
Abstract
Background
Although delayed union or pseudoarthrosis after lumbar arthrodesis has been recognized as a major radiographic complication, little has been known about the effect of fusion status on the patient’s quality-of-life (QOL) outcome. The purpose of this study was to investigate the effects of fusion status after posterior lumbar interbody fusion (PLIF) on QOL outcomes by using the Japanese Orthopaedic Association Back Pain Evaluation Questionnaire (JOABPEQ).
Methods
Among 100 patients who underwent single level PLIF for spinal canal stenosis, 29 who had not achieved fusion (incomplete fusion group) and 29 age- and sex ratio-matched patients who had achieved fusion (fusion group) 6 months after surgery were enrolled. Overall clinical evaluation was performed before and 6 months after surgery: the physician determined the Japanese Orthopaedic Association Score for Low Back Pain (JOA score); the JOABPEQ and visual analogue scale (VAS) values were collected. The recovery rate of the JOA score, changes in all JOABPEQ subdomain scores and in the VAS values were calculated. All variables were compared between the groups.
Results
The preoperative JOA scores, JOABPEQ scores of all subdomains, and VAS values of all categories did not differ between the groups. The recovery rate was higher in the fusion group than the incomplete fusion group (p = 0.0185). The changes in the JOABPEQ scores for walking ability and social life function were significantly greater in the fusion group than the incomplete fusion group (walking ability, p = 0.0172; social life function, p = 0.0191). The postoperative VAS values and changes in the VAS values for all categories did not differ between the groups.
Conclusions
Incomplete fusion after PLIF correlated with poor improvement in walking ability and social life function. Therefore, the achievement of fusion after PLIF is essential to obtain better patient QOL outcomes.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Posterior lumbar interbody fusion (PLIF) is performed to decompress the neural tissues and fuse the affected motion segments. Although pedicle screw fixation has dramatically reduced the incidence of pseudoarthrosis (1.7–10 %) [1–4], delayed union or pseudoarthrosis remains a major radiographic complication after PLIF.
The clinical importance of fusion status has been underestimated on the basis of reports in which pseudoarthrosis did not affect the short-term outcome after lumbar arthrodesis [3, 5–9]. However, the clinical evaluations in the majority of those studies were primarily physician-based assessments. The effect of fusion status after PLIF on patient-based quality-of-life (QOL) outcomes remains unknown. We hypothesized that non-fusion after PLIF negatively affects QOL outcomes.
The purpose of this study was to investigate the effect of fusion status after PLIF on patient-based QOL outcomes by using the Japanese Orthopaedic Association Back Pain Evaluation Questionnaire (JOABPEQ) [10].
Methods
This study was a retrospective review of prospectively collected data and approved by the research ethics committee of National Hospital Organization Osaka Minami Medical Center (No. 24-11).
Potential subjects were 117 consecutive patients who underwent one-level PLIF (including single-level PLIF combined with laminectomy at other levels) for treatment of lumbar spinal canal stenosis between November 2010 and April 2013 at National Hospital Organization Osaka Minami Medical Center. The indications of PLIF were as follows: spondylolisthesis with slippage greater than 3 mm and/or posterior opening greater than 5° on dynamic lateral plain radiograph; foraminal stenosis requiring total fecetectomy for decompression. Out of the total, 17 patients were excluded: 12 patients with rheumatoid arthritis and 5 patients undergoing dialysis for chronic renal failure. Finally, 100 patients [mean age, 66.8 years (range 40–89 years)] were evaluated 6 months after surgery for fusion status by examining anteroposterior and dynamic lateral plain radiographs using Ito’s method [2] by the first author (T.M.), blindly. In brief, the bony fusion as apparent on the radiographs was classified into 4 grades: grade 1, complete fusion achieved with formation of a bone bridge between the upper and lower vertebral bodies; grade 2, bone bridge not formed, but formation of a thick fusion mass with no translucency observed around the cages; grade 3, fusion not achieved and translucency apparent around the cages; grade 4, cage sinking into the vertebral body or bone resorption around the cages. Fusion was defined as grade 1 or 2 with a flexion–extension angle of less than 5°. On the basis of these criteria, incomplete fusion was observed in 29 of the 100 patients, who were designated the incomplete fusion group. This group included 15 men and 14 women with a mean age of 71.1 years (range 49–84 years) at the time of surgery. Of the 71 patients in whom fusion had occurred, 29 patients whose age (±2 years) and sex matched those of the incomplete fusion group were designated as the fusion group. The fusion group included 15 men and 14 women with a mean age of 70.9 years (range 49–86 years) at the time of surgery.
Surgical procedure
In all patients, PLIF was performed through conventional open surgery (without minimally invasive surgery techniques) using carbon-polyetheretherketone cages and titanium pedicle screws and rods. The disc and cartilaginous endplates were removed to prepare the graft bed, and morselized local bone chips were implanted in the anterior and lateral portions of the interbody space. Two cages filled with local bone chips were inserted into the intervertebral space, and two bone blocks were inserted lateral to the cages. Finally, pedicle screws were inserted and connected with rods. Partial laminectomy at other levels was added if required.
Demographic and clinical characteristics
Age at the time of surgery, gender, number of levels of additional laminectomy, and level of the fusion segments were obtained from the medical charts and operative notes.
Outcome assessment
An overall clinical evaluation was made before and 6 months after surgery using the JOA Score for Low Back Pain (JOA score) [11]. The patients also answered the JOABPEQ and reported visual analogue scale (VAS) values for low back pain, pain in the buttocks and lower limb(s), and numbness in the buttocks and lower limb(s) at the same time points. The recovery rate based on the JOA score was calculated according to Hirabayashi’s method [(postoperative score − preoperative score)/(29 − preoperative score) × 100 (%)] [12]. The changes in the scores (postoperative score − preoperative score) in all 5 subdomains of the JOABPEQ (low back pain, lumbar function, walking ability, social life function, and mental health) and in the VAS values (postoperative VAS value − preoperative VAS value) for all categories were also calculated.
Statistical analysis
We compared the above parameters between the fusion and incomplete fusion groups. The Mann–Whitney U test was used to compare the age, number of levels of additional laminectomy, pre- and post-operative JOA scores, JOA score-based recovery rate, pre- and post-operative JOABPEQ score for each subdomain, change in the score for each JOABPEQ subdomain, pre- and post-operative VAS values for each category, and change in the VAS value for each category. Fisher’s exact probability test was used to compare genders. The chi-square test was used to compare the level of the fusion segments. Intraobserver and interobserver agreement for evaluation of fusion status were assessed with Cohen’s kappa coefficient in the first 25 patients blindly. For the analysis of intraobserver reliability, the first author (T.M.) evaluated the fusion status twice, with a week’s interval. For the analysis of interobserver reliability, the two spinal surgeons (T.M. and Y.M.) evaluated fusion status. Statistical analysis was performed using StatView Version 5.0 (SAS Institute Inc., Cary, NC, USA) except Cohen’s kappa coefficient. Cohen’s kappa coefficient was analyzed using R version 2.8.1 (The R Foundation for Statistical Computing). Differences were considered statistically significant at p < 0.05.
Results
Fusion was achieved within 6 months after surgery in 71 of overall 100 patients (71.0 %). No surgical site infection or instrumentation failure was observed. The age, gender, number of levels of additional laminectomy, and fusion level did not differ between the groups (Table 1).
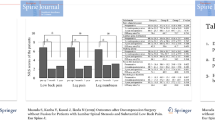
The preoperative JOA score, JOABPEQ scores for all subdomains, and VAS values for all categories did not differ between the groups (Tables 2, 3, 4).
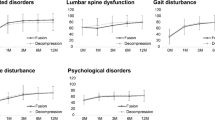
The postoperative JOA score and the associated recovery rate were higher in the fusion group than in the incomplete fusion group (JOA score, p = 0.0202; recovery rate, p = 0.0185) (Table 2). The postoperative scores of JOABPEQ for low back pain, walking ability, and social life function were significantly higher in the fusion group than in the incomplete fusion group (low back pain, p = 0.0234; walking ability, p = 0.0104; social life function, p = 0.0043) (Table 3). The changes in the JOABPEQ subdomain scores for low back pain, lumbar function, and mental health did not differ between the groups (Table 3). However, the changes in the JOABPEQ subdomain scores for walking ability and social life function were significantly greater in the fusion group than in the incomplete fusion group (walking ability, p = 0.0172; social life function, p = 0.0191) (Table 3). The postoperative VAS values and the changes in the VAS values for all categories did not differ between the groups (Table 4).
Intraobserver agreement for evaluation of fusion status had a kappa value of 0.884 and interobserver agreement had a kappa value of 0.750.
Discussion
This study revealed that fusion status affected not only clinical outcome in terms of the physician’s assessment (JOA score) but also patient-based QOL outcomes assessed by the JOABPEQ, though it did not affect VAS values for all categories. In particular, the JOABPEQ revealed that incomplete fusion after PLIF was associated with patients’ functional disability in walking ability and social life function. The JOABPEQ could reveal what kinds of disability the patients under incomplete fusion suffered from. Furthermore, the JOABPEQ was more sensitive than VAS scales for detecting postoperative patient QOL changes. To the best of our knowledge, this is the first report demonstrating an effect of fusion status after PLIF on the patient’s QOL outcome by using the JOABPEQ.
The effect of fusion status after lumbar arthrodesis on the patient’s outcome has been controversial. Reports with long-term follow-up have suggested that pseudoarthrosis adversely affects the patient’s outcome [9, 13]. In contrast, many authors have reported that pseudoarthrosis after lumbar arthrodesis did not affect the short-term outcome [3, 5–9]. Tsutsumimoto et al. [9] reported that clinical results 5 years after posterolateral lumbar fusion were better in patients with fusion than in those without fusion, although there was no significant difference in the clinical results after 1 and 3 years’ follow-up. Lee et al. [3] reported no difference in outcome in terms of the Korean Oswestry Disability Index, SF-36, and VAS 1 year after PLIF between patients who achieved fusion and those with pseudoarthrosis. However, the interpretation of these reports is complicated by their outcome evaluation methods (using predominantly physician-based outcome measurements), inhomogeneous fusion techniques and numbers of fusion levels, and different definitions of fusion. In this study, patients treated with the same surgical technique and one-level PLIF were evaluated by using patient-based outcome measures.
A number of trends in patient evaluation have resulted in the development and growing use of patient-based outcome measures to assess functional status and health-related QOL. In the field of lumbar spine disease, VASs or numerical rating scales have been used to quantify symptoms, the Roland-Morris Disability Questionnaire (RDQ) and Oswestry Disability Index have been used as lumbago-specific QOL measures, and the SF-36 has been used as a comprehensive measure of QOL. The JOABPEQ is a newly developed patient-based evaluation questionnaire drawn from the SF-36 and RDQ [10]. Its reproducibility, validity, and sensitivity have been verified previously [10, 14–16]. The JOABPEQ consists of 25 questions and five functional scores (low back pain, lumbar function, walking ability, social life function, and mental health) that are calculated as weighted sums of the corresponding domains according to the formulas provided [10]. The minimally clinical important difference is 20 points between two time points [10]. The advantage of the JOABPEQ is that it allows independent evaluation of 5 subdomains of low back pain-related disability, whereas the RDQ and ODI both result in a single overall score. The detailed evaluation provided by the JOABPEQ may have contributed to the clarification of the effect of fusion status on the patient’s outcome in this study.
We chose 6 months postoperatively as the time for final evaluation. One reason for this is because maximum recovery in terms of the JOABPEQ results is expected to occur between 6 and 12 months after lumbar decompression surgery and PLIF [17, 18]. The other is because the fusion rate after PLIF is reportedly over 90 % 1 year postoperatively [1–4]. Furthermore, several factors such as the emergence of adjacent segment disease and degenerative changes would make it difficult to evaluate the true effect of fusion status on patient outcome after a longer follow-up period. In order to evaluate the true effect of fusion status, we chose 6 months after surgery as the final evaluation time. Moreover, we used an age-matched control group to exclude any effect of an age difference between the groups, as the mean age of the overall fusion group (n = 71, 65.0 years) was about 6 years younger than that of the incomplete fusion group. This was important because age has previously been shown to affect JOABPEQ subdomain scores [19].
We speculate about several reasons why incomplete fusion caused the poor improvement in walking ability and social life function. One possible reason is low back pain by endplate injury. It has been reported that lumbar endplate lesions associated with disc degeneration could induce low back pain [20]. The cages at the incomplete fusion segment could also injure the adjacent vertebral endplates by repetitive micro-motion. The other possible reason is patients’ fear-avoidance behavior caused by incomplete fusion. If patients were informed of incomplete fusion, they might restrain their daily activities to prevent undesirable results such as instrumentation failure. However, we neither took magnetic resonance images or computed tomographies for all patients, nor evaluated fear-avoidance behavior, and so further investigation is needed to clarify the reason why the fusion status affects patients’ QOL.
In conclusion, we investigated patients’ QOL outcomes after PLIF by using the JOABPEQ, a patient-based QOL outcome evaluation. This assessment revealed that QOL outcomes were in fact better in the fusion group than in the incomplete fusion group. Specifically, the JOABPEQ revealed that incomplete fusion after PLIF correlated with poor improvement in walking ability and social life function. This result indicates that achievement of fusion after PLIF is essential for not only long-term but also short-term QOL outcomes. We plan to perform additional studies to determine whether the QOL outcomes of patients in the incomplete fusion group can improve if fusion is later achieved, or even if fusion is not achieved.
References
Ito Z, Imagama S, Kanemura T, Hachiya Y, Miura Y, Kamiya M, Yukawa Y, Sakai Y, Katayama Y, Wakao N, Matsuyama Y, Ishiguro N. Bone union rate with autologous iliac bone versus local bone graft in posterior lumbar interbody fusion (PLIF): a multicenter study. Eur Spine J. 2013;22(5):1158–63.
Ito Z, Matsuyama Y, Sakai Y, Imagama S, Wakao N, Ando K, Hirano K, Tauchi R, Muramoto A, Matsui H, Matsumoto T, Kanemura T, Yoshida G, Ishikawa Y, Ishiguro N. Bone union rate with autologous iliac bone versus local bone graft in posterior lumbar interbody fusion. Spine. 2010;35(21):E1101–5.
Lee JH, Lee JH, Park JW, Lee HS. Fusion rates of a morselized local bone graft in polyetheretherketone cages in posterior lumbar interbody fusion by quantitative analysis using consecutive three-dimensional computed tomography scans. Spine J. 2011;11(7):647–53.
Sakaura H, Yamashita T, Miwa T, Ohzono K, Ohwada T. Outcomes of 2-level posterior lumbar interbody fusion for 2-level degenerative lumbar spondylolisthesis. J Neurosurg Spine. 2013;19(1):90–4.
Epstein NE. Fusion rates and SF-36 outcomes after multilevel laminectomy and non-instrumented lumbar fusions in a predominantly geriatric population. J Spinal Disord Tech. 2008;21(3):159–64.
Fischgrund JS, Mackay M, Herkowitz HN, Brower R, Montgomery DM, Kurz LT, 1997 Volvo Award winner in clinical studies. Degenerative lumbar spondylolisthesis with spinal stenosis: a prospective, randomized study comparing decompressive laminectomy and arthrodesis with and without spinal instrumentation. Spine. 1997;22(24):2807–12.
Herkowitz HN, Kurz LT. Degenerative lumbar spondylolisthesis with spinal stenosis. A prospective study comparing decompression with decompression and intertransverse process arthrodesis. J Bone Joint Surg Am. 1991;73(6):802–8.
Nakashima H, Yukawa Y, Ito K, Horie Y, Machino M, Kanbara S, Morita D, Imagama S, Ishiguro N, Kato F. Extension CT scan: its suitability for assessing fusion after posterior lumbar interbody fusion. Eur Spine J. 2011;20(9):1496–502.
Tsutsumimoto T, Shimogata M, Yoshimura Y, Misawa H. Union versus nonunion after posterolateral lumbar fusion: a comparison of long-term surgical outcomes in patients with degenerative lumbar spondylolisthesis. Eur Spine J. 2008;17(8):1107–12.
Fukui M, Chiba K, Kawakami M, Kikuchi S, Konno S, Miyamoto M, Seichi A, Shimamura T, Shirado O, Taguchi T, Takahashi K, Takeshita K, Tani T, Toyama Y, Yonenobu K, Wada E, Tanaka T, Hirota Y, JOA Back Pain Evaluation Questionnaire (JOABPEQ)/JOA Cervical Myelopathy Evaluation Questionnaire (JOACMEQ). The report on the development of revised versions. April 16, 2007. The Subcommittee of the Clinical Outcome Committee of the Japanese Orthopaedic Association on Low Back Pain and Cervical Myelopathy Evaluation. J Orthop Sci. 2009;14(3):348–65.
Izumida S, Inoue S. Assessment of treatment for low back pain. Japanese Orthopaedic Association. J Jpn Orthop Assoc. 1986;60(3):391–4 (in Japanese).
Hirabayashi K, Miyakawa J, Satomi K, Maruyama T, Wakano K. Operative results and postoperative progression of ossification among patients with ossification of cervical posterior longitudinal ligament. Spine. 1981;6(4):354–64.
Kornblum MB, Fischgrund JS, Herkowitz HN, Abraham DA, Berkower DL, Ditkoff JS. Degenerative lumbar spondylolisthesis with spinal stenosis: a prospective long-term study comparing fusion and pseudarthrosis. Spine. 2004;29(7):726–33.
Fukui M, Chiba K, Kawakami M, Kikuchi S, Konno S, Miyamoto M, Seichi A, Shimamura T, Shirado O, Taguchi T, Takahashi K, Takeshita K, Tani T, Toyama Y, Wada E, Yonenobu K, Tanaka T, Hirota Y. JOA Back Pain Evaluation Questionnaire: initial report. J Orthop Sci. 2007;12(5):443–50.
Fukui M, Chiba K, Kawakami M, Kikuchi S, Konno S, Miyamoto M, Seichi A, Shimamura T, Shirado O, Taguchi T, Takahashi K, Takeshita K, Tani T, Toyama Y, Yonenobu K, Wada E, Tanaka T, Hirota Y. Japanese Orthopaedic Association Back Pain Evaluation Questionnaire. Part 2. Verification of its reliability: the Subcommittee on Low Back Pain and Cervical Myelopathy Evaluation of the Clinical Outcome Committee of the Japanese Orthopaedic Association. J Orthop Sci. 2007;12(6):526–32.
Fukui M, Chiba K, Kawakami M, Kikuchi S, Konno S, Miyamoto M, Seichi A, Shimamura T, Shirado O, Taguchi T, Takahashi K, Takeshita K, Tani T, Toyama Y, Wada E, Yonenobu K, Tanaka T, Hirota Y. Japanese Orthopaedic Association Back Pain Evaluation Questionnaire. Part 3. Validity study and establishment of the measurement scale: subcommittee on Low Back Pain and Cervical Myelopathy Evaluation of the Clinical Outcome Committee of the Japanese Orthopaedic Association, Japan. J Orthop Sci. 2008;13(3):173–9.
Miyamoto M. Clinical Outcome Committee of the Japanese Society for Spine Surgery and Related Research. Validation study of JOABPEQ for patients with lumbar spinal canal stenosis. J Spine Res. 2012;3(3):543 (in Japanese).
Watanabe K, Yamazaki A, Katsumi K, Ohashi M. Surgical outcomes of spinal fusion with 2-year follow-up for lumbar degenerative disorders. J Spine Res. 2011;2(9):1473–8 (in Japanese).
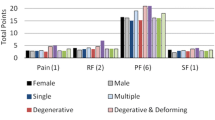
Ohtori S, Ito T, Yamashita M, Murata Y, Morinaga T, Hirayama J, Kinoshita T, Ataka H, Koshi T, Sekikawa T, Miyagi M, Tanno T, Suzuki M, Aoki Y, Aihara T, Nakamura S, Yamaguchi K, Tauchi T, Hatakeyama K, Takata K, Sameda H, Ozawa T, Hanaoka E, Suzuki H, Akazawa T, Suseki K, Arai H, Kurokawa M, Eguchi Y, Suzuki M, Okamoto Y, Miyagi J, Yamagata M, Toyone T, Takahashi K, Chiba Low Back Pain Research Group. Evaluation of low back pain using the Japanese Orthopaedic Association Back Pain Evaluation Questionnaire for lumbar spinal disease in a multicenter study: differences in scores based on age, sex, and type of disease. J Orthop Sci. 2010;15(1):86–91.
Wang Y, Videman T, Battié MC. ISSLS prize winner: lumbar vertebral endplate lesions: associations with disc degeneration and back pain history. Spine. 2012;37(17):1490–6.
Acknowledgments
The authors thank Yohei Matsuo (Department of Orthopedic Biomaterial Science, Osaka University Graduate School of Medicine) for help with interobserver agreement for evaluation of fusion status.
Conflict of interest
No funds were received in support of this work. No benefits in any form have been or will be received from a commercial party related directly or indirectly to the subject of this manuscript.
Author information
Authors and Affiliations
Corresponding author
About this article

Cite this article
Makino, T., Kaito, T., Fujiwara, H. et al. Does fusion status after posterior lumbar interbody fusion affect patient-based QOL outcomes? An evaluation performed using a patient-based outcome measure. J Orthop Sci 19, 707–712 (2014). https://doi.org/10.1007/s00776-014-0591-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00776-014-0591-6