
Abstract
The aim of the present study was to investigate the association between caries frequency and body mass index (BMI) in German elementary school children. A total of 1,290 elementary school children (648 boys, 642 girls) were examined. The dental examination included the determination of caries frequency (DF-T/df-t values). The medical evaluation assessed the pupils’ general health and BMI. The study showed that 3.6% of the children were underweight, 74.8% had a normal weight, 11.9% were overweight, and 9.7% were obese. Underweight children showed natural healthy teeth in 44.7%, those with normal weight in 40.7%, whereas children with high weight and obese children showed natural healthy teeth in 30.5% and 31.7%, respectively. A significant association between high weight and caries frequency in the first dentition (p = 0.0067) and in the permanent dentition (p = 0.0002) could be observed. The association remains statistically significant after adjusting for age. The number of natural healthy teeth decreased with age (p = 0.001) and BMI (p = 0.0061) and was different between girls and boys (p = 0.0334). This study demonstrated a significant association between caries frequency and weight in school children. In future preventive programs, the importance of nutrition should not only be emphasized with respect to general diseases but also with regard to carious lesions.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
To maintain oral health, several factors such as food low in fermentable carbohydrates, oral hygiene techniques, adequate fluoride supplementation, as well as regular dental examinations have to be taken into consideration. Different national preventive programs during the last decades are responsible for a significant decrease in dental decay, particularly in children and adolescents [17, 18, 23]. Due to changed eating habits, an increase in high weight and obesity especially in developed countries has been observed over the past two decades. In 1981, about 12% of the 7- to 13-year-old children in Canada were either overweight or obese; in 1996, these values increased up to 30% [20, 25, 31].
A study of 1,585 Australian children aged between 7 and 15 years showed an increasing tendency for high weight (11–21%) and obesity (4–7%). Furthermore, an association between body mass index (BMI) and disposable income could be observed [29]. In studies with German school children, the percentage of overweight children has been established at about 15–20% [13]. A study in the USA documented that children are amongst the fastest growing group of the overweight and obese population [7]. Obesity is now one of the most common health problems in modern societies [19]. Childhood obesity may lead to serious diseases, a decrease in life expectancy and numerous other problems. A high body weight is associated with a greater risk for type 2 diabetes and might be a risk factor for cardiovascular diseases, asthma, arthritis, and general poor health [18, 24]. Being an overweight child can also cause emotional morbidity [5]. Obese adolescents are more likely to become obese adults, and obese adults have an increased risk of morbidity and mortality in adulthood [9]. Changes in eating habits, a lack of activity, and less exercise as well as social changes are thought to be responsible for this new epidemic [4]. Overweight people have a greater need of medications [5], and several studies were able to prove that BMI correlated positively with the number of doctors’ appointments and medications, but negatively with preventive measures and preventive medical checkups [28]. It has been proposed that obesity prevention should start as early as possible and that prevention in infants may be the most effective preventive measure for adult obesity. Of equal importance are the negative social and physiological ramifications of childhood obesity, such as being rejected by peers and being the victims of various forms of peer aggression like bullying [12, 21]. To our knowledge, the association between weight, BMI, and dental health has not been examined in children although similar risk factors, such as a one-sided diet, e.g. a diet high in sugar, may play a role in the development of these characteristics.
The objective of this study was to examine a possible relationship between the presence of caries lesions and BMI in elementary school children by taking into account other factors such as age and sex.
Materials and methods
This study was conducted in cooperation between the dental hospital and the Department of Pediatrics of the Johannes Gutenberg—University of Mainz as well as with the Association of Dental Health of the State of Rhineland Palatinate. A total of 1,298 children were examined at the dental hospital. For this analysis, only children aged between 6 and 11 years were considered. These dental assessments were made mandatory, and the parents were encouraged to give their written consent; less than 5% of the parents refused to give this permission. Data from 1,290 children (648 boys and 642 girls) from five elementary schools from different social backgrounds in a medium sized German city (about 220,000 habitants) were available for this study. The dental and physical examinations of the children were only conducted with the written consent of the parents and/or guardian.
The dental examination (performed by eight calibrated dentists of the Department of Operative Dentistry, University Mainz) was non-invasive (mirror, dental probe, cotton roll), included optimal illumination of the oral cavity, and the determination of visual caries as no X-rays were used. Before the dental examination, the children were instructed to clean their teeth as usual. Cavities and significant discolorations around the restorations were designated as carious lesions.
In addition to the dental examination, the children were questioned about their dietary habits, the daily consumption of sweets and beverages. The documentation of the oral health was anonymous and, therefore, recorded on special forms, including number of teeth, caries frequency, age of the children, school grade, and gender. Decayed deciduous teeth, and permanent teeth that were in need of treatment, were marked as cavities. Teeth with fissure sealants were separately recorded as having received prophylactic treatment. If restoration materials were present, the teeth were marked as sufficiently or insufficiently treated. Missing teeth were not specially marked, as no definite statement could be made without a proper dental history.
Due to being a dental mass screening and on account of missing indication criteria, no X-rays were taken. To assess the caries frequency, the DF-T value for the permanent dentition and the df-t value for the primary dentition were used [14]. The examination always referred to the respective tooth (DF-T/df-t value), not to an individual tooth surface (DF-S/df-s value). Other relevant clinical data, like the regular development of the children, the deviation in growth, and BMI, were recorded by qualified physicians of the Department of Pediatrics. The height of the children was measured with a portable measuring unit. The weight was established with a portable digital scale, and the weight was always rounded off to the nearest 100-gram value. BMI (=body weight/body height2, in kg/m2) was used. The internationally recognized classification of BMI with low weight, normal weight, high weight, and obesity was conducted with special tables from the obesity consortium for children and adolescents [1].
Data analysis
The statistical analysis of this cross-sectional data was performed with the software SAS (version 8.2; Statistical Analysis Systems, North Carolina, USA). Frequency distributions of DF-T- and df-t index and BMI are presented. The association between age and BMI is illustrated using box plots. In the box plots, the central line marks the median, box outlines present the quartile range and whiskers the range 1.5-fold of the quartiles, dots present outliers and asterisk extreme outliers. Children were classified according to BMI into categories, such as “underweight”, “normal weight”, “high weight”, and “obesity”; df-t and DF-T values were treated as continuous variables. Additionally, we used the binary variable “natural healthy teeth” defined as neither no caries nor fillings. The frequency of caries between subgroups was compared using the t-test. For the binary variable “natural healthy teeth”, a logistic regression model was used to investigate whether age, BMI, and gender are independent risk factors. The influence of age, BMI, and gender on the number of df-t and DF-T was investigated by analysis of variance.
Results
The examination of elementary school children in a German city included 1,290 pupils. The gender distribution was even, with 50.2% boys and 49.8% girls, and the age ranged from 6 to 11 years. One hundred sixty-three children (70 boys, 93 girls) were 6 years of age, 356 children (185 boys, 171 girls) were 7 years of age, 308 children (158 boys, 150 girls) were 8 years, 274 children (137 boys, 137 girls) were 9 years old, 175 children (91 boys, 84 girls) were 10 years, and 14 children (7 boys and 7 girls) had the age of 11 years. The distribution of the children according to age, gender, and BMI is given in Table 1. The dental examination showed that only 38.6% of the children (boys, 35%; girls, 41%) were caries-free, without decayed or filled teeth, and there was a significant difference between the genders (p = 0.0211). Teeth with fissure sealants were present in 16% of the children; 87% of the fissure sealants were intact, 6.4% displayed discolorations, and in 6.6%, the sealant was partially lost, but the dental hard tissue was still sound. The boys showed a mean of 2.11 carious lesions (df-t values) in the first dentition and of 0.59 in the permanent dentition (DF-T values). The girls showed a mean df-t value of 1.71 and mean DF-T values of 0.57. There is a remarkable, even not surprising, trend in the caries frequency: 53% of 6-year-old children had natural healthy teeth; this number decreased to 42% in the 7-year-old children, to 39% in 8-year-old children, 32% in 9-year-old children, 30% in 10-year-old children, and was as low as 14% of children at the age of 11 years, showing an increase of about 10% per year. It was found that the number of healthy teeth decreased clearly with increasing age (p = 0.001). The daily consumption of sweets showed a significant correlation to caries frequency (p = 0.0001). Twenty-five percent of the children reported to eat sweets several times per day (mean df-t/DF-T values = 4.81), 44% stated to eat something sweet once per day (mean df-t/DF-T values = 2.81), and 31% of the children reported to eat sweets rarely or very rarely (mean df-t/DF-T values = 1.32).
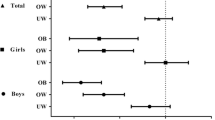
Figure 1 demonstrates the distribution of natural healthy teeth in the group of boys and girls. Only 3.6% of the children in the study (n = 47; 26 boys and 21 girls) were underweight, 74.7% (n = 964; 485 boys and 479 girls) of the children were of normal weight, 11.9% (n = 153; 73 boys and 80 girls) of the children were overweight, and obesity was present in 9.8% (n = 126; 64 boys and 62 girls) of the children. No significant gender differences could be observed. Figure 2 shows the increasing relation between the age of the children and the BMI value. When looking at the BMI value, 44.7% of the underweight children had natural healthy teeth, 40.7% of the children with normal weight had healthy teeth, whereas only 31% of the overweight children and 31.7% of the obese children showed healthy dentitions.

Prevalence of natural healthy teeth (primary and permanent dentition) among elementary school children regarding the different age groups (6-year-old: 163 children; 7-year-old: 356 children; 8-year-old: 308 children; 9-year-old: 274 children; 10-year-old: 175 children; 11-year-old: 14 children)

Distribution of BMI and age of the children
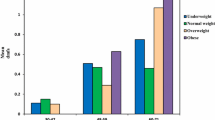
Figure 3 shows the distribution of boys and girls with natural healthy teeth into different weight classes. There was a statistically significant association between natural healthy teeth and BMI (p = 0.001). Multivariate analysis demonstrates that age (p ≤ 0.01), BMI (p ≤ 0.01), and gender (p ≤ 0.05) are independent risk factors. Estimated odds ratio for age is 1.27 (per year), and this value did not change substantially after adjusting for age and gender. Similarly, BMI is associated with carious frequency in the first dentition (df-t values) as well as in the permanent dentition (DF-T values). Although underweight children showed a mean DF-T value of 0.38 (mean df-t = 1.43), children with normal weight had a mean DF-T value of 0.53 (mean df-t = 1.82), overweight children had a mean DF-T value of 0.85 (mean df-t = 2.3), and obese children had a mean DF-T value of 0.82 (mean df-t = 2.2). The gender differences of the frequency of caries lesions in relation to BMI resulted in a slightly higher occurrence of caries lesions in boys (Table 1).

Distribution of healthy teeth in the elementary school children and age-related low weight, normal weight, high weight, and obesity
Discussion
The prevalence of obesity and severe obesity continues to increase rapidly, implying that both obesity-associated co-morbidity and mortality will rise accordingly [6, 8]. The significant, important determinants of quality of life include oral health and healthy teeth [22], as oral changes and/or disorders can result in physical as well as psychological problems. Given the increased health risks associated with obesity, those people should consult their physician regularly [32]. There is some evidence that an impaired dentition can affect individuals by causing dietary restrictions via difficulty in chewing, possibly compromising their nutritional status and well-being [10, 18].
A number of studies have considered the risk factors contributing to the prevalence of high weight in children and adolescence. The literature reports a range of different indicators, e.g. income, education levels and occupation, high weight of parents, and life style, as being suitable measures of the social status [26, 27, 29]. A study in Estonia, Finland, and Lithuania showed that approximately half of the adult population was either overweight or obese. The authors found that obesity significantly correlated with little or no exercise and the education level especially in women [15]. When looking at childhood obesity, other parameters such as the socioeconomic position of the parents must be regarded [4, 30]. Danielzik et al. [3] showed that a child is more likely to become overweight if the parents are overweight and/or obese, and therefore, the familial disposition has to be taken into account regarding further preventive programs. One of the main risks of obesity in childhood is that it will probably continue into adulthood with all the associated health risks. In Germany, a great increase in childhood obesity could be observed after the country’s reunification [16].
In a study of Kalies et al. [13], the prevalence of overweight and obesity in pre-school children (5 and 6 years old) in Bavaria, Germany, was examined. The prevalence of overweight/obesity for both sexes increased from 8.5/1.8% in 1982 to 12.3/2.8% in 1997. The study of Heude et al. [11] in France with 5- to 12-year olds showed that, over a period of 8 years (1992–2000), there was an increase in height and BMI in both boys and girls. In girls, e.g. obesity increased from 1.6 to 4.4% and overweight from 14.1 to 18.6%. In this study, a total of 1,290 elementary school children were enrolled to reexamine the relationship between dental caries and high weight. Underweight children showed in 44.7% natural healthy teeth, 40.7% of the children with normal weight had healthy teeth, whereas only 31% of the overweight children, and 31.7% of the obese children showed healthy dentitions. The distribution of the caries frequency of the pupils from the present study was comparable with data from other German states. In this study, 53% of the 6-year-old children were caries-free and, in the study of Pieper [22], was shown for the year 2004 that 54% of the 6- to 7-year-old children from Rhineland Palatinate and 50.1% of the 6- to 7-year-old children in Germany were caries-free.
In a study of Chen et al. [2] in Taiwan, 3-year-old children were examined for decayed and missing teeth (df-t), and BMI was evaluated. The authors found that the prevalence of dental caries was not significantly different among the BMI groups. These results may deviate from our study because the children were only 3 years old. At this age, there is still a major parental control over the diet—especially in consideration of modern convenience food—and over the oral hygiene techniques. Furthermore, at that age, the influence of peers is limited or non-existent.
The results of this study indicate a possible association of high weight and caries. Besides numerous other risk factors, high weight can also be made responsible for an increased number of carious lesions. Certainly, high weight is not per se an etiological factor for the caries process. In future preventive programs, the strategies should aim a nutrition control to avoid high weight as well as caries, including meal frequency control and reduction in fermentable carbon hydrates.
References
Arbeitsgemeinschaft Adipositas im Kindes-und Jugendalter der Deutschen Adipositas Gesellschaft, Leitlinien vom 04.10.2002
Chen W, Chen P, Chen SC, Shih WT, Hu HC (1998) Lack of association between obesity and dental caries in three-year old children. Zhonghua Minguo Xiaoer Keyi Xuehui Zazhi 38:109–111
Danielzik S, Langnäse K, Mast M, Spetmann C, Müller MJ (2002) Impact of parental BMI on the manifestation of overweight 5–7 year old children. Eur J Nutr 41:132–138
De Spiegelaere M, Dramaix M, Hennert P (1998) The influence of socioeconomic status on the incidence and evolution of obesity during early adolescence. Int J Obes 22:268–274
Dietz WH, Robinson TN (1998) Use of the body mass index (BMI) as a measure of overweight in children and adolescents. J Pediatr 132:191–193
Fiscella K (1999) Is lower income associated with greater biopsychosocial morbidity? Implications for physicians working with underserved patients. J Fam Pract 48:372–377
Flegal KM, Troiano RP (2000) Changes in the distribution of body mass index of adults and children in the US population. Int J Obes Relat Metab Disord 24:807–818
Fontaine KR, Bartlett SJ (2000) Access and use of medical care among obese persons. Obes Res 8:403–406
Freedman DS, Khan LK, Dietz WH, Srinivasan SR, Berebson GS (2001) Relationship of childhood obesity to coronary heart disease risk factors in adulthood: the Bogalusa heart Study. Pediatrics 108:712–718
Hollister MC, Weintraub JA (1993) The association of oral status with systemic health, quality of life, and economic productivity. J Dent Educ 57:901–911
Heude B, Lafay L, Borys JM (2003) Time trend in high, weight, and obesity prevalence in school children from Northern France, 1992–2000. Diabetes Metab 29:235–240
Janssen IJ, Craig WM, Boyce WF, Pickett W (2004) Associations between overweight and obesity with bullying behaviours in school-aged children. Pediatrics 113:1187–1194
Kalies H, Lenz J, von Kries R (2002) Prevalence of overweight and obesity and trends in body mass index in German pre-school children, 1982–1997. Int J Obes Relat Metab Disord 26:1211–1217
Klein H, Palmer CE, Knutson JW (1938) Studies in dental caries. I. Dental status and dental needs of elementary school children. Public Health Rep 53:751
Klumbiene J, Petkeviciene J, Heasoja V, Prättäla R, Kasmel A (2004) Sociodemographic and health behaviour factors associated with obesity in adult populations in Estonia, Finland and Lithuania. Eur J Public Health 14:390–394
Kromeyer-Hauschild Jaeger U (1998) Growth studies in Jena, Germany: changes in body size and subcutaneous fat distribution between 1975 and 1995. Am J Human Biol 10:579–587
Locker D (1988) Measuring oral health: a conceptual framework. Community Dent Health 5:3–18
Marcenes W, Steele JG, Sheiham A, Walls AWG (2003) The relationship between dental status, food selection, nutrient intake, nutritional status, and body mass index in older people. Cad Saúde Pública, Rio de Janeiro 19:809–916
Mokdad AH, Ford ES, Bowman BA (2003) Prevalence of obesity, diabetes, and obesity-related health risk factors. JAMA 289:76–79
Ogden CL, Flegal KM, Carroll MD, Johnson CL (2002) Prevalence and trends in overweight among US children and adolescents 1999–2000. JAMA 288:1728–1732
Pearce MJ, Boergers J, Prinstein MJ (2002) Adolescent obesity, overt and relational peer victimization, and romantic relationships. Obes Res 10:386–393
Pieper K (2005) Epidemiologische Begleituntersuchung zur Gruppenprophylaxe 2004. Dtsch Arbeitsgemeinschaft für Jugendzahnpflege e. V, Bonn
Reisine ST, Locker D (1995) Social, psychological and economic impacts of oral conditions and treatments. In: Cohen LK, Gift HC (eds) Disease prevention and oral health promotion. Socio-dental sciences in action. Munksgaard, Copenhagen, pp 33–71
Sinha R, Fisch G, Teague B (2002) Prevalence of impaired glucose tolerance among children and adolescents with marked obesity. N Engl J Med 246:802–810
Tremblay MS, Katzmarzyk PT, Willms JD (2002) Temporal trends in overweight and obesity in Canada, 1981–1996. Int J Obes Relat Metab Disord 26:538–543
Troiano RP, Flegal KM, Kuczmarski RJ, Campbell SM, Johnson CL (1995) Overweight prevalence and trends for children and adolescents: the National Health and Nutrition Examination Surveys, 1963–1991. Arch Pediatr Adolesc Med 149:1085–1901
Turrell G, Western JS, Najman JM (1994) The measurement of social class in health research: problems and prospects. In: Waddell C, Petersen AR (eds) Just health: inequality in illness, care and prevention. Churchill Livingstone, Melbourne, pp 87–103
Twetman S, Garcia-Godoy F, Goepferd SJ (2000) Infant oral health. Dent Clin North Am 44:487
Wang Z, Patterson CM, Hills AP (2002) Association between overweight or obesity and household income and parental body mass index in Australian youth. Analysis of the Australian National Nutrition Survey, 1995. Asia Pac J Clin Nutr 11:200–205
Whitaker R, Wright JA, Pape MS, Seidel KD, Dietz WH (1997) Predicting obesity in young adulthood from childhood and parental obesity. N Engl J Med 337:869–873
WHO (2000) Obesity-preventing and managing the global epidemic. Report of a WHO consulting on obesity. WHO Technical Report Series 894
Zayat EN, Fontaine KR, Cheskin LJ (1999) Use of preventive health care services by patients with obesity. Obes Res 7:223–226
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Willerhausen, B., Blettner, M., Kasaj, A. et al. Association between body mass index and dental health in 1,290 children of elementary schools in a German city. Clin Oral Invest 11, 195–200 (2007). https://doi.org/10.1007/s00784-007-0103-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00784-007-0103-6