LFpen than with BW, as the former presented the highest values of post-test probability. All radiographs in children must be justified by an anticipated benefit based on new information to aid the patient’s management [35]. For occlusal caries and early caries detection, based on the results of this study, the additional benefit is greater using LF devices than using bitewing radiography. Therefore, if there is no doubt about the clinical status of approximal sites in children, radiography should be considered obsolete for occlusal caries detection and be replaced by LF [34, 35]. The LFpen consistently yielded higher post-test probabilities than LF for both detection thresholds. When LF methods were combined with VE, consistently higher post-test probabilities were achieved than in combination with ICDAS. The reason for this finding is the low intraexaminer reliability of one examiner and is discussed below.
The ICC values obtained in the present study for both intra- and interexaminer reproducibilities agree with those found by Kavvadia and Lagouvardos [15], who evaluated in vivo occlusal surfaces of primary teeth using the first LF device and found an ICC average of 0.96. Rodrigues et al. [16] compared in vitro the performance of the first LF device in permanent and primary teeth and found ICC values of 0.92 (interexaminer) and 0.91 (intraexaminer), in agreement with our results. As described above, this is the first study that evaluated the performance of the LFpen on occlusal surfaces of primary teeth. However, in occlusal surfaces of permanent teeth, high values of ICC have been reported when both LF and LFpen devices were used [11, 36, 37]. The Bland and Altman plots yielded relatively large intervals between upper and lower limits of agreement compared to former in vitro [36] and in vivo studies [38]. However, Kühnisch et al. [37] suggested that the range of LF measurements in a Bland and Altman plot should not be greater than ±20 digits (i.e., an interval of 40 digits), which was the case in the reproducibility measurements in this study. Regarding intraexaminer reliability, it is remarkable that one examiner achieved excellent kappa values with both VE and ICDAS (>0.9), while the other performed differently in the second measurement. This was due to some unavoidable personal distracting circumstances occurring during assessment. As shown in a study with four examiners using permanent teeth, weighted kappa values of 0.62–0.82 for interexaminer reliability and 0.74–0.83 can be achieved [3]. Compared to these ranges, one examiner in our study performed better and the other worse. As all “subjective” diagnostic methods can be affected by external circumstances, it is interesting that under the same level of distraction, the intraexaminer reliability scores for LF and LFpen remained equally high, as these are “objective” diagnostic methods. Good reproducibility means that both LF devices can be used for monitoring the caries process.
Reproducibility was also assessed by means of kappa values for VE, ICDAS and BW. Interexaminer reproducibility presented low values (0.23–0.35), confirming that these methods are dependent on subjective aspects such as background knowledge and individual clinical experience of the examiners involved [11, 39]. Assessing primary teeth, Rodrigues et al. [16] also found a low kappa value for interexaminer reproducibility (0.19). The difference between kappa values for intraexaminer reproducibility could exemplify the influence of subjective characteristics and clinical experience of the examiners for these examinations, as the results are very different from each other.
Moreover, a valuable feature of quantitative caries diagnostic tools is the possibility of establishing cut-off levels in order to differentiate caries penetration. However, it should be noted that there is a remarkable difference between cut-off values obtained in clinical and in laboratory settings [38]. The optimal cut-off values found in the present investigation (Table 2) were higher than those suggested by Lussi and Francescut [29], Rodrigues et al. [16] and Braga et al. [17]. These groups stored the teeth in formalin [16, 29] and saline solution [17], likely resulting in decreased fluorescence [19]. As the cut-off values obtained from this study were quite different comparing the LF devices, a question on which LF device pictures the ‘truth’ might arise. Because a variation of ±4 numerical values is inherent, the LFpen seems to be more suitable as the cut-offs and their intervals of variation are not overlapping. Therefore, it must be stressed that the cut-off values of the new LFpen device (2190) should not be confused with those suggested for the first LF device (2095). For monitoring purposes, the use of only one device is required as the readings of the LF and LFpen seem to be incompatible.
In the present study, the good performance of both LF devices in the assessment of occlusal surfaces of primary teeth was confirmed. In the literature, LF devices have been reported as an adjunct tool for caries detection. However, with respect to treatment decision LF measurements alone should never lead to a dichotomous decision regarding operative intervention. However, in combination with visual inspection LF might positively assist in the treatment decision process, which of course must also consider other aspects such as the individual caries risk and lesion activity.
Conclusions
After primary visual inspection using ICDAS or not, the use of LFpen may aid in the detection of occlusal caries in primary teeth. Bitewing radiographs may be indicated only for approximal caries detection.
References
Marthaler TM (2004) Changes in dental caries 1953–2003. Caries Res 38:173–181
Pendlebury ME, Horner K, Eaton KA (eds) (2004) Selection criteria for dental radiography. Faculty of General Dental Practice (UK), London
Jablonski-Momeni A, Stachniss V, Ricketts DN, Heinzel-Gutenbrunner M, Pieper K (2008) Reproducibility and accuracy of the ICDAS-II for detection of occlusal caries in vitro. Caries Res 42:79–87
Ricketts DN, Ekstrand KR, Kidd EA, Larsen T (2002) Relating visual and radiographic ranked scoring systems for occlusal caries detection to histological and microbiological evidence. Oper Dent 27:231–237
Ismail AI (2004) Visual and visuo-tactile detection of dental caries. J Dent Res 83 Spec No C:C56-66
Rocha RO, Ardenghi TM, Oliveira LB, Rodrigues CR, Ciamponi AL (2003) In vivo effectiveness of laser fluorescence compared to visual inspection and radiography for the detection of occlusal caries in primary teeth. Caries Res 37:437–441
Nyvad B, Machiulskiene V, Baelum V (1999) Reliability of a new caries diagnostic system differentiating between active and inactive caries lesions. Caries Res 33:252–260
Ismail AI, Sohn W, Tellez M, Amaya A, Sen A, Hasson H, Pitts NB (2007) The International Caries Detection and Assessment System (ICDAS): an integrated system for measuring dental caries. Community Dent Oral Epidemiol 35:170–178
Kühnisch J, Goddon I, Berger S, Senkel H, Bücher K, Oehme T, Hickel R, Heinrich-Weltzien R (2009) Development, methodology and potential of the new Universal Visual Scoring System (UniViSS) for caries detection and diagnosis. Int J Environ Res Public Health 6:2500–2509
Ismail AI, Sohn W, Lim S, Willem JM (2008) Progression of early carious lesions in children aged 5 years or less. Caries Res 42:226
Rodrigues JA, Hug I, Diniz MB, Lussi A (2008) Performance of fluorescence methods, radiographic examination and ICDAS II on occlusal surfaces in vitro. Caries Res 42:297–304
Diniz MB, Rodrigues JA, Hug I, Cordeiro Rde C, Lussi A (2009) Reproducibility and accuracy of the ICDAS-II for occlusal caries detection. Community Dent Oral Epidemiol 37:399–404
Lussi A, Imwinkelried S, Pitts N, Longbottom C, Reich E (1999) Performance and reproducibility of a laser fluorescence system for detection of occlusal caries in vitro. Caries Res 33:261–266
König K, Flemming G, Hibst R (1998) Laser-induced autofluorescence spectroscopy of dental caries. Cell Mol Biol (Noisy-le-grand) 44:1293–1300
Kavvadia K, Lagouvardos P (2008) Clinical performance of a diode laser fluorescence device for the detection of occlusal caries in primary teeth. Int J Paediatr Dent 18:197–204
Rodrigues JA, Diniz MB, Josgrilberg EB, Cordeiro RC (2009) In vitro comparison of laser fluorescence performance with visual examination for detection of occlusal caries in permanent and primary molars. Lasers Med Sci 24:501–506
Braga M, Nicolau J, Rodrigues CR, Imparato JC, Mendes FM (2008) Laser fluorescence device does not perform well in detection of early caries lesions in primary teeth: an in vitro study. Oral Health Prev Dent 6:165–169
Barberia E, Maroto M, Arenas M, Silva CC (2008) A clinical study of caries diagnosis with a laser fluorescence system. J Am Dent Assoc 139:572–579
Francescut P, Zimmerli B, Lussi A (2006) Influence of different storage methods on laser fluorescence values: a two-year study. Caries Res 40:181–185
Lussi A, Reich E (2005) The influence of toothpastes and prophylaxis pastes on fluorescence measurements for caries detection in vitro. Eur J Oral Sci 113:141–144
Ekstrand KR, Martignon S, Ricketts DJ, Qvist V (2007) Detection and activity assessment of primary coronal caries lesions: a methodologic study. Oper Dent 32:225–235
Lussi A, Firestone A, Schoenberg V, Hotz P, Stich H (1995) In vivo diagnosis of fissure caries using a new electrical resistance monitor. Caries Res 29:81–87
Bland JM, Altman DG (1986) Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1:307–310
Alberg AJ, Park JW, Hager BW, Brock MV, Diener-West M (2004) The use of "overall accuracy" to evaluate the validity of screening or diagnostic tests. J Gen Intern Med 19:460–465
Schulze RK, Nackat D, D'Hoedt B (2004) In vitro carious lesion detection on D-, E-, and F-speed radiographic films. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 97:529–534
Schulte AG, Wittchen A, Stachniss V, Jacquet W, Bottenberg P (2008) Approximal caries diagnosis after data import from different digital radiography systems: interobserver agreement and comparison to histological hard-tissue sections. Caries Res 42:57–61
Nair MK, Nair UP (2001) An in-vitro evaluation of Kodak Insight and Ektaspeed Plus film with a CMOS detector for natural proximal caries: ROC analysis. Caries Res 35:354–359
Kühnisch J, Berger S, Goddon I, Senkel H, Pitts N, Heinrich-Weltzien R (2008) Occlusal caries detection in permanent molars according to WHO basic methods, ICDAS II and laser fluorescence measurements. Community Dent Oral Epidemiol 36:475–484
Lussi A, Francescut P (2003) Performance of conventional and new methods for the detection of occlusal caries in deciduous teeth. Caries Res 37:2–7
Attrill DC, Ashley PF (2001) Occlusal caries detection in primary teeth: a comparison of DIAGNOdent with conventional methods. Br Dent J 190:440–443
Ketley CE, Holt RD (1993) Visual and radiographic diagnosis of occlusal caries in first permanent molars and in second primary molars. Br Dent J 174:364–370
Machiulskiene V, Nyvad B, Baelum V (1999) A comparison of clinical and radiographic caries diagnoses in posterior teeth of 12-year-old Lithuanian children. Caries Res 33:340–348
Ekstrand KR, Ricketts DN, Kidd EA (1997) Reproducibility and accuracy of three methods for assessment of demineralization depth of the occlusal surface: an in vitro examination. Caries Res 31:224–231
Burin C, Burin C, Loguercio AD, Grande RH, Reis A (2005) Occlusal caries detection: a comparison of a laser fluorescence system and conventional methods. Pediatr Dent 27:307–312
European Commission (2004) Radiation protection. European guidelines on radiation protection in dental radiology. Office for Official Publications of the European Communities, Luxembourg
Lussi A, Hellwig E (2006) Performance of a new laser fluorescence device for the detection of occlusal caries in vitro. J Dent 34:467–471
Kühnisch J, Bücher K, Henschel V, Hickel R (2007) Reproducibility of DIAGNOdent 2095 and DIAGNOdent Pen measurements: results from an in vitro study on occlusal sites. Eur J Oral Sci 115:206–211
Huth KC, Neuhaus KW, Gygax M, Bücher K, Crispin A, Paschos E, R. H, Lussi A (2008) Clinical performance of a new laser fluorescence device for detection of occlusal caries lesions at permanent molars. J Dent 35:1033–1040
Fung L, Smales R, Ngo H, Moun G (2004) Diagnostic comparison of three groups of examiners using visual and laser fluorescence methods to detect occlusal caries in vitro. Aust Dent J 49:67–71, quiz 101
Declaration of interest
The authors declare that they have no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Neuhaus, K.W., Rodrigues, J.A., Hug, I. et al. Performance of laser fluorescence devices, visual and radiographic examination for the detection of occlusal caries in primary molars. Clin Oral Invest 15, 635–641 (2011). https://doi.org/10.1007/s00784-010-0427-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-010-0427-5