
Abstract
Fall risk and fall-related injuries increase with age. With an aging population, we need to have a better understanding of what solutions can help us cope with age-related falls. Ambient and ubiquitous fall technologies engage a large research community. We wanted to map research that has been done, technology that is developed and/or applied, current major research topics, and the current knowledge gaps. We employed the systematic mapping study approach. We searched systematically for available literature where modern ICT was developed or applied. A total of 1017 relevant abstracts were analyzed based on a number of criteria such as type of intervention (e.g., fall detection), type of technology (e.g., accelerometers), type of research contributions (e.g., proof of concepts, field trial results), focus of the solution (e.g., accuracy, privacy) etc. Our findings show that existing research is largely in a proof-of-concept phase. A large variety of technology is used. Component requirements are in focus, while system requirements related to real-world deployment are seldom addressed. The focus is on monitoring and data collection, while systems for empowering users are less frequent. Fall detection is by far the largest intervention type, while preventive interventions are less frequent. We have four recommendations based on our findings: (1) more research is needed to develop ICT-based preventive and corrective interventions; (2) more research is needed to develop ICT for empowering users; (3) more research is needed to integrate component technologies into future deployable service models; and (4) more research is needed to evaluate solutions in real-world settings.
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
1 Introduction
This paper is about age-related falls and the role that modern ICT—including pervasive and ubiquitous technology—plays in addressing the problem of falls. Age-related falls are undesirable falls that potentially lead to injuries and other physical and psychological consequences for the faller. Falls are commonly defined as “inadvertently coming to rest on the ground, floor or other lower level, excluding intentional change in position to rest in furniture, wall or other objects” [1]. Another common definition used by, e.g., the American Geriatrics Society and British Geriatrics Society, is “A fall is an unexpected event in which the participant comes to rest on the ground, floor or lower level without known loss of consciousness” [2].
Falls are more common—and consequences more sever—among seniors above 65. According to the “World Health Organization global report on falls prevention in older age,” approximately 28–35 % of people aged 65 and above fall each year, increasing to 32–42 % for those over 70 years of age. More than 50 % of injury-related hospitalizations among people older than 65 are related to falls. This makes falls the second leading cause of accidental or unintentional injury deaths worldwide. Fall mortality among men age 65 and older in USA is 46.2 per 100,000, increasing to 153.2 in age 85 and older. Similar numbers apply to many European countries [1]. Scandinavian countries are at the top of the statistics—Oslo had almost 200 hip fractures per 10,000 inhabitants in 1996–1997, compared to around 110 in USA [3]. Worldwide, death rates from falls have increased by 50 % during the last decade [4]. Incidences of some fall injuries that are common among seniors—such as fractures and spinal cord injuries—have increased by 131 % during the last three decades [1]. There is no doubt that falls pose a major burden on both those who fall and the healthcare systems in many countries. If preventive measures are not taken in the immediate future, the numbers of injuries caused by falls is projected to rise sharply with an aging population.
ICT is proposed by many as a solution to addressing the challenge of an aging population [5]. For this reason, funding has been channeled into research and innovation projects that try to understand how ICT can help support independent living. Age-related falls is one of the major research and innovation areas within independent living (at the time of writing we identified seven EU-funded R&D projects on the topic of falls). Falls are interesting from a pervasive and ubiquitous technology perspective. Falls are by nature physical and embodied in physical environments. Pervasive and ubiquitous technologies are traditionally concerned with bringing the computers “out of the box” and integrating them into the user’s physical environment [6, 7]. This is also what we see as common in the ICT research related to falls: mobile, wearable, or embedded devices that follow the users as they move about in the physical world. One could argue that age-related falls is one of the areas where pervasive and ubiquitous technologies can make the greatest societal impact.
In order to contribute to this impact, we have done a systematic mapping of the literature related to ICT and age-related falls. A systematic mapping is a process to analyze the properties of the research papers in a research field. Our goal has been to provide a map of the research that is being done, and in this way to provide the basis for a reflection process among the researchers in this field. In what follows we will first describe why we have used the systematic mapping approach and why we need a mapping of the research in the first place. Next, we describe the research questions we have used in our study. We then describe our data sources and our inclusion and exclusion criteria for the systematic search and screening of the papers we have found. Our coding, classification scheme and the findings are then presented. Finally, we will sum up our major findings in the discussion chapter and conclude with a set of recommendations that we hope will contribute to a more informed research agenda in this field.
2 Method: systematic mapping
For our literature mapping we have used a method called systematic mapping [8, 9]. Systematic mapping is a survey method used for the analysis of published literature in a wide research area. A systematic mapping study (SMS) is different in its aim than the more well-known systematic literature review (SLR) [10]. This difference is illustrated in Fig. 1. An SLR is an in-depth study of a narrow area using specific and pointed research questions. The aim of an SLR is to create new knowledge through a meta-analysis of existing knowledge published in the literature. SLRs use methodological quality as inclusion criteria when searching for and including literature. An SMS uses the same basic methodology for searching and analyzing literature as in a SLR. An SMS, on the other hand, aims at creating a map of a wide research field. Methodological rigor in the primary studies is not of importance for an SMS. An SMS can answer high-level research questions such as: “What are the main areas of research within age-related falls?”; “What are the types of papers being published in the area?” The knowledge created by an SMS can be used as the basis for further research [9], for instance, as a pre-study for one or several SLRs in specific areas. An SMS can also be used to identify gaps in knowledge and inform research funding policies [11]. In this way, SMS is more of a policy making and strategic research tool, while SLRs create new empirical knowledge.

Systematic literature reviews are concerned with depth, while systematic mapping studies are concerned with covering a wide field
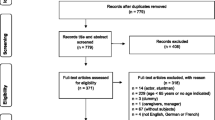
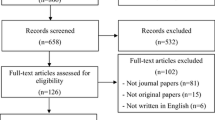
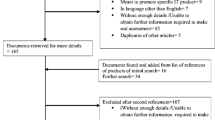
Figure 2 shows the steps involved in a typical mapping study as described in [8] and adapted in this paper with number of search results shown for each step. The top row of rounded boxes denotes the steps involved in the process, while the lower row denotes the outcomes from each step. The study starts with a definition of the research question(s) that define the scope of the study. Search for papers and screening of papers based on inclusion and exclusion criteria result in a set of relevant papers. The abstracts of these papers are then analyzed through a coding (categorization) process. This coding process results in a classification scheme which is then used in a mapping and visualization process leading to the systematic map of the research field. Our study has followed all these steps. The steps and the outcomes are documented in the rest of this paper.

Steps and outcomes in a systematic mapping study. Adapted from [8]
2.1 The need for this mapping study
We believe there is a need for a mapping study in the area of ICT addressing age-related falls. The research field has grown and produces hundreds of publications each year (approximately 250 articles in 2012 found in our searches). We need to see what is being researched on and where knowledge gaps are. At the same time, from our own experience working with ICT and independent living in Norway, we do not see many examples of this type of technology being deployed as part of healthcare services. We naturally ask ourselves why, whether enough research funding is being spent on real-world trials, and how we can improve the impact of this research on practitioners. How can ICT be better connected to the clinical practices of preventing age-related falls? Although the main target for our study is researchers working in this field, we believe the results are also of importance for research funding agencies and policy makers [12].
We have not found any other SMS published in this topic. However, there is a growing number of SLRs that we knew of beforehand or we discovered during our search. Table 1 provides for an overview of some of these SLRs. These studies answer some very important research questions and collectively offer some indications of the overall picture. These SLRs have also helped shape our understanding of the field and in forming the research questions for our SMS. Our mapping study provides additional macro-level knowledge about the field, such as which phases of movement impairment gets more attention, and what is the overall distribution of evidence, as will be described later.
3 Definition of research questions
In this section we first provide a more in-depth analysis of the problem of age-related falls. We then sketch a model of age-related falls we have developed to frame and scope the study and to guide the coding process. At the end of the section, we will introduce the research questions that we have addressed in our study.
3.1 Age-related movement impairment and falls
As part of the natural aging process, our bodies undergo a number of physiological and biomechanical changes. Although these changes are a natural part of the aging process, they also lead to different types of movement impairment [21]. As we age, our joint flexibility decreases considerably, making it difficult to move smoothly and switch among different postures. Our muscle mass is reduced, which leads to reduction in strength and force control, problems with balance, and gait disorders [22]. In addition, decline in our cognitive abilities as a consequence of aging reduces our ability to perform complex and coordinated physical movements, to learn new physical skills, and to switch quickly between physical tasks [23]. We use a longer time to plan and initiate complex movements. Increased tremor reduces our body’s fine movements and control of muscles [24]. Gradually, our ability to perform many fine motor activities of daily life declines. Consequently, movements such as pointing, reaching, and grasping—all of which require the ability to balance and stabilize posture in order to perform [25]—are affected.
Although movement impairment is a natural process that occurs as part of the aging process, the sum of these factors contributes to turning this process into a hinder for independent living. Loss of mobility is one of the biggest challenges facing an aging population [21]. Independent living and self-management are heavily dependent on the senior person’s ability to move freely, perform a set of activities of daily life, and live without fear of falling [21, 26]. With the increasingly aging population and the increase in the number of the very old, frailty becomes a major challenge. Somewhere between a quarter and half of people older than 85 years are estimated to be frail, with substantial risk of falling and disabilities [26].
As part of the aging process, the consequences of falling also increase due to, e.g., skeletal fragility. The bone mass reduction process (called osteoporosis) amplifies the consequences of falling–especially among women [27]. Bone mass reduction process increases rapidly with increased age. Skeletal fragility can also be caused by other age-related causes, e.g., decreased ability of bones to resist a crack [23, 27]. Consequences of falling for elderly include injury, hospitalization, premature death, loss of independence, social isolation, increased fear of falling, and serious hip and other fractures [1]. Hip fractures are one of the most costly types of fractures among seniors, psychologically, socially, and economically for the society. In Norway, each year we witness approximately 9000 hip fractures, almost one every hour [28].
3.2 Using technology to cope with movement impairment
Due to their being a major societal burden, falls attract large amounts of research funding. Both quantitative and qualitative strategies are used to generate knowledge about the nature of falls and the impact of various preventive actions. Clinical research focuses on the effect of various fall prevention and risk assessment interventions. Social scientists try to understand the consequences of falls and fear of falling on the involved people, including fallers but also their formal and informal caregivers. In the recent years, also a large number of researchers from computer sciences and related fields have been involved in addressing falls from a technological perspective. Understanding and addressing falls among seniors has become a truly multidisciplinary research area.
Our interest is mainly related to the role that ICT, especially modern pervasive and ubiquitous technologies, plays in this vast research field. In this paper we pose the overall research question: What role does modern ICT and ICT-related research play in addressing the problem of age-related falls? As a framework to attack this problem we have adopted a lifetime model of age-related falls, as shown in Fig. 3. This model is based on the progression of movement impairment as a consequence of aging, as discussed in the previous section. The arrow in the figure denotes the aging process, active community-dwelling seniors to the left and frail seniors to the right. The lines inside the arrow show examples of intervention types where ICT-based solutions have been applied. These interventions are relevant for specific age groups. Preventive interventions are normally useful before the first serious fall that leads to hospitalization and potential fractures. ICT-based solutions to support preventive interventions include educational portals and applications, applications to promote physical activity, applications to support exercises (e.g. gamified exercises using game consoles), and various ICT-based risk assessment tools. ICT research in fall detection focuses mainly on falls sensors, wearable or embedded in the user’s environment, and associated algorithms for accurate detection of falls. Mechanical and physical devices, such as hip protectors, have been used to prevent injuries. Typical solutions in the rehabilitation phase include exercise-related applications.

A lifetime model of movement impairment and ICT-based interventions used as the framework for the mapping of the literature
3.3 Research questions
Based on this lifetime model of movement impairment, and at the same time focusing on age-related falls as the phenomenon under study, we have addressed the following research questions:
-
In which phases of the movement impairment process is ICT used? What types of interventions are reported? What is the distribution of research efforts among the various phases and types of interventions?
-
What types of technology, components and systems are being developed and used in each phase? e.g., sensors, devices, information systems.
-
What properties of ICT systems are most central? e.g., functionality, security, interoperability.
-
What types of settings are these technologies used in? e.g., home, nursing home, hospitals.
-
What types of research are published in the field? e.g., concept design papers, field trials, expert opinions. What is the distribution among these types of research?
-
What portion of this research in focused on documenting real-world effects?
4 Data sources and search queries
Table 2 shows our search query. The first column lists common terms used for the type of intervention, corresponding to the phases in the lifetime model described above. The population column uses some common terms to describe seniors. The technology part is the most extensive one and consists of two types of queries, one at the system level and one at the component level.
The content of each column was put together into a sub-query using the OR logical operator. The four sub-queries from each column were then combined into the final query using the AND logical operation.
We have searched only in titles and abstracts. The search was done iteratively where we observed results from initial pilot searches and added new terms that were observed in search results into Table 2. We searched in a number of databases as shown in the Table 3. In total, we had 5754 hits. This was reduced to 4545 after duplicate removal. Duplicate removal was done automatically in the bibliography software (EndNote) by comparing author name, title and year of publication.
5 Screening of papers
After the duplicates were removed, we had a manual screening process where we used the inclusion and exclusion criteria listed in Table 4. The screening was done by Author A and Author B in parallel, each author independently screening all the 4545 papers. We had a consensus meeting afterward where we compared our results. Only papers that were included by both authors were included in the further analysis. In total, 1017 papers were included by both authors.
We did not include research quality aspects of the papers, such as whether they reported empirical data, in inclusion or exclusion criteria (which is a common criterion in SLRs). Our goal is not to evaluate the quality of individual papers but to evaluate the research field as a whole.
6 Results from coding and our findings from the data
We adapted the process described in [8] to code the abstracts and to create a classification scheme. The coding was done as a combination of top-down and bottom-up processes. We were not sure how much information the abstracts contained so we had a number of small iterations where we let the text in the abstracts guide the coding. We then tried to combine the keywords and align them with the research questions in order to create a scheme for further coding. The final coding includes the following dimensions:
-
Type of technology used, e.g., software, hardware, sensor, camera.
-
Form factor of the technology, e.g., ambient, wearable, portable.
-
Areas of intervention e.g., fall prevention, fall detection.
-
Intended usage setting e.g., home, hospital.
-
Research contributions e.g., concept design, field evaluation.
The following sections document our data and our findings. You will find a main graph for each major categorization dimension. In addition, for each of these main dimensions you will also see a number of combination graphs where combined categories are interesting to investigate (e.g., type of technology per intervention).
A note to the reader: The main graphs that follow are designed to show trends by dividing the abstracts into yearly intervals. We have decided to limit these graphs to show the period 2008–2013 in order to avoid overcrowded graphs. However, our search results include both older papers and some papers from 2014 (see Fig. 4). These total numbers are shown in parentheses (e.g., n = 122) in the text that describes the main graphs. You will therefore notice that the numbers in parentheses are sometimes higher than those shown in the main graph for the same categories.

Type and number of publications per year
6.1 Bibliographic data
This section provides some data about the type of the publications, the year of the publication, and most used publication channels. The complete database including all 1017 citations in RIS format can be downloaded here [29].
Figure 4 shows the type and number of publications per year. We included journals (n = 377), conferences (n = 615), magazines/serials (n = 22), theses (n = 2), and book sections (n = 1). The lower number of publications in 2013 is most probably due to the fact that our search was done in the end of 2013, which is too early for all 2013 papers to be indexed in the databases.
Some of the most popular journals and conferences are shown in Table 5. These numbers are based on data automatically collected from the search engines. The table shows only a small selection of all the journals and conferences in our database. Our data also show a large number of unknown values (n = 510 for conferences and n = 208 for journals). We have not made any effort to classify sources manually.
6.2 Technology
We coded the abstracts for the characteristics of the technology reported. One type of coding was done to classify the type of technology, e.g., an accelerometer device or a smart wheelchair. Additionally, we coded based on technology form factor, e.g., if it is wearable or embedded in the physical environment.
6.2.1 Type of technology
We divided technology roughly into hardware oriented and software oriented (see Fig. 5). Within the hardware-oriented group, we coded abstracts into three main categories: sensor technology (for monitoring), actuator technology (for interacting with user and making changes in the environment), and computer networks (for data communication). Within the software-oriented group, we ended with three major groups: algorithms (mostly used in conjunction with sensors to process sensor data), information systems, and middleware (targeting developers of technology).

Types of technology. We have made a rough division into hardware-oriented technologies (three columns to the left) and software-oriented technologies (the three columns to the right)
We defined actuator technology to be any technology that is designed primarily to interact with the user. This group includes various game consoles used for interactive games, smart canes, walkers, walking aids, dance pads, robots, and wearable devices that are used for, e.g., force feedback. On the other hand, sensors are defined to denote technology that is developed for monitoring, with little or no user involvement. The information system category includes electronic patient records, geographic IS, telecare, Web services, administrative software, data analysis software and other software that demonstrates holistic system/service thinking beyond component technology.
One general finding related to technology is the sheer number and variety of technology used. This might not come as a surprise since we had a large scope to begin with. For instance, we found more than 30 types of sensors ranging from accelerometers (the most popular), to radars, laser scanners, and thermal sensors. We also found a wide variety of software algorithms ranging from Bayesian networks to Markov chains and neural networks.
As shown in Fig. 5, the large majority of the abstracts discuss some form of sensor technology. Algorithms are very common and are often used to process data from sensors. Actuator technology is far less common. The same is true for information systems. Some abstracts focused on the network technology used, such as body area networks, ZigBee, and Bluetooth.
6.2.2 Technology form factor
We coded the abstracts based on what we call form factor. Form factor is the aspect of technology that is most visible for the end user, and likely to have large impact on user acceptance [30].
We identified four major form factor types (Fig. 6). Ambient technologies are those that are integrated in the lived physical environment. The largest group of ambient technologies is fixed cameras (approximately n = 106). These are normally used for activity recognition and detection of abnormal situations such as falls. In the ambient group, we also have a number of studies using game consoles, intelligent floors, televisions, stationary alarms connected to beds and chairs. Note that some of these technologies, in particular game consoles such as Nintendo Wii, also have wearable and portable parts.

Abstracts coded based on the form factor of the technology
In the mechanical group, we have physical products that are neither portable nor wearable in the traditional sense. They are mainly assistive technologies such as walkers, robots, canes, airbags, and balance boards. As part of our inclusion criteria, we excluded assistive technology that did not have an ICT part. So all these mechanical devices demonstrate some form of “smartness” implemented using ICT. For instance, intelligent walkers and canes often have sensors and actuators for force or audio feedback based on user behavior [31].
The portable group includes smart phones, mobile phones, and tablets. Most portable devices have user interaction mechanisms such as a touch screen. However, most of the portable devices in our results were used for their integrated inertial sensors and could therefore have been coded as wearables.
The second largest group, wearables, includes a variety of sensor-based devices that are attached to the body with the intention of being worn over longer periods of time. A more detailed coding of this category revealed that waist was the most frequently used location (approximately n = 55), followed by trunk (approximately n = 31), wrist (approximately n = 19), and foot (approximately n = 15). Other locations included head, ear, neck, hip, thigh, and clothes.
6.3 Areas of intervention and use of technology
We coded all the abstracts based on the type of intervention. Some of these types followed from our initial model (see Fig. 3). Some additional bottom-up categories emerged from the coding. We also coded the abstracts, where possible, according to the intended context of use, such as home, nursing home, hospital, and community.
6.3.1 Type of intervention
Figure 7 shows the distribution of the abstracts across the different intervention types. Some of the types that emerged from the coding include movement analysis (e.g., gait analysis), movement tests (e.g., “timed-up-and-go” tests or other clinical tests), assisted walking (e.g., using canes and walkers), and balance control (mainly exercises). By far the largest group of papers deals with fall detection (n = 629). In addition, the second largest group (movement analysis, n = 217) mostly includes abstracts that deal with fall detection, albeit through generic movement analysis technology. The fourth largest group, fall prevention (n = 144), deals mostly with detecting falls just before they happen, i.e., the pre-fall phase. Risk assessment (n = 152), movement tests (n = 16), and physical training (n = 33) are the main preventive interventions. Additionally, a number of post-fall interventions (mainly rehabilitation and balance control) can probably be used as preventive interventions.

Distribution of the abstracts across the different intervention types
6.3.2 Technology form factor per intervention type
Figure 8 shows what form factors are used in each intervention type. We can see that wearables are the largest type used in risk assessment, movement analysis, fall detection, and rehabilitation. Ambient technologies are used largely in movement tests, physical training, balance control, but also in fall detection and prevention. Mechanical devices are used mainly in assisted walking and some in fall prevention.

Technology form factor applied in the various intervention categories
6.3.3 Major technology types per intervention
Figure 9 shows the prevalence of major technology categories (information systems, algorithms, sensors, network communication, and actuators) across intervention types. Sensors and algorithms are mostly interconnected since algorithms are mainly used to analyze data from sensors. Sensors and algorithms are used in most of the interventions. They are used to a lesser degree in physical training and balance control, where actuators are used more frequently. Actuators are also frequently used in assisted walking. The largest occurrence of information systems is in risk analysis, fall prevention, and rehabilitation.

Main technology categories used across intervention types
6.4 Intended usage context and population
Initially, we wanted to code based on the intended population (e.g., community-dwelling, frail), but for most papers this information did not exist in the abstracts (beyond general terms such as elderly or seniors that we searched for initially). We then decided to code based on the intended usage context where possible. The coding was done based on the words in the abstracts (where words like home, hospital, clinic etc. were used). Such words were more common than words classifying user groups. We assume the intended usage context to some extent indicates the target population. As shown in Fig. 10, the major contexts that emerged are home (n = 210), community (for community-dwelling seniors not bound to home, n = 56), hospital (n = 55), and nursing home (n = 34). As you can also see, we still have a very large “Unknown” class (n = 636).

Abstracts distributed per usage context
6.4.1 Use context per intervention type
Although the large proportion of the “Unknown” makes it difficult to conclude anything with significance about usage context, it is nevertheless interesting to see which intervention areas are most common in each context, including the unknown context itself. Figure 11 shows this distribution. As we can see, home setting is represented well in the preventive areas such as risk assessment, movement tests, movement analysis, and physical training. Hospital setting is prevalent in fall prevention, balance control, movement tests, and physical training. Nursing home is a main target setting for balance control and rehabilitation.

Type of intervention per user setting
6.4.2 Form factors used in each usage context
Figure 12 shows in which context the different technology form factors are used. Homes and nursing homes are main settings for ambient technology, while wearables are used mostly in hospitals and home setting. Mechanical devices are mainly used in the community.

Technology form factor most used in each user setting
6.4.3 Use context for major technology categories
Figure 13 shows the distribution of the major technology categories across the user settings. It shows that sensors are prevalent in all settings, while actuators are mainly used in nursing homes and in the community. Information systems have been used mainly in nursing homes and hospitals, followed by the community.

Major technology categories used in different user settings
6.5 Research contributions
It has been difficult to say much about research contributions based on the information in the abstracts. This is partly due to the brevity and the unstructured form of a large portion of the analyzed abstracts. In-depth information about what new knowledge was created is difficult to get from abstracts alone. We can, however, assume that most authors will mention major contributions, such as empirical results from field studies or major technological breakthroughs, in their abstracts. In this category we coded the abstracts based on the high-level criteria of “ICT area of contribution” and “scientific type of contribution.”
The ICT area of contribution says roughly what ICT-related properties of the artifacts were in focus for each paper. Some examples are accuracy, security, safety, interoperability, user-friendliness, etc. The types of scientific contribution is adopted from [32] and tells us whether the paper focuses mainly on design of concepts, on implementation of solutions, on validation of solutions, on field trials, etc.
6.5.1 ICT area of contribution
Figure 14 shows the areas of ICT research that the papers contribute to. The “Other” category includes more than 40 different areas with very low occurrence such as ethical issues, interoperability, reuse, performance, and engagement. By far the largest group is “accuracy” (n = 649) which is due to the high density of papers that report on more sensitive and specific algorithms for sensor data processing. Clinical validation (n = 122) includes all the papers where the technology itself was not in focus, but the clinical impact was reported as the main contribution. Acceptance (n = 122) refers to papers that mentioned user acceptance and user-friendliness as topic. Cost efficiency (n = 117) includes mainly abstracts that promote using off-the-shelf components (such as Web cameras) in implementing solutions and thereby reducing the cost of such solutions and making them more available. Unobtrusiveness (n = 89) was mentioned as a desirable property of, for example, wearable sensors. Real-time behavior (n = 51), network communication (n = 35), energy efficiency (n = 39), privacy (n = 39), and safety (n = 16) were other main categories. Service integration (n = 32) includes papers that mention integrating with existing services (e.g., fall detection services) as a contribution.

Number of abstracts per ICT-related area of contribution
6.5.2 Type of scientific contribution
As we can see in Fig. 15, the vast majority of the papers are about creating (n = 843), implementing (n = 780), and validating (n = 591) new concepts. Validation here means experimental or laboratory-based validation of a proof-of-concept prototype. Field evaluation (n = 92) includes those abstracts that reported real-world field-based evaluation of own or others’ technology. Problem investigation (n = 50) contains papers that try to conceptualize, or analyze some aspect of the problem (e.g., classification of falls) or develop models and theories. Solution selection (n = 18) refers to papers that try to compare a set of similar technologies (e.g., fall detection algorithms) and provide data about, e.g., their comparative accuracy. The last category is abstracts that report systematic or non-systematic literature surveys (n = 29).

Types of research contributions
6.5.3 Type of contribution per intervention type
Figure 16 shows what type of research is reported in each intervention area. Fall detection is the field with proportionally the largest number of papers that try to design, develop, and validate concepts. It is also the field with the lowest percentage of field evaluations. One possible explanation for this is the challenges of setting up fall detection trials with elderly users. Falls cannot be predicted, recruiting users is difficult, and there are ethical issues involved.

Types of research contribution per intervention
On the other hand, physical training and the related area of balance control have the largest proportion of field studies. This might be due to the fact that training and balance control field trials are easiest to set up because they involve healthy elderly users. Another factor is the fact that most of these trials use off-the-shelf game consoles, such as Nintendo Wii and Microsoft Kinect. As such, the focus is mainly on evaluating the effect of the technology rather than on creating new technology.
7 Discussion
In the following sections, we present four principal findings based on the data presented in the previous sections. We discuss the implications of these findings with regard to contributing to an agenda for pervasive and ubiquitous computing research within the area of age-related falls.
7.1 Too little focus on using ICT in preventive interventions
Fall detection is the most frequent application area among the papers we analyzed (see Fig. 7). In addition, the majority of the papers dealing with movement analysis and fall prevention (the second and the third largest groups of papers) in reality, deal with the pre-fall phase. This focus on falls as phenomenon can be the result of several things. First, falls are the most visible and devastating reminder of the challenge of age-related movement impairment. It is easy to motivate research that deals directly with falls. However, we need to keep in mind that falls can also be seen as a symptom of the lack of preventive interventions.
Second, a fall can be considered as a concrete incident that seems to be addressable by ICT components such as acceleration sensors. This does not mean that fall detection is easy. False positives are still a very common problem facing fall detection technology. Our point is that fall detection might seem to ICT researchers as conceptually easier to isolate and address using ICT. Preventive interventions need a more complex analytic model. This model needs to take into account a number of factors such as the lack of physical activity, cognitive and psychological aspects, sight, dizziness, poly-pharma, co-morbidities, lack of knowledge and training, etc. Another major challenge is the general resistance among community-dwelling seniors to actually follow preventive measures [33]. In this sense, using ICT for preventive interventions can seem a daunting undertaking.
Despite their complexity, complex problems such as fall prevention tend to require technology that is well diffused and does not bear any novelty or pose any challenge to an ICT researcher. For instance, conventional Web sites are used successfully to disseminate information in fall prevention interventions [34]. This lack of novelty might also be a factor contributing to preventive interventions not being so popular among ICT researchers. The solutions that are needed are simply not challenging enough.
Detecting falls at home or elsewhere is an important topic and will continue to attract research activities. So-called prolonged lie after falls has shown to be extremely dangerous, leading to not only prolonged hospitalization and increased fear of falling [35] but also dehydration, infections, hypothermia, pneumonia, and mortality [36]. Falls need to be detected quickly. But what we also need to address are the preventive aspects. Mobile technology is already used in sports and consumer lifestyle products and services. We need to apply lessons learned from these and similar areas, and create new technology and knowledge about how to prevent age-related falls before they happen. Only detecting falls is not a sustainable model for the aging society.
7.2 Too little focus on technologies for involving and empowering users
Our findings show that sensors and associated data processing algorithms are by far the largest group of technology being developed. At the same time, actuators—in our definition meaning technology that requires some form of active user involvement—constitute a comparably very small group (see Fig. 5). This resembles an automation mindset in the current research in this area, with healthcare being the “to be automated” activity. Another possible sign of this mindset is the apparent lack of information in the abstracts about the target user population (see Fig. 10, and also the next finding), which might indicate a lack of interest in understanding the users. On the other hand, the major political mindset for a sustainable future healthcare is concerned with active aging, patient empowerment, and self-management [37]. There seems to be a stark contrast between what our data show and what the political agenda asks for.
7.3 Too little focus on addressing context of use and future service models
Focus on context of use in the research phase is a strong indicator of how well the technology will eventually be accepted by the users and the market. The analyzed abstracts, however, are mainly about technical properties of components, such as algorithm accuracy (see for instance Figs. 5, 14). Properties that have to do with understanding the context of use—for instance, user acceptance, ease-of-use, business models, and privacy—are underrepresented in our data (Fig. 14). We know for instance that seniors are sensitive to social stigma and often do not consider themselves in risk of falling nor in need of fall-related technology [33]. We also know that seniors can have problems handling mobile and wearable technology because of, for instance, low muscular strength and tremor [21, 38]. Not taking such issues into consideration might mean that the technology will not get used despite its superior technical properties.
We also see very few papers that deal with the integration of new technical components into larger systems—such as service integration, interoperability, telecare, medical information systems. More importantly, abstracts that report service integration do not seem to have this aspect as their main focus. So they often report on conventional services using innovative ICT components. The typical setup is the administration of traditional clinic-based movement tests and interventions augmented with sensors. There are very few papers that report on new service models enabled by new ICT (for instance, self-managed movement tests at home using smart phones). This might mean that research in ICT is focusing on local optimization—components of high quality are being developed—but systemic optimizations are not being investigated.
7.4 Too little field evaluation of new technology
The vast majority of the analyzed papers are about creating new technology. Moreover, the data also show that almost 30 % of these papers lack any kind of validation (See Fig. 15, where only 70 % of new concepts are validated). We should also take into consideration that some of the papers that deal with field evaluations are not about new technology. They rather evaluate existing off-the-shelf technology (e.g., off-the-shelf devices with accelerometers, game consoles such as Nintendo Wii and Microsoft Kinect). It seems there is a sharp separation in the research community between those who are in charge of creating new technology, and those few who are concerned with field and clinical evaluation of technology.
Seniors with physical impairment are a fragile user group. Many aspects of movement impairment involve medical and social sciences and require multidisciplinary research. It is a challenging area to do field evaluations with new technology. Such evaluations require high-fidelity prototypes that can be used by users with no ICT experience. There are ethical issues involved in field trials of, e.g., fall detection (which is evident in the extra low level of field trials related to fall detection, see Fig. 16). Moreover, field trials often require that the novelty of technology is reduced in favor of its practical aspects. This lack of novelty might discourage ICT researchers from getting involved in real-world evaluations. However, these challenges should not mean that it is acceptable to keep on creating new technology that never gets validated and evaluated in the field. Although we can see a slight increase in the number of field trials in the last 2–3 years (see Fig. 15), we need a much bigger focus on field evaluations if we are committed to solving the societal problem of movement impairment.
7.5 Limitations of the study
SMS approach is not without limitations [9]. As opposed to SLRs, mapping studies catalogue papers and not primary studies. Number of papers is not a perfect indicator of the number of primary studies. This means that our study might contain several papers that report about the same primary study. Moreover, we use only abstracts in our analysis. This means that the accuracy of the cataloguing process depends on the quality of the abstracts. ICT-related research publications often do not use structured abstract [20] which results in poor accuracy when classifying papers based solely on abstracts.
In addition to these limitations of SMS as a method, our study specifically has a number of limitations and threats to internal validity as summarized below:
-
The automatic search and the search terms (see Table 2) can always be improved and expanded. We did a number of pilot searches with the goal of creating an accurate query, but we acknowledge that the query can be improved using additional terms.
-
One of our search engines, Scopus, limited downloadable abstracts to a maximum of 2000 even though our search resulted in 7617 hits. What we did was to sort the results based on relevance and download the 2000 most relevant abstracts. We do not believe it to be a major limitation that we omitted the remaining 5617 hits. Search engines are normally not accurate (therefore the need for the screening step). Moreover, SMS as a method is about trends and we believe statistical trends would not have been much different even if we had managed to download the remaining abstracts from Scopus.
-
Screening of the abstracts was done separately by both of the authors, meaning each of us did a screening of all papers. We included in the study only those abstracts that were included by both of the authors. This resulted in approximately 300 abstracts in total being rejected even though each was included by at least one of the authors.
-
The coding of the papers was done by only one author for each abstract. We divided the abstracts between ourselves and each of us coded half of the abstracts. An alternative could have been for both of us to code all the abstracts and merge the results. We decided to go for the single-coding alternative mainly because of the costs related to doing a double-coding. We did, however, tested the coding scheme through several pilot coding sessions, discuss the scheme extensively between ourselves, and improved it during the coding process.
Despite these limitations, we believe SMS is a strong methodology for demonstrating, at a macro-level, the trends within a research field. SMS is a quantitative method. With such a large number of abstracts as in our study (n = 1017), the effect of the above limitations has been reduced.
8 Conclusions
Our goal in this paper has been to map the research that has been done in the field of age-related falls in the recent years. In the previous sections, we have documented the methodology used for searching and categorizing this research. We have four major findings based on the analyzed data. These findings were described in the previous section.
Based on our four main findings, we propose four recommendations for a future research agenda in the area of age-related falls:
-
1.
More research is needed to develop ICT to support preventive and corrective interventions, such as fall prevention, fall risk assessment, and fall injury rehabilitation. We also need a better understanding of the underlying models and theories related to these types of intervention in order to create better ICT solutions.
-
2.
More research is needed to find out how ICT can empower seniors, e.g., by increasing awareness of own condition, active participation in interventions, active participation in the design of technology, and methods for adherence and compliance. We need a better understanding of the underlying values and incentives of seniors at risk of fall and apply this understanding to the design of new solutions.
-
3.
More research is needed on integrating component technologies into future deployable service models. We also need to know what new service models are enabled by these new technologies, how they will affect existing care models, and what new radically different service models can be invented.
-
4.
More research effort should be invested in evaluating solutions in real-world settings and collecting scientific empirical evidence from real-world trials. We should be more critical of fall-related technology that has not undergone rigorous evaluation.
Of course more research effort in these four areas would probably mean less research in other areas. We have not aimed in this study to suggest areas where research efforts should be reduced. We leave this exercise to the readers and possibly to a future study based on the data presented here.
References
World Health Organization (2007) WHO global report on falls prevention in older age. http://www.who.int
Kenny RA, Romero-Ortuno R, Cogan L (2013) Falls. Medicine (Baltimore) 41:155–159. doi:10.1016/j.mpmed.2012.12.007
Lofthus C, Osnes E, Falch J et al (2001) Epidemiology of hip fractures in Oslo, Norway. Bone 29:413–418. doi:10.1016/S8756-3282(01)00603-2
Lozano R, Naghavi M, Foreman K et al (2012) Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 380:2095–2128. doi:10.1016/S0140-6736(12)61728-0
van den Broek G, Cavallo F, Odetti L, Wehrmann C (2010) Ambient assisted living roadmap. IOS Press, Amsterdam
Weiser M (1991) The computer for the 21st century. Sci Am 265:94–104. doi:10.1038/scientificamerican0991-94
Dourish P (2001) Where the action is: the foundations of embodied interaction. MIT Press, Cambridge
Petersen K, Feldt R, Mujtaba S, Mattsson M (2008) Systematic mapping studies in software engineering. In: EASE’08 Proceedings of 12th international conference on evaluation and assessment in software engineering. British Computer Society, pp 68–77
Kitchenham BA, Budgen D, Pearl Brereton O (2011) Using mapping studies as the basis for further research—a participant-observer case study. Inf Softw Technol 53:638–651. doi:10.1016/j.infsof.2010.12.011
Kitchenham B, Charters S (2007) Guidelines for performing systematic literature reviews in software engineering. EBSE Technical Report Nr. EBSE-2007-01. Keele, UK
Clapton J, Rutter D, Sharif N (2009) SCIE systematic mapping guidance. Social care institute for excellence
Lavis J, Davies H, Oxman A et al (2005) Towards systematic reviews that inform health care management and policy-making. J Health Serv Res Policy 10(Suppl 1):35–48. doi:10.1258/1355819054308549
Howcroft J, Kofman J, Lemaire ED (2013) Review of fall risk assessment in geriatric populations using inertial sensors. J Neuroeng Rehabil 10:91. doi:10.1186/1743-0003-10-91
Kosse NM, Brands K, Bauer JM et al (2013) Sensor technologies aiming at fall prevention in institutionalized old adults: a synthesis of current knowledge. Int J Med Inform 82:743–752. doi:10.1016/j.ijmedinf.2013.06.001
Schwickert L, Becker C, Lindemann U et al (2013) Fall detection with body-worn sensors : a systematic review. Z Gerontol Geriatr 46:706–719. doi:10.1007/s00391-013-0559-8
De Bruin ED, Hartmann A, Uebelhart D et al (2008) Wearable systems for monitoring mobility-related activities in older people: a systematic review. Clin Rehabil 22:878–895. doi:10.1177/0269215508090675
Van Diest M, Lamoth CJC, Stegenga J et al (2013) Exergaming for balance training of elderly: state of the art and future developments. J Neuroeng Rehabil 10:101. doi:10.1186/1743-0003-10-101
Ward G, Holliday N, Fielden S, Williams S (2012) Fall detectors: a review of the literature. J Assist Technol 6:202–215. doi:10.1108/17549451211261326
Hawley-Hague H, Boulton E, Hall A et al (2014) Older adults’ perceptions of technologies aimed at falls prevention, detection or monitoring: a systematic review. Int J Med Inf 83:416–426. doi:10.1016/j.ijmedinf.2014.03.002
Kitchenham BA, Pearl Brereton O, Owen S et al (2008) Length and readability of structured software engineering abstracts. IET Softw 2:37. doi:10.1049/iet-sen:20070044
Brown CJ, Flood KL (2013) Mobility limitation in the older patient: a clinical review. JAMA 310:1168–1177. doi:10.1001/jama.2013.276566
Ketcham CJ, Stelmach GE (2004) Movement control in the older adult. In: Technology for adaptive aging. The National Academies Press, Washington DC, pp 64–92
Schultz AB (1992) Mobility impairment in the elderly: challenges for biomechanics research. Biomechanics 25:519–528
Verwey WB (2010) Diminished motor skill development in elderly: indications for limited motor chunk use. Acta Psychol (Amst) 134:206–214. doi:10.1016/j.actpsy.2010.02.001
Ketcham CJ, Stelmach GE (2001) Age-related decline in motor control. In: Handbook of the psychology of aging. pp 313–348
Clegg A, Young J, Iliffe S et al (2013) Frailty in elderly people. Lancet 381:752–762. doi:10.1016/S0140-6736(12)62167-9
Ensrud KE (2013) Epidemiology of fracture risk with advancing age. J Gerontol A Biol Sci Med Sci 68:1236–1242. doi:10.1093/gerona/glt092
Norwegian Institute of Public Health (2014) Osteoporosis and fractures in Norway—fact sheet. http://www.fhi.no/artikler/?id=74450
Farshchian B, Dahl Y (2015) Included abstracts from systematic mapping study of age-related falls and ICT. doi:10.5281/zenodo.16926
Dahl Y, Holbø K (2012) Value biases of sensor-based assistive technology. In: Proceedings of the designing interactive systems conference—DIS’12. p 572
Almeida O, Zhang M, Liu J-C (2007) Dynamic fall detection and pace measurement in walking sticks. In: High confidence medical devices, software, and systems and medical device plug-and-play interoperability, 2007 (HCMDSS-MDPnP 2007). IEEE, pp 204–206
Wieringa R, Maiden N, Mead N, Rolland C (2005) Requirements engineering paper classification and evaluation criteria: a proposal and a discussion. Requir Eng 11:102–107. doi:10.1007/s00766-005-0021-6
McInnes E, Askie L (2004) Evidence review on older people’s views and experiences of falls prevention strategies. Worldviews Evid Based Nurs 1:20–37. doi:10.1111/j.1741-6787.2004.04013.x
Nyman SR, Yardley L (2009) Web-site-based tailored advice to promote strength and balance training: an experimental evaluation. J Aging Phys Act 17:210–222
Johnston K, Grimmer-Somers K, Sutherland M (2010) Perspectives on use of personal alarms by older fallers. Int J Gen Med 3:231–237
De San Miguel K, Lewin G (2008) Personal emergency alarms: What impact do they have on older people’s lives? Australas J Ageing 27:103–105. doi:10.1111/j.1741-6612.2008.00286.x
The European Commission (2013) Horizon 2020 work programme 2014–2015. https://ec.europa.eu/programmes/horizon2020/
Brownsell S, Hawley MS (2004) Automatic fall detectors and the fear of falling. J Telemed Telecare 10:262–266. doi:10.1258/1357633042026251
Acknowledgments
This research is supported partly by the EU FP7 projects FARSEEING (Grant Agreement No. 288940), OPTET (Grant Agreement No. 317631) and by the Norwegian National Research Council funded project ADAPT. We thank the editors of the special issue and the anonymous reviewers for useful comments to earlier versions of this article.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Farshchian, B.A., Dahl, Y. The role of ICT in addressing the challenges of age-related falls: a research agenda based on a systematic mapping of the literature. Pers Ubiquit Comput 19, 649–666 (2015). https://doi.org/10.1007/s00779-015-0852-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00779-015-0852-1