
Abstract
Background
Ultrasound is suitable for routine examinations of capitellar osteochondritis dissecans because it can visualize both the subchondral bone and the overlying articular cartilage non-invasively. The radial head interferes with the sonographically visible area of the articular surface of the humeral capitellum, although the precise extent of this is currently unknown. This study aimed to investigate the visible area of the humeral capitellum using both anterior and posterior ultrasonographic scans.
Methods
Twelve elbows were used from cadavers with a mean age of 85.6 years. After marking a 45° angle in the anterior capitellum in a caudal direction using a drill, anterior and posterior, long-axis ultrasonographic scans were performed with the cadaveric elbows bent. The elbow-flexion angle at which the 45° point was obscured by the radial head was measured and these ultrasonic measurements were then verified by macroscopic observation.
Results
The elbow-flexion angle at which the 45° point was obscured by the radial head was 24° in anterior scans and 102° in posterior scans. These ultrasonic measurements corresponded to the macroscopic measurements. The results showed that anterior, long-axis ultrasound scans could visualize the capitellum from 45° through the rest of the anterior area at 24° flexion of the elbow: the radial head obscured the area of the capitellum that is 21° anterior to the elbow flexion angle. Similarly, posterior long-axis scans could visualize the capitellum from 45° through the rest of the posterior area at 102° flexion of the elbow: the radial head obscured the area of the capitellum that is 57° posterior to the elbow flexion angle. The radial head obscured a 78° (21° + 57°) arc of the capitellum in ultrasonography.
Conclusions
This study thus clarified the area of the humeral capitellum visible in both anterior and posterior ultrasound scans in the sagittal plane.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Osteochondritis dissecans (OCD) of the humeral capitellum is a refractory osteochondral injury of the elbow joint that usually occurs in adolescents, particularly in athletes such as throwers and gymnasts who are involved in highly demanding, repetitive, overhead or weight-bearing activities [1–4]. It is treated conservatively or surgically depending on disease stage and the stability of the lesion [1, 5–7].
Magnetic resonance imaging (MRI) and ultrasound scans can detect OCD early in the disease process, even when radiographs appear normal or demonstrate only subtle changes [8]. MRI can provide accurate assessment of the size, extent, and stability of an OCD lesion [9, 10]. However, this approach is expensive and time-consuming, which limits its repeated use. By contrast, ultrasound is very useful for routine examination of capitellar OCD because it is non-invasive and cost-effective [11]. Moreover, ultrasound can produce dynamic images and allow both the subchondral bone and the overlying articular cartilage to be visualized simultaneously. It also enables the observer to distinguish between stable and unstable lesions and provides relevant information for treatment decisions [12].
Ultrasound cannot visualize the entire area of the capitellum in a single scan, and both anterior and posterior long-axis scans are commonly used [8, 13]. In general, an anterior long-axis scan shows the proximal and middle parts of the anterior capitellum, whereas a posterior long-axis scan shows the middle and distal parts. However, the precise extent of the capitellum visible in ultrasound scans is currently unknown. In addition, when the elbow joint moves, the radial head (RH) obscures the sonographically visible area of the articular surface of the humeral capitellum. The purpose of this study was, therefore, to clarify the area of the humeral capitellum visible in anterior and posterior ultrasonographic scans.
Materials and methods
Marking the humeral capitellum
Twenty elbows were used in this study, from seventeen cadavers (six males and eleven females) with a mean age at death of 85.6 years (range 66–97 years). Specimens with obvious deformities, operation scars around the elbow, or a limited range of elbow motion were excluded. A skin incision was made on the lateral side of the elbow joint and the anterior area of the humeral capitellum was exposed, keeping the lateral collateral ligament and annular ligament intact. A hole was made with a 6 mm diameter drill at a 45° angle caudally in the anterior capitellum; the hole was at a 45° angle, anterior to the long axis of the humeral shaft, in the sagittal plane (Fig. 1a) and at the center of the anterior capitellum in the radioulnar plane (Fig. 1b).

Marking the humeral capitellum. a Drilling was performed at a 45° angle anteriorly to the humeral shaft in the sagittal plane. b Drill holes were created at the center of the anterior capitellum in the radioulnar plane
Ultrasonographic and macroscopic evaluation of the elbow flexion angle
After creating an osteochondral defect (the drill hole), a long-axis ultrasound scan was performed by using ultrasonic diagnostic equipment with a 12-MHz linear-array transducer (LOGIQ e; General Electric, Fairfield, CT, USA) and standard coupling gel. These evaluations were performed by an orthopaedic surgeon (H.G) with more than 20 years’ experience of the ultrasonographic examination of musculoskeletal tissue.
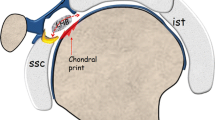
The location of the linear-array transducer was adjusted to maximize the width of the osteochondral defect in the long-axis ultrasound scan. The center of the defect was defined as point C (Fig. 2a). The flexion angle at which point C was covered by the RH in anterior, long-axis ultrasound scans (Fig. 2b) was measured using a goniometer by bending the cadaveric elbow from full extension with the forearm supinated. A posterior, long-axis ultrasound scan was also performed by extending the elbow from full flexion with the forearm supinated. The elbow-flexion angle was measured as point C became obscured by the RH.

Ultrasound images of the humeral capitellum (HC). a Posterior scan with the elbow flexed. The center of the defect was defined as point C (arrow). b Posterior scan. Point C was obscured by the radial head (RH)
Macroscopic observations were carried out to verify the results of the ultrasound measurements. The soft tissue around the elbow, apart from the collateral and annular ligaments, was carefully removed, macroscopic examinations were made from both anterior and posterior views, and the flexion angles at which point C became covered by the RH were measured using a goniometer. The method used to measure elbow flexion angles was the same in both ultrasound and macroscopic measurements: the goniometer was applied to the lateral side of the elbow, placing one ruler along the long axis of the humerus and adjusting the other ruler along the long axis of the radius.
This study was approved by our institutional review board (IRB No. 951).
Statistical analysis
To assess interobserver reliability, two independent orthopedic surgeons measured elbow flexion angles. Each observer was unaware of the other’s measurements. Interobserver reliability was evaluated by using the interclass correlation coefficient (ICC) with a 95 % confidence interval (CI) in a two-way random model with absolute agreement. To assess measurement accuracy, individual ultrasound measurements were compared with the macroscopic measurements by using the ICC with a 95 % CI. The statistical software R (R package; http://www.r-project.org/) was used for data analysis.
Results
Comparison of ultrasonographic and macroscopic measurements
The elbow flexion angles at which the RH covered point C by ultrasonography were 24.1° ± 4.9° in anterior long-axis scans and 101.6° ± 4.1° in posterior long-axis scans. The corresponding angles from the macroscopic observations were 21.8° ± 5.9° from the anterior view and 102.5° ± 5.2° from the posterior view. The ICC values (with 95 % CIs) for ultrasound and macroscopic measurements are shown in Table 1. The ICC values for interobserver reliability were 0.991 (95 % CI 0.983–0.995) and 0.977 (95 % CI 0.961–0.987) for macroscopic and ultrasonographic measurements, respectively.
Modeling visibility of the humeral capitellum by ultrasonography
We made the assumption that, as a model of the elbow, the humeral capitellum could be represented as a perfect circle in the sagittal plane and the area of the capitellum could be described as an angle measured from the long axis of the humerus. In anterior ultrasound scans, point C was found to disappear when the elbow joint was flexed to a mean angle of 24°. As point C was located at a 45° angle, antero–caudally, in the humeral capitellum, it should be possible to visualize this point from 45° in the antero–caudal direction through the rest of the anterior area by using an anterior ultrasound scan with the elbow joint flexed at 24° (Fig. 3a). This means that the RH obscures the area of the capitellum that is 21° anterior to the angle of elbow flexion in an anterior long-axis scan (Fig. 3b).

Modeling of the humeral capitellum (HC): anterior. a Visible area (solid arrow) in anterior long-axis ultrasound scans with elbow flexed at 24°, from 45° to the anterior. b The area obscured by the radial head (RH) is indicated by the double arrow
Similarly, in posterior ultrasound scans, point C was shown to disappear when the elbow was flexed to a mean angle of 102°. Thus, the humeral capitellum was visible from a 45° angle in the antero–caudal direction through the rest of the posterior area by using a posterior ultrasound scan with the elbow flexed at 102° (Fig. 4a). This means that the RH obscures the area of the capitellum that is 57° posterior to the angle of elbow flexion in a posterior long-axis scan (Fig. 4b). Therefore, the RH obscures a total arc of 78° (21° + 57°) of the capitellum in ultrasound scans with the forearm supinated. An alternative approach to this calculation is that the RH obscured point C anteriorly at 24° flexion of the elbow joint and posteriorly at 102° flexion of the elbow joint, as observed in ultrasound scans, so point C was obscured by the RH between 24° and 102°, or a total 78° arc of the elbow joint motion.

Modeling of the humeral capitellum (HC): posterior. a Visible area (dotted arrow) in posterior long-axis ultrasound scans with elbow flexed at 102°, from 45° to the distal and posterior. b Area obscured by radial head (RH) is indicated by the double arrow
Discussion
Capitellar OCD most commonly affects young athletes who are engaged in sports that repetitively stress the elbow. Repeated compression and shear forces to the capitellum are thought to be the main etiological factor for OCD, which is a localized disorder of the subchondral bone, resulting in separation and fragmentation of the articular surface and underlying bone [1, 2, 4]. This lesion is distinct from Panner’s disease (osteochondrosis), which is typically seen in boys under the age of 10 years and resolves spontaneously [14, 15].
Ultrasound is a non-invasive, real-time diagnostic tool that can visualize both the subchondral bone and the overlying articular cartilage simultaneously, and so is very useful for routine examinations of capitellar OCD. Sonography of the elbow joint is a well-established technique [13], and ultrasound findings of capitellar OCD at different disease stages and types have been reported [8, 12]. However the limits of the area of the capitellum visible by sonography have not previously been defined.
In this study we have clarified the area of the humeral capitellum visible in both anterior and posterior ultrasound scans in the sagittal plane. The ICC values for interobserver reliability indicated almost perfect reliability in both the macroscopic and ultrasonographic measurements [16] and, as shown in Table 1, the measurements made using anterior and posterior ultrasound scans can both be regarded as reliable [17].
Of course, the area visible by sonography will vary depending on the range of motion in the elbow joint. Takahara et al. [7] previously reported that the average range of motion at the elbow, in 106 patients with OCD of the humeral capitellum, was −13.6° in extension and 128.0° in flexion in initial physical examinations. When we applied our model of ultrasound examination of the elbow to the data from these patients, we found it was possible to visualize the capitellum from 34.6° (13.6° + 21°) in the antero–caudal direction through the rest of the anterior area, in an anterior ultrasound scan at an elbow flexion of 13.6° (maximum extension), and to visualize the capitellum from 71.0° (128.0° − 57°) in the antero-caudal direction through the rest of the posterior area, in a posterior ultrasound scan at an elbow flexion of 128.0° (maximum flexion) (Fig. 5). We would expect to be able to detect capitellar OCD lesions in such patients because the visible areas in the two scans would overlap. This example demonstrated that the whole area of the capitellum could be evaluated for patients with mild restrictions in their elbow motion by using ultrasonographic anterior and posterior scans. To put it precisely, as the RH covers a 78° arc of the capitellum, we can examine the entire area of the capitellum in an elbow for which the total sagittal arc of motion is more than 78° by using both anterior and posterior ultrasound scans. Therefore, ultrasound is a useful technique for initial examination and medical check-up.

Model of the visible area of the capitellum for an elbow joint with a flexion range of 13.6–128.0°. Visible areas in anterior scans (solid arrow), in posterior scans (dotted arrow) and in both scans (double arrow)
It might be possible to investigate the sonographically visible area of the capitellum by inserting a needle along the anterior/posterior ultrasound long-axis scan, with the cadaveric elbow either fully extended or flexed. However, the angles would not always be the same, because the laxity of the elbow joints varied in different cadavers. Moreover, the area obscured by the RH could not be clarified using that method. Therefore, we used a mark in the anterior capitellum at a 45° angle caudally, which is where capitellar OCD is most likely to occur [18], measured the elbow-flexion angles at which the 45° point was obscured by the RH, and then calculated the area obscured by the RH. In this way we could establish the visible area of the capitellum. We drilled holes at the center of the capitellum, so that we did not overestimate the visible area. If the holes had been made laterally, the elbow-flexion angles at which point C was obscured by the RH would have been bigger in anterior ultrasound scans and the visible area calculated from anterior scans would have been wider. This is because the articular surface of the RH is ellipsoid in shape [19], so that the anteroposterior length of the articular surface of the RH is shorter at the side than at the center. For the same reason, the elbow-flexion angles at which point C would be obscured by the RH would be smaller in posterior ultrasound scans and the visible area calculated from posterior scans would be wider. Ultrasound examinations are usually performed using both long-axis and short-axis scans, with long-axis scans showing sagittal plane views and short-axis scans showing axial plane views of the capitellum. In this study, we only used long-axis scans because our objective was to determine the ultrasonographically visible area of the capitellum in the sagittal plane. In addition, long-axis ultrasound scans can visualize the capitellum and RH simultaneously and are therefore suitable for dynamic observations of moving elbow joints.
This study had some limitations. First, OCD at the capitellum is most frequent in adolescents, who are skeletally immature, and so have smaller bones than the cadaveric specimens used in our study. However, the positional relationship described by the angles measured was the same, irrespective of the size of the bones. Second, to be precise, the humeral capitellum is not positioned on the long axis of the humerus, but is anterior to it. For practical reasons, all the angles describing the location of the capitellum were measured from the long axis of the humerus, because they corresponded to the elbow-flexion angles. Third and finally, the visible area of the capitellum might be expected to change depending on the rotation of the forearm, because the RH is ellipsoid in shape [19]. However, ultrasound examinations of the elbow are usually performed with the forearm supinated [13], as in our study.
In summary, assuming that the humeral capitellum can be represented as a perfect circle in the sagittal plane, the RH covers a 78° arc of the capitellum when the forearm is supinated in ultrasonography. Expressing the whole area of the capitellum as a 360° angle, and measuring angles from the long axis of the humerus, which correspond to the elbow-flexion angles, the RH obscures 21° of the capitellum anterior to the elbow-flexion angle in anterior long-axis scans and 57° of the capitellum posterior to the elbow-flexion angle in posterior long-axis scans. This study clarified the area of the humeral capitellum visible in both anterior and posterior ultrasound scans in the sagittal plane.
References
Baker CL 3rd, Romeo AA, Baker CL Jr. Osteochondritis dissecans of the capitellum. Am J Sports Med. 2010;38(9):1917–28.
Cain EL Jr, Dugas JR, Wolf RS, Andrews JR. Elbow injuries in throwing athletes: a current concepts review. Am J Sports Med. 2003;31(4):621–35.
Jobe FW, Nuber G. Throwing injuries of the elbow. Clin Sports Med. 1986;5(4):621–36.
Jackson DW, Silvino N, Reiman P. Osteochondritis in the female gymnast’s elbow. Arthroscopy. 1989;5(2):129–36.
Matsuura T, Kashiwaguchi S, Iwase T, Takeda Y, Tasui N. Conservative treatment for osteochondrosis of the humeral capitellum. Am J Sports Med. 2008;36(5):868–72.
Shimada K, Yoshida T, Nakata K, Hamada M, Akita S. Reconstruction with an osteochondral autograft for advanced osteochondritis dissecans of the elbow. Clin Orthop Relat Res. 2005;435:140–7.
Takahara M, Mura N, Sasaki J, Harada M, Ogino T. Classification, treatment, and outcome of osteochondritis dissecans of the humeral capitellum. J Bone Joint Surg Am. 2007;89(6):1205–14.
Takahara M, Shundo M, Kondo M, Suzuki K, Nambu T, Ogino T. Early detection of osteochondritis dissecans of the capitellum in young baseball players. Report of three cases. J Bone Joint Surg Am. 1998;80(16):892–7.
Bowen RE, Otsuka NY, Yoon ST, Lang P. Osteochondral lesions of the capitellum in pediatric patients: role of magnetic resonance imaging. J Pediatr Orthop. 2001;21(3):298–301.
Kijowski R, Tuite M, Sanford M. Magnetic resonance imaging of the elbow. Part 1: normal anatomy, imaging technique, and osseous abnormalities. Skeletal Radiol. 2004;33(12):685–97.
Parker L, Nazarian LN, Carrino JA, Morrison WB, Grimaldi G, Frangos AJ, Levin DC, Rao VM. Musculoskeletal imaging: medicare use, costs, and potential for cost substitution. J Am Coll Radiol. 2008;5(3):182–8.
Takahara M, Ogino T, Tsuchida H, Takagi M, Kashiwa H, Nambu T. Sonographic assessment of osteochondritis dissecans of the humeral capitellum. AJR. 2000;174(2):411–5.
Barr LL, Babcock DS. Sonography of the normal elbow. AJR. 1991;157(4):793–8.
Panner HJ. A peculiar affection of the capitulum humeri, resembling Calve-Perthes disease of the hip. Acta Radiol. 1929;10(3):234–42.
Smith MGH. Osteochondritis of the humeral capitellum. J Bone Joint Surg Br. 1964;46(1):50–4.
Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33(1):159–74.
Fleiss JL, Cohen J. The equivalence of weighted kappa and the intraclass correlation coefficient as measures of reliability. Educ Psychol Meas. 1973;33(3):613–9.
Maezawa S, Muro S, Nishikimi J, Ito H, Ito S, Mizuno N, Mori M, Yamashita H. Roentgenologic evaluation of etiology of osteochondritis dissecans of the elbow. Rinshou Seikeigeka (Clinical Orthopaedic Surgery). 1985;20(10):1157–63 (in Japanese).
Puchwein P, Heidari N, Dorr K, Struger L, Pichler W. Computer-aided analysis of radial head morphometry. Orthopedics. 2013;36(1):e51–7.
Acknowledgments
We thank Y. Mabuchi at the Department of Anatomy, Nagoya City University (Nagoya, Japan), for performing the dissections. We also thank Y. Nishimori and A. Murase at the Department of Orthopedic Surgery, Nagoya City University Graduate School of Medical Science for their contributions.
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
About this article

Cite this article
Takenaga, T., Goto, H., Nozaki, M. et al. Ultrasound imaging of the humeral capitellum: a cadaveric study. J Orthop Sci 19, 907–912 (2014). https://doi.org/10.1007/s00776-014-0637-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00776-014-0637-9