
Abstract
The aim of this study was to correlate clinical and computerized tomography (CT) features of bisphosphonate-related osteonecrosis of the jaws (BRONJ). All ONJ patients for whom there was complete CT scan imaging were eligible. Selected clinical parameters retrieved from their medical records were analyzed for correlation with CT parameters. The clinical presentation of BRONJ was supported by findings in CT imaging in 78.3%. The lesion’s size on CT correlated with the presence of purulent secretion (p = 0.03). When sequestrum was present, the median lesion’s size on CT was relatively big (28 mm, range 21–43 mm). The mandibular canal cortex was never breached. CT has reasonable detection competence for diagnosing BRONJ. Purulent secretion indicates the likelihood that a more extensive involvement will be displayed on CT. A large lesion on CT should raise the index of suspicion for sequestrum. The CT appearance of a continuous cortex of the mandibular canal may serve as a differential parameter between BRONJ and metastasis to the jaw.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Osteonecrosis of the jaws (ONJ) is a devastating side effect of bisphosphonates therapy. It typically manifests as exposed bone accompanied by pain, swelling, and purulent secretions [1–7]. There are several speculations regarding the pathogenesis, but it remains unclear. Since first described in 2003 [2, 8], several hundred cases of bisphosphonate-related osteonecrosis of the jaws (BRONJ) have been published, mostly related to parenterally administered bisphosphonates, e.g., pamidronate and zoledronate [1–4]. Documentation focusing on the appearance of (BRONJ) on computerized tomography (CT) is sparse, and the available literature provides insufficient information for accurately assessing the specificity and sensitivity of CT scanning for cases of (BRONJ). Moreover, when bone exposure is not apparent, the clinical diagnosis of (BRONJ) and the determination of its severity are also difficult, as is its differentiation from other diagnoses (for example, metastasis to the jaws or localized reacutization of chronic periodontitis).
At present, panoramic radiography is the primary imaging choice followed by CT. CT scanning, however, was found to be superior to panoramic radiography as it more accurately demonstrates the lesion and its extent [9]. Bianchi et al. [9], however, recently suggested that CT scans are not always diagnostic in the early stages of (BRONJ), raising the question of the actual contribution of CT for diagnosing (BRONJ). We reasoned that the correlations between CT and clinical findings may contribute to the diagnostic process of (BRONJ) and may assist in the selection of ONJ patients for whom a CT evaluation would add important information. Our aim in the current study was to describe the CT appearance of a cohort of patients with (BRONJ) and to correlate selected clinical parameters with the CT findings.
Materials and methods
From October 2003 to August 2007, 110 bisphosphonate-treated patients with signs and symptoms of (BRONJ) were referred to the Oral Medicine and Maxillofacial Surgery Clinics of two university-affiliated medical centers in Israel (Hadassah and Sheba). In accordance with the position papers of the American Academy of Oral Medicine and the American Association of Oral and Maxillofacial Surgeons, the diagnosis of (BRONJ) was based on the medical and dental history of each patient, as well as on the observation of clinical signs and symptoms (pain, erythema, bone exposure, fistula, purulent secretion, sensory abnormality, or swelling) of this pathological process [10]. All included patients had exposed bone in the oral cavity despite 8 weeks of adequate treatment, showed no evidence of local metastasis, and had no prior radiotherapy to the affected region [11]. Another inclusion criterion was an available CT scan of the relevant jaw. These data were recorded and analyzed for all eligible patients. A periodontal probe was used to measure the longest dimension of the lesion. Selected clinical features that were noted during an early phase of the diagnostic process were matched with the CT scan findings during the same time period.
Axial CT images were obtained using various parameters. The slice thickness ranged from 1 to 2.5 mm, the mAs ranged from 40 to 400, and the kVp was 120 for all the examinations. About one quarter of the examinations was performed with intravenous contrast material, and about one third of the studies had multiplanar reconstructions. CT images were evaluated to extract the following information: lesion diameter (the radiological measurement of the largest diameter of the lesion in the axial scans), imaging characteristics of the alveolar bone (lytic/erosive, sclerotic, and mixed), presence of sequestrum, cortical discontinuity, periosteal response, structures (e.g., the cortex of the mandibular canal and maxillary sinus), and identification of any soft tissues that were involved. For uniformity of interpretation, all images were all evaluated by one neuroradiologist (JMG) who was blinded to the clinical features of each patient.
Statistical analysis
Data were analyzed using descriptive statistics. Comparisons of CT parameters for different subgroups were analyzed with the non-directional t test. Correlations between the clinical and CT parameters were analyzed using analysis of variance. Differences were considered to be significant at a p value of <0.05. The statistical analyses were performed using Statview software version 5.0.1 (StatView, SAS Institute Inc.)
Results
Patient characteristics
Thirty of the 110 patients fulfilled the inclusion criteria and were included in the analysis. Table 1 lists the demographic data, indication for and type of bisphosphonate treatment, and comorbidities. Nineteen (63%) were females, and the median age of the cohort was 67 years (range 53–83 years). The most prevalent pathologies among the patients in the cohort were hematologic malignancies [multiple myeloma (n = 11), non-Hodgkin lymphoma (n = 2), Waldenstrom macroglobulinemia (n = 1), chronic lymphocytic leukemia (n = 1) and solid cancer (n = 11)].
Bisphosphonate treatment
The three types of bisphosphonates used by the study patients were zoledronate, pamidronate, and alendronate (Table 1). One patient had undergone clodronate treatment in the past. At the onset of BRONJ, 14 patients were being treated with zoledronate (six of them had a history of pamidronate treatment), 11 were receiving pamidronate (one of them had a history of zolendronate treatment), and four patients were receiving alendronate for the treatment of osteoporosis. The median duration of bisphosphonate treatment was 3.5 years (range 8 months to 9 years).
Main complaint and relevant local history
Most patients (17/30, 57%) complained of local pain. Four patients suffered from variable types of sensory loss (dysesthesia, paresthesia) in addition to pain. All four cases of sensory loss were located at the lower jaw. Seventeen (57%) patients had a suspected triggering event, such as tooth extraction and dental implant placement. The median interval between the triggering event and the onset of (BRONJ) was 12 months (range 0–26 months; it developed immediately after dento-alveolar surgery in five patients).
Clinical presentation
The mandible was involved more often than the maxilla (24 versus 13, respectively; Table 2). The posterior segment of the jaws, i.e., molars and premolars area, was involved more often than the anterior segment, i.e., incisors and canines area (26 versus 11, respectively). Exposed bone, purulent secretion, and swelling were the predominant clinical features (Table 2). Six patients exhibited extraoral manifestations. Eight patients had multiple foci of (BRONJ) (patients 7, 8, 17, 20, 26, 27, 29, and 30), and it involved both jaws in four patients (patients 17, 20, 29, and 30).
CT evaluation
Twenty-nine lesions (in 26 patients) were observed on the CT scan compared to 37 clinically detected lesions (in 30 patients), yielding a detection level of 78.3%. The median lesion size on CT was 17.5 mm (range 0–43 mm), while the median clinically measured size was 10 mm (range 1.5–40 mm; Fig. 1). There was no significant correlation between the two measurements (p = 0.97).

Bisphosphonate-related osteonecrosis of the mandible. The patient (no. 28) underwent a dental extraction at the same site immediately before the onset of the lesion. a Clinical presentation of the bone exposure which is visible adjacent to the first premolar (arrow). b Cropped panoramic radiograph showing the lesion extending through the entire crater formed after the second premolar was extracted. c A computerized tomographic (CT) scan showing bone destruction and not fully undetached necrotic bone, which was not seen as clearly on X-ray as on the CT scan
Lesions that appeared larger on CT scans had purulent secretion and intra- or extraoral sinus tracts. There was a significant correlation between the characteristic of purulent secretion and the lesion size depicted on CT (p = 0.03). Specifically, the median size of purulent secreting lesions was 19.5 mm (range 0–41 mm) compared to median size of 15.25 mm (range 0–43 mm) for non-secreting lesions. Erythema, swelling, and pain, however, were not statistically correlated with the CT-measured lesion size.
The resolution of CT could detect lesions as small as 1 mm, but there were some “mismatches” between the clinical presentation and the CT findings. In one patient (no. 11), the site of the CT finding was a few millimeters distal to the clinically determined site. In other cases, a clinically manifested lesion was not demonstrated on CT (patients 3, 9, 17, 20, 26, 27, and 30). The lesion of patient 9 was visible on CT, but it was not detectable clinically at the same time. The radiologist reconfirmed his original CT interpretations at the end of the study, i.e., after the clinical and CT “mismatches” were revealed, and so they remained mismatches. These findings reflect the lack of statistical correlation between lesion size on CT scans and the clinical presence of bone exposure (p = 0.98).
The majority of cases affecting the bone had a mixed appearance: lysis was combined with sclerosis in 16 out of 29 bony lesions and erosion was combined with sclerosis in 3 out of 29 bony lesions. Sclerosis was often present at the periphery of the lytic focus. Only an osteolytic element, however, was visible in ten lesions: patients 2, 6, 26, 28, 29 (both lesions), and 30 had lytic lesions, and patients 7, 10, and 20 had erosive lesions. Obvious detached sequestrum with marked margins was observed on CT scans in only seven cases. These latter cases involved more extensive lesions with a median diameter of 28 mm (range 21–43 mm) compared with a median diameter of 13 mm (range 0–41 mm) in the cases with no obvious sequestrum on CT (p = 0.0006). Discontinuity of the mandibular cortex was seen in 21 out of 30 of the patients (24 out of 29 bony lesions seen on CT), and often, it involved both buccal and lingual cortexes (17 cases). The lesion damaged both the buccal and lingual cortexes in all cases where sequestrum was observed.
Periosteal reaction was observed in only 6 of 29 bony cases. None of the periosteal reactions seen on CT had the appearance of multiple horizontal layers (onion peel appearance). The periosteal reaction was in the shape of a thin smooth layer or an irregular layer of new compact bone.
None of the 24 cases involving the mandibular bone demonstrated any damage to the mandibular canal (i.e., no shifting of the canal, no encroachment of the canal, and no loss of cortex). Slight cortical sclerosis was detected in only one patient (no. 21), which is remarkable considering the massive damage to the adjacent alveolar bone. In another case (patient 13), the canal cortex was preserved and continuous but with localized areas of lower density (Fig. 2).

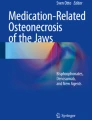
Bisphosphonate-related osteonecrosis of the mandible. The patient (no. 13) underwent dental surgery at the same site 20 months before the onset of the lesion. The lesion caused massive buccal and lingual damage to the cortex of the mandible (only lingual penetration is seen here). Note the continuity of the cortex of the mandibular canal
Of the 29 cases of ONJ displayed on CT, ten were in the maxilla and 19 were in the mandible. Perforation to nearby anatomical cavities was present in six of the former: These six perforated the maxillary sinus and two of them also perforated the nasal cavity. The destructive nature of these lesions was additionally indicated by their relatively large median diameter of 30 mm (range 4–43 mm). Mucosal swelling of the maxillary sinus mucosa was seen in only five cases. The alveolar lesion reached the maxillary sinus wall in these same five cases, while no bone formation was seen in the maxillary sinus adjacent to the alveolar lesion.
Most of the 30 CT evaluations did not use contrast material, but soft tissue changes could still be demonstrated in 14 of the 37 lesions. The sole pathology seen on the CT scan in one patient (number 11) was in the soft tissue, and her soft tissue lesions were mainly swelling. Finally, an extraoral fistula was seen on the CT scan in one case (patient 2).
Discussion
Since it was first described by Marx [2] and Wang et al. [8], (BRONJ) has become a major concern in the management of patients with multiple myeloma and bone metastases. Although bisphosphonates provide significant protection against skeletal complications and spare bone pain in these patients [10], (BRONJ) significantly reduces their oral function and quality of life. The estimated prevalence of (BRONJ) in patients treated with intravenous bisphosphonates is 4.5–12.8% for those with multiple myeloma and 1.2–12% for those with metastatic breast cancer [4, 12, 13]. These studies were performed before adequate prevention strategies for (BRONJ) were implemented. The estimated occurrence of (BRONJ) following oral bisphosphonates ranges between 0.7 per 100,000 years of use, as estimated by Merck [14], and one case per a few thousand patients as reported by two groups [15, 16]. Both intravenous and oral bisphosphonates were administered to our study patients. Since the clinical diagnostic criteria for (BRONJ) are independent of the type of bisphosphonate, the inclusion of (BRONJ) cases following oral bisphosphonate use probably did not influence the study findings.
The present bicenter study describes the CT presentation of (BRONJ) and correlates it with selected clinical features of 30 patients with (BRONJ). The CT findings matched the clinical diagnosis of (BRONJ) in 26 individuals (an approximate 78% detection level per lesion and 86% detection level per patient). Furthermore, the CT scan demonstrated the size of alveolar involvement more accurately than was clinically assumed based on the size of bone exposure, and it revealed the full extent of the alveolar lesions compared to the clinical impression of the lesion’s size in most cases (Fig. 1). These findings demonstrate that CT is an aid in the assessment of the dimensions and location of a lesion. They suggest that CT imaging may be used for definition of the lesion’s margins during its management.
In the eight cases in which clinical diagnosis of (BRONJ) was not supported with CT findings, the misdiagnosed lesion was localized to the cortex of the alveolar crest in half of the cases. These lesions were superficial and the process was in its acute early stages. In conditions such as these, the CT manifestation of a lesion is more likely to be masked by the normal thick cortex of the alveolar crest. Therefore, in cases of suspected (BRONJ) located at the periodontal papilla, it is impossible to exclude this diagnosis by CT imaging alone. During clinical follow-up, however, additional signs can be expected to develop, such as bone exposure, and thereby confirm earlier suspicions. The results of our correlations between clinical and CT findings in this study showed that purulent secretion is the only parameter for which CT indicates greater severity and a larger size of the lesion than is seen clinically. Other clinical features, such as the presence of erythema, exposed bone, swelling, or pain, are not predictive for the lesion’s actual size as seen on CT.
It is noteworthy that the cortex of the mandibular canal remained intact in all of our cases even where the adjacent alveolar bone showed lytic or sclerotic changes. The appearance of sclerotic margins around the mandibular canal in one of our patients is similar to the description in the report of Phal et al. [17]. In contrast to the resistance displayed by the cortex of the mandibular canal, the cortex of the mandible was often breached and accompanied by simultaneous perforation of buccal and lingual cortex in most cases. The sparing of the cortex of the mandibular canal was not addressed in a recent CT analysis of 32 (BRONJ) patients [9], nor did a later study describe the specific presentation of the mandibular cortex or type of mandibular canal involvement [18]. We propose that it may represent a protective feature of the mandible during the pathological bone remodeling process. Considering the recognized destructive effect of metastasis on the cortex of the mandibular canal [19], its absence in bisphosphonate-related ONJ on CT imaging may thus contribute to differentiating it from metastasis. From a clinical point of view, although the cortex of the mandibular canal was intact in all cases, sensory changes in the chin or lip were present in four of our patients, possibly indicating that mandibular nerve involvement can be present without any manifestation of mandibular canal cortex involvement on CT.
A typical formation of bone on the periosteum and on maxillary sinus mucosa whenever (BRONJ) is in proximity with the maxillary sinus was suggested in the literature [9]. We did not observe this formation among our patients, and we consider that this may be attributed to the lack of the necessary multiplanar reconstructions for all of the patients.
The current study has the usual limitations of a retrospective investigation. We believe that our data are valuable since there is only one published study on CT in (BRONJ) patients and there is no report on the application of CT as a diagnostic aid in differentiating (BRONJ) from metastasis. We recommend that this important issue be further pursued in a prospective study that compares CT representation of (BRONJ) versus CT representation of metastasis to the jaws as well as the use of contrast material for soft tissue imaging.
It is well known that dento-alveolar surgery is a triggering event for (BRONJ) [1, 20, 21]. This risk factor was also found among our patients. Therefore, it is recommended to exert special effort to avoid surgical trauma to the alveolar bone in patients who are being treated with bisphosphonates [11]. The American Association of Oral and Maxillofacial Surgeons referred to this risk factor when they suggested in their position paper that sequestrum should be removed without exposing uninvolved bone [11]. CT is a powerful tool for identifying the margins of the sequestrum. In our study, the presence and dimensions of the sequestrum, its proximity to important anatomical structures, and its margins were clearly defined whenever the lesion was observed on CT. Based on accurate information about the margins of the sequestrum, it may be removed without trauma to the adjacent alveolar bone. The added value of CT imaging to determine whether a sequestrum can be safely removed is apparent in cases where the sequestrum is large, but the window through which the alveolar bone is observed is small. In such cases, a clinical evaluation will poorly confirm that sequester is highly mobile. A comparison of the outcomes of sequestrectomy using CT imaging to the outcomes of sequestrectomy based on clinical evaluation alone that will validate the role of CT imaging in the management of (BRONJ) awaits future studies.
We demonstrated that CT may be of value in a subset of selected patients with (BRONJ), but no definitive statement on its true role is currently possible until further prospective studies are carried out. The correlations between clinical and CT findings presented in this study may assist clinicians in interpreting clinical signs of (BRONJ), especially the presence of purulent secretion. In addition, we showed that a larger lesion size on CT (median 28 mm) suggests the presence of sequestrum. Nonetheless, some cases are difficult to be diagnosed even with CT imaging, and a meticulous clinical evaluation and follow-up continue to be vital for accurate diagnosis and optimal management. Another interesting CT finding was that in (BRONJ), the mandibular canal cortex was resistant to the destructive process of the jaw, unlike in metastases. This finding may be of great diagnostic value considering the risk associated with performing a biopsy in (BRONJ) patients.
References
Ruggiero SL, Mehrotra B, Rosenberg TJ et al (2004) Osteonecrosis of the jaws associated with the use of bisphosphonates: a review of 63 cases. J Oral Maxillofac Surg 62:527–534
Marx RE (2003) Pamidronate (Aredia) and zoledronate (Zometa) induced avascular necrosis of the jaws: a growing epidemic. J Oral Maxillofac Surg 61:1115–1117
Migliorati CA, Siegel MA, Elting LS (2006) Bisphosphonate-associated osteonecrosis: a long-term complication of bisphosphonate treatment. Lancet Oncol 7:508–514
Bamias A, Kastritis E, Bamia C et al (2005) Osteonecrosis of the jaw in cancer after treatment with bisphosphonates: incidence and risk factors. J Clin Oncol 23:8580–8587
Woo SB, Hellstein JW, Kalmar JR (2006) Narrative [corrected] review: bisphosphonates and osteonecrosis of the jaws. Ann Intern Med 144:753–761
Wutzl A, Eisenmenger G, Hoffmann M et al (2006) Osteonecrosis of the jaws and bisphosphonate treatment in cancer patients. Wien Klin Wochenschr 118:473–478
Sanna G, Zampino MG, Pelosi G et al (2005) Jaw avascular bone necrosis associated with long-term use of biphosphonates. Ann Oncol 16:1207–1208
Wang J, Goodger NM, Pogrel MA (2003) Osteonecrosis of the jaws associated with cancer chemotherapy. J Oral Maxillofac Surg 61:1104–1107
Bianchi SD, Scoletta M, Cassione FB et al (2007) Computerized tomographic findings in bisphosphonate-associated osteonecrosis of the jaw in patients with cancer. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 104:249–258
Migliorati CA, Casiglia J, Epstein J et al (2005) Managing the care of patients with bisphosphonate-associated osteonecrosis: an American Academy of Oral Medicine position paper. J Am Dent Assoc 136:1658–1668
American Association of Oral and Maxillofacial Surgeons (2007) American Association of Oral and Maxillofacial Surgeons position paper on bisphosphonate-related osteonecrosis of the jaws. J Oral Maxillofac Surg 65:369–376
Durie BG, Katz M, Crowley J (2005) Osteonecrosis of the jaw and bisphosphonates. N Engl J Med 353:99–102 discussion 199–102
Hoff AO, Toth BB, Altundag K et al (2008) Frequency and risk factors associated with osteonecrosis of the jaw in cancer patients treated with intravenous bisphosphonates. J Bone Miner Res 23:826–836
American Dental Association (2006) Dental management of patients receiving oral bisphosphonate therapy: expert panel recommendations. J Am Dent Assoc 137:1144–1150
Yarom N, Yahalom R, Shoshani Y et al (2007) Osteonecrosis of the jaw induced by orally administered bisphosphonates: incidence, clinical features, predisposing factors and treatment outcome. Osteoporos Int 18:1363–1370
Mavrokokki T, Cheng A, Stein B et al (2007) Nature and frequency of bisphosphonate-associated osteonecrosis of the jaws in Australia. J Oral Maxillofac Surg 65:415–423
Phal PM, Myall RW, Assael LA et al (2007) Imaging findings of bisphosphonate-associated osteonecrosis of the jaws. AJNR Am J Neuroradiol 28:1139–1145
Bisdas S, Chambron Pinho N, Smolarz A et al (2008) Biphosphonate-induced osteonecrosis of the jaws: CT and MRI spectrum of findings in 32 patients. Clin Radiol 63:71–77
White SC, Pharoah MJ (2004) Oral radiology: principles and interpretation. Mosby, St. Louis
Marx RE, Sawatari Y, Fortin M et al (2005) Bisphosphonate-induced exposed bone (osteonecrosis/osteopetrosis) of the jaws: risk factors, recognition, prevention, and treatment. J Oral Maxillofac Surg 63:1567–1575
Badros A, Weikel D, Salama A et al (2006) Osteonecrosis of the jaw in multiple myeloma patients: clinical features and risk factors. J Clin Oncol 24:945–952
Acknowledgment
The authors thank Ms. Esther Eshkol for editorial assistance. The study was based in part on a OMD thesis of Miss Noa Ben-Ami. Dr. Noam Varom received an honorarium from Bayer Israel Ltd.
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Elad, S., Gomori, M.J., Ben-Ami, N. et al. Bisphosphonate-related osteonecrosis of the jaw: clinical correlations with computerized tomography presentation. Clin Oral Invest 14, 43–50 (2010). https://doi.org/10.1007/s00784-009-0311-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-009-0311-3