
Abstract
Human exposure to gadolinium-based contrast agents can be complicated by nephrogenic systemic fibrosis (NSF). Demonstration of significant quantities of insoluble gadolinium in the skin of NSF patients suggested transmetallation as a mechanism of toxicity of this injury. An alternative pathway for the biological effect of gadolinium is a disruption of iron homeostasis. We tested the postulate that cell exposure to gadolinium increases iron uptake to disrupt intracellular metal homeostasis and impact inflammatory events. Alveolar macrophages, THP1 cells, NHBE cells, and BEAS-2B cells all demonstrated a capacity to import gadolinium from both GdCl3 and Omniscan. All four cell types similarly imported iron following exposure to ferric ammonium citrate (FAC). Exposure of all cell types to gadolinium and iron resulted in increased iron import relative to cell concentrations following incubation with FAC alone. To analyze for further evidence of changes in iron homeostasis, cell ferritin concentration was determined. Relative to incubation with FAC alone, co-incubation of BEAS-2B cells with gadolinium and FAC resulted in significant increases in ferritin level. Finally, potential effects of gadolinium uptake and associated changes in iron homeostasis on the inflammatory response were evaluated by measuring IL-8. Co-incubation of BEAS-2B cells with both gadolinium and iron resulted in diminished release of IL-8 relative to levels of the cytokine following incubation with gadolinium alone. We conclude that gadolinium impacts cell iron homeostasis to change import and storage of the metal and biological effects of exposure.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Human exposure to gadolinium-based contrast agents can be complicated by nephrogenic systemic fibrosis (NSF). Since the first observation of this relationship [1, 2], there have been over 200 cases of NSF reported following the use of such contrast agents [3]. NSF was initially considered a cutaneous disorder present almost exclusively in patients with end-stage renal disease and characterized by the development of (1) pruritic skin plaques over the extremities and trunk, (2) contractures of joints, and (3) loss of range of motion [4–7]. However, clinical and autopsy data now suggest that NSF is a systemic fibrogenic process that involves many tissues other than the skin, including the liver, lungs, muscles, heart, myocardium, testes, and dura [8]. Onset of the disease can vary from days to months following exposure to the contrast agent. Cases can follow multiple exposures but NSF has also been observed after a single dose [6]. The diagnosis is confirmed by a deep dermal biopsy from affected skin areas showing significant deposition of collagen, thickening of the dermis, an accumulation of histiocytes, and specific histopathologic features (e.g., identification of CD34-positive spindle cells as bone-marrow-derived fibrocytes) [4, 9]. Estimates of the prevalence of NSF are inaccurate because of underdiagnosis and underreporting [10, 11].
Demonstration of significant quantities of insoluble gadolinium in the skin of NSF patients [12] after use of a gadolinium-based contrast agent suggested that transmetallation followed gadolinium exposure. This transmetallation theory proposes that gadolinium is released from its chelating agent, imported into cells and tissues, and exchanged with other metals to affect a biological response [3]. Supporting a possible participation of transmetallation in the injury, all NSF cases reported thus far have been associated with linear contrast agents that have inferior thermodynamic stability and a kinetic or conditional stability which would favor this process [10].
An alternative mechanism to explain gadolinium toxicity in NSF is a disruption of iron homeostasis. A mobilization of host iron has been described following exposure to gadolinium-based contrast agents, with the levels of serum iron, transferrin saturation, and ferritin all increasing after the provision of Omniscan to two patients [13]. In a second study, the heart, blood vessels, and skin of three NSF patients who had died of cardiac and/or vascular complications were examined and these tissues showed significantly elevated levels of iron as well as gadolinium [14]. In support of an effect of gadolinium on iron homeostasis, other trivalent metal cations have been previously demonstrated to affect iron metabolism with significant increases in cell and tissue import [15–18]. It is proposed that increased cell and tissue concentrations of biologically active iron could result after introduction of a gadolinium-based contrast agent. Injury would be associated with elevated levels available via a catalysis of an oxidative stress (Fenton reaction). We subsequently tested the postulate that cell exposure to gadolinium increases iron uptake to disrupt intracellular metal homeostasis and impact inflammatory events.
Materials and methods
Materials
Gadolinium chloride hexahydrate and Omniscan (gadolinium diethylenetriaminepentaacetate bismethylamide) were obtained from Sigma (St. Louis, MO, USA) and GE Healthcare, respectively. Omniscan was provided as a 0.4848 M solution. Ferric ammonium citrate (FAC; Sigma) was employed in cell exposures to iron.
Cell culture
Four different cell types were employed in the studies. These included alveolar macrophages, THP1 cells, primary human bronchial epithelial cells, and BEAS-2B cells.
For the acquisition of alveolar macrophages, the protocol and consent form were approved by the University of North Carolina School of Medicine Committee on the Protection of the Rights of Human Subjects. Healthy nonsmoking volunteers (18–40 years of age) underwent fiber-optic bronchoscopy with bronchoalveolar lavage. The fiber-optic bronchoscope was wedged into a segmental bronchus of the lingula and then the right middle lobe. Aliquots of sterile saline were instilled and immediately aspirated, centrifuged, and stored at −70 °C. Macrophages from aliquots were pooled and washed twice. Incubations were in RPMI-1640 (Invitrogen, Carlsbad, CA, USA) supplemented with 10% fetal calf serum (FCS; Invitrogen, Carlsbad, CA, USA) and gentamicin solution (20 μg/ml; Sigma, St. Louis, MO, USA).
THP1 cells are derived from a monocyte-like cell line. These were cultured in 75-cm2 tissue culture flasks using RPMI-1640 (Invitrogen, Carlsbad, CA, USA) supplemented with 10% FCS (Invitrogen, Carlsbad, CA, USA) and gentamicin solution (20 μg/ml; Sigma, St. Louis, MO, USA). Incubations were in RPMI-1640 supplemented with FCS and gentamicin.
The protocol for acquiring human bronchial epithelial cells was approved by the University of North Carolina School of Medicine Committee on Protection of the Rights of Human Subjects and by the US EPA. Subjects were informed of the procedure and its potential risks, and each subject signed an informed consent form. Airway epithelial cells were obtained from healthy individuals through bronchoscopy with bronchial brushings. Cells were expanded to passage 3 in bronchial epithelial growth medium (BEGM; Clonetics, San Diego, CA, USA) and plated at a density of 1 × 105 cells/well into 12-well culture plates (Trans-CLR, Costar, Cambridge, MA, USA). The cells were maintained in BEGM with supplements. Fresh medium was provided every 48 h. Exposures were in 1.0 ml Hank’s balanced salt solution (HBSS) with calcium and magnesium. These specific cells have been employed and characterized in numerous previous studies [19, 20].
Finally, BEAS-2B cells were used. This is an immortalized line of normal human bronchial epithelium derived by transfection of primary cells with SV40 early-region genes. Cells were grown to 90–100% confluence on uncoated plastic 12-well plates in keratinocyte growth medium (KGM; Clonetics, San Diego, CA, USA), which is essentially MCDB 153 medium supplemented with 5 ng/ml human epidermal growth factor, 5 mg/ml insulin, 0.5 mg/ml hydrocortisone, 0.15 mM calcium, bovine pituitary extract, 0.1 mM ethanolamine, and 0.1 mM phosphoethanolamine. Fresh medium was provided every 48 h.
Gadolinium and iron concentrations
For gadolinium and iron uptake studies, alveolar macrophages and THP1 cells were exposed for 4 h while suspended in polypropylene tubes at 1.0 × 106 cells/1.0 ml medium (n = 4 per exposure). Human bronchial epithelial and BEAS-2B cells were cultured on 12-well plates and exposed for 4 h to metals in HBSS with calcium and magnesium included in the buffer. After the exposure was complete, alveolar macrophages and THP1 cells were centrifuged, the medium was removed, the cells were washed with HBSS twice, and 1.0 ml of 3 N HCl/10% trichloroacetic acid was added to the pellet. At the end of the exposure of both human bronchial epithelial and BEAS-2B cells to metal, the buffer was removed from the well and the cells were washed twice with HBSS. Epithelial cells were then scraped into 1.0 ml of 3 N HCl/10% trichloroacetic acid. All cells were then hydrolyzed in the acid at 70 °C for 18 h. After centrifugation at 20,800g for 5 min, gadolinium and iron concentrations in the supernatant were determined using inductively coupled plasma optical emission spectroscopy (Optima 4300D; PerkinElmer, Norwalk, CT, USA) at wavelengths of 342.247 and 238.204 nm, respectively. A multielement standard (Fisher, Pittsburgh, PA, USA) was used to calibrate the instrument. The limits of detection for gadolinium and iron were 0.1–1.0 ppb and less than 0.1 ppb, respectively. Previous investigation has confirmed intracellular transport of metal using this method [21].
Ferritin and IL-8
BEAS-2B cells were exposed to gadolinium and iron for 24 h. After completion of the exposure, the medium was removed and the cells were washed twice with HBSS. They were then scraped into 0.50 ml HBSS and disrupted using repeated aspirations through a 25-gauge needle. Ferritin concentrations in these cell lysates were determined using an enzyme immunoassay (Microgenics, Concord, CA, USA). This assay was modified for use in the Cobas Fara II centrifugal spectrophotometer (Hoffman-LaRoche, Branchburg, NJ, USA).
BEAS-2B cells were again exposed to gadolinium and iron for 24 h and the medium was taken. After centrifugation, IL-8 in the supernatant was quantified using a commercially available ELISA kit (R&D, Minneapolis, MN, USA).
Statistics
Data are expressed as mean values plus the standard error. The minimum number of replicates for all measurements was six. Differences between multiple groups were compared using one-way analysis of variance. The post hoc test employed in analysis of variance was Duncan’s multiple range test. Two-tailed tests of significance were employed. Significance was assumed at p < 0.05.
Results
Gadolinium was not detectable in any cell type prior to exposure to either GdCl3 or Omniscan. Alveolar macrophages, THP1 cells, NHBE cells, and BEAS-2B cells all demonstrated a capacity to import gadolinium from GdCl3 (Fig. 1). The buffer for the human bronchial epithelial and BEAS-2B cells (HBSS with calcium and magnesium) contained little to no transferrin; therefore, in these specific cell types, uptake was likely to be via a non-transferrin-dependent pathway. Comparable to exposure to GdCl3, incubation with Omniscan resulted in elevation of cell gadolinium concentrations (Fig. 1). In incubations with GdCl3, approximately 10–30% of the available gadolinium appeared to be imported by cells. There were differences among cell types in the uptake of gadolinium, with BEAS-2B cells showing the greatest capacity. Import of this metal by all cell types following GdCl3 exposure was significantly greater than that after Omniscan, likely reflecting the strong complexation by the diethylenetriaminepentaacetate chelate present in the latter. Cell gadolinium concentration increased linearly within the range of exposures employed; no saturation was observed.

Cell gadolinium concentration following exposure to GdCl3 and Omniscan. Alveolar macrophages (a), THP1 cells (b), bronchial epithelial cells (c), and BEAS-2B cells (d) were exposed to 0–100 μM GdCl3 and Omniscan. There was no measurable gadolinium in any cell type prior to exposure. All cell types demonstrated concentration-dependent uptake of gadolinium. Asterisk significant difference relative to cells exposed to 0 μM gadolinium
Iron was measurable in all cell types prior to exposure to FAC. Comparable to the situation with gadolinium, all four cell types similarly imported iron following exposure to FAC (Fig. 2). Those cells with the greatest capacity for iron uptake were the BEAS-2B cells. However, relative to gadolinium, far less iron was imported into any of the cells. Cell iron concentrations showed no evidence of saturation following FAC exposure.

Cell iron concentration following exposure to ferric ammonium citrate (FAC). Alveolar macrophages (a), THP1 cells (b), bronchial epithelial cells (c), and BEAS-2B cells (d) were exposed to 0–100 μM FAC for 4 h. Iron in all cells was measurable prior to exposure. All cell types demonstrated concentration-dependent uptake of iron
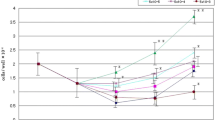
Co-incubation of cells with GdCl3 and FAC resulted in significantly elevated concentrations of cell gadolinium in alveolar macrophages and BEAS-2B cells relative to the concentrations following incubation of the cells with GdCl3 alone (Fig. 3a, d). However, no such elevations were observed in THP1 and human bronchial epithelial cells (Fig. 3b, c). Relative to cells incubated with FAC alone, the exposure of all cell types to both gadolinium and iron resulted in increased iron import (Fig. 4). Co-incubation of cells with Omniscan and FAC showed smaller elevations in cell metal concentrations; however, cell iron concentrations remained significantly increased following co-incubation.

Cell gadolinium concentration following coexposure to GdCl3 and FAC. Alveolar macrophages (a), THP1 cells (b), bronchial epithelial cells (c), and BEAS-2B cells (d) were exposed to 100 μM GdCl3 and 100 μM FAC. Relative to GdCl3 exposure alone, alveolar macrophages and BEAS-2B cells demonstrated increased uptake of gadolinium following co-incubation of GdCl3 and FAC. Single asterisk significant difference relative to cells exposed to media/buffer, double asterisk significant difference relative to cells exposed to gadolinium alone

Cell iron concentration following coexposure to GdCl3 and FAC. Alveolar macrophages (a), THP1 cells (b), bronchial epithelial cells (c), and BEAS-2B cells (d) were exposed to 100 μM GdCl3 and 100 μM FAC. Relative to exposure to FAC alone, all cell types demonstrated increased uptake of iron following co-incubation of GdCl3 and FAC. Single asterisk significant difference relative to cells exposed to medium/buffer, double asterisk significant difference relative to cells exposed to either medium or gadolinium alone, triple asterisk significant difference relative to cells exposed to iron alone
Incubation of BEAS-2B cells in 100 μM GdCl3 with increasing concentrations of FAC (0–100 μM) for 4 h was associated with increased cell import of gadolinium (Fig. 5a). In a similar manner, incubation of 100 μM FAC with various concentrations of GdCl3 (0–100 μM) was associated with elevated iron import in BEAS-2B cells (Fig. 5b). BEAS-2B cells were also exposed first to 100 μM GdCl3 for 4 h, washed twice with HBSS, and then exposed to 100 μM FAC in HBSS for 4 h. Prior gadolinium exposure increased iron import even after the GdCl3 had been removed from the buffer (data not shown).

Cell gadolinium and iron concentrations following coexposure to GdCl3 and FAC. BEAS-2B cells were all exposed to 100 μM GdCl3 and various concentrations of FAC (0–100 μM) (a). BEAS-2B cells were then exposed to 100 μM FAC and various concentrations of GdCl3 (0–100 μM) (b). Co-incubations of 100 μM FAC and 100 μM GdCl3 demonstrated the greatest cell concentration of iron. Single asterisk significant difference relative to cells exposed to 0 μM, double asterisk significant difference relative to cells exposed to 50 μM
The measurement of cell metal concentrations supported a disruption of iron homeostasis following gadolinium exposure. Cell ferritin concentration was determined to analyze for further evidence of changes in iron homeostasis. Exposure of BEAS-2B cells for 24 h to gadolinium in KGM did not show any changes in cell ferritin concentration (Fig. 6a). In contrast, incubation of the same cells with FAC in KGM for 24 h showed significantly elevated cell concentrations of ferritin (Fig. 6b). Finally, co-incubation of gadolinium and FAC was associated with significant increases in ferritin levels, relative to levels following incubation with FAC alone, likely reflecting the higher cellular iron levels (Fig. 6b).

Cell ferritin levels after exposure to FAC and co-incubation of gadolinium and FAC. BEAS-2B cells exposed to various concentrations of FAC (0–100 μM) showed increased concentrations of cell ferritin (a). Co-incubation of GdCl3 and FAC significantly increased cell ferritin levels relative to levels of this storage protein following incubation with iron alone (b). Single asterisk significant difference relative to cells exposed to 0 μM or medium/buffer, double asterisk significant difference relative to cells exposed to 50 μM FAC or iron alone
IL-8 was utilized as an end point of biological effect relevant to inflammation. IL-8 is considered proinflammatory and increases in IL-8 levels are frequently observed in tissue injuries complicated by both inflammation and fibrosis. Potential effects of gadolinium uptake and associated changes in iron homeostasis on the cell inflammatory response were evaluated by measuring IL-8 release. Exposure of BEAS-2B cells to GdCl3 for 24 h resulted in increased IL-8 release into the cell supernatant (Fig. 7). Comparable exposure of the same cell type to FAC did not show such an increase in the release of proinflammatory mediator (Fig. 7). Finally, co-incubation of gadolinium and iron resulted in diminished release of IL-8 relative to levels of the cytokine following incubation with gadolinium alone (Fig. 7).

IL-8 release after exposure to GdCl3 and co-incubation of gadolinium and FAC. BEAS-2B cells exposed to various concentrations of GdCl3 (0–100 μM) showed increased release of IL-8. Co-incubation of GdCl3 and FAC significantly decreased IL-8 release relative to levels following incubation with gadolinium alone. Single asterisk significant difference relative to cells exposed to 0 μM or medium/buffer, double asterisk significant difference relative to cells exposed to gadolinium alone
Discussion
Gadolinium concentrations in those tissues affected by NSF can range up to hundreds of parts par million (micrograms per gram of tissue) [22–24]. The highest in vitro cell exposure to gadolinium in this investigation was 100 ppm. Consequently, the concentrations employed in this in vitro investigation are considered relevant to the in vivo tissue injury.
Gadolinium significantly impacts iron homeostasis in cultured cells. Exposure of four different cell types to both GdCl3 and Omniscan increased iron import. GdCl3 incubations increased cell iron concentration to a higher value relative to Omniscan; this may reflect the stronger complexation of gadolinium by the diethylenetriaminepentaacetate in Omniscan. The inhibition of metal import by a chelator has been previously demonstrated with deferoxamine decreasing iron uptake by several cell types [25]. The molecular basis for elevations in the cell import of iron with gadolinium exposure was not determined. However, such an elevation in the uptake of non-transferrin-bound iron has also been shown after exposure to Ga3+ with gallium nitrate stimulating iron uptake in a time- and concentration-dependent manner [15]. Comparable to our investigation using Gd3+, pre-exposure of cells to gallium followed by its removal also resulted in sustained stimulation of iron uptake. Consequently, gallium and iron are considered to likely share the same cellular uptake system. Aluminum is another trivalent metal cation which has been observed to elevate iron import via non-transferrin uptake pathways [16, 18]. Comparable to Ga3+ and Al3+, divalent cations (i.e., copper and zinc) can impact iron transport to increase import [26]. However, there is an investigation which shows a lack of an effect of divalent metal cations on iron homeostasis [18]. Results of this previous investigation suggest a mechanism of transporter activation dependent on the presence of the iron atom itself or a metal ion with atomic similarities to iron (e.g., gallium) [17]. Finally, exposure to iron in specific cell types appears to have increased Gd3+ uptake, which is comparable to its increasing the import of other trivalent metal cations (e.g., gallium) via the non-transferrin-dependent pathway [15]. This increase in gadolinium import following iron co-incubation was observed in alveolar macrophages and BEAS-2B cells but not in THP1 and human bronchial epithelial cells.
To decrease oxidative stress potentially presented by iron, it benefits the host to sequester available iron. The intracellular sequestration of iron limits its potential to generate free radicals and prevents cellular injury resulting from its exposure. The storage of iron in a chemically less reactive form within intracellular ferritin confers an antioxidant function to this protein and, in certain cells, provides cytoprotection in vitro against oxidants [27, 28]. Ferritin synthesis is known to be regulated by a posttranscriptional mechanism [29, 30]. A specific sequence at the 5′-untranslated end of ferritin messenger RNA called the iron responsive element binds a cubane iron–sulfur cluster, iron regulatory protein 1 (IRP1), when it exists in the apoprotein form. Available iron reacts with IRP1 to alter its conformation. This decreases the affinity of IRP1 for the messenger RNA and it is displaced, allowing translation of ferritin to proceed. This regulation of ferritin allows the cell to respond rapidly to increased concentrations of iron by increasing the amount of metal sequestered in this protein. In our investigation, co-incubation of iron and gadolinium increased cell ferritin concentrations relative to iron exposure alone. This elevation in cell ferritin levels reflects the greater import of the metal following coexposure to the two metals. Gadolinium exposure alone did not impact cell ferritin concentration. This is comparable to the action of other trivalent metal cations (e.g., gallium) which similarly increase iron uptake into the cell but do not increase the ferritin levels themselves [31].
Finally, the effects of gadolinium on iron homeostasis could potentially impact inflammatory events. We demonstrated that cell exposure to gadolinium increased the release of IL-8 by BEAS-2B cells, whereas incubation with FAC had little effect. The co-incubation of gadolinium and FAC actually resulted in a diminished release of the inflammatory cytokine IL-8 relative to that following incubation with gadolinium alone. This diminished release of a mediator may reflect some modification in the inflammatory response after co-incubation of the two metals. Such interaction is not unique to gadolinium but also occurs following coexposure of several metals with iron [32]. This relationship between gadolinium and iron predicts a potential interaction of the two metals in clinical injury. In NSF following exposure to gadolinium-based contrast agents, iron mobilization may increase the risk of inflammatory conditions such as cardiovascular disease [33–35].
As a result of their interactions with O2, transition metals were selected in molecular evolution to carry out a wide range of biological functions. These metals are essential micronutrients utilized in almost every aspect of normal cell function. As a result of its abundance in nature, iron has a greater participation in the normal physiological processes of a living system relative to other transition metals. Those same chemical properties which allow iron to function as a catalyst in the numerous reactions of molecular oxygen also make it a threat to life via the generation of oxygen-based free radicals. Although nearly all living systems depend on iron to catalyze homeostatic and synthetic functions, oxidative stress generated by this metal has a capacity to damage biological molecules. The increased cell and tissue exposures to catalytically active iron after exposure to gadolinium-based contrast agents can potentially result in a systemic fibrosis characteristic of NSF. Prolyl and lysyl hydroxylases are enzymes which both play a central role in collagen synthesis [36]. These dioxygenases couple the oxidative decarboxylation of 2-oxoglutarate to the hydroxylation of prolyl and lysyl residues, respectively. Both enzymes use molecular oxygen as a substrate and require ascorbate and iron as cofactors [37]. Prolyl hydroxylase may not contain stoichiometric amounts of iron [38] but rather the metal is loosely bound in a non-heme form. Elevations in the concentration of available iron following gadolinium exposure with contrast use could increase the activity of prolyl and lysyl hydroxylases, resulting in collagen deposition and fibrosis. In support of a relationship between iron availability and collagen synthesis, exposure to iron chelates, such as the ferrous–bleomycin coordination complex, can directly increase prolyl hydroxylase activity [39]. In further support, iron chelators, including 2,2′-dipyridyl and deferoxamine [40–42], can inhibit prolyl hydroxylase. In contrast, dietary depletion of iron [43] and metal chelation [44] can inhibit fibrosis after exposure to such chelates.
We conclude that gadolinium impacts cell iron homeostasis to change import, storage, and biological effects of the metal. A dependence of both (1) NSF following exposure to gadolinium-based contrast agents and (2) animal models of this injury on elevated concentrations of iron can be explained by the interactions of the two metals observed in our results [1, 45]. Caution is warranted when using gadolinium-based contrast agents for patients but especially those with clinical or laboratory evidence of iron overload.
Abbreviations
- BEGM:
-
Bronchial epithelial growth medium
- FAC:
-
Ferric ammonium citrate
- FCS:
-
Fetal calf serum
- HBSS:
-
Hank’s balanced salt solution
- ICPOES:
-
Inductively coupled plasma optical emission spectroscopy
- IRP1:
-
Iron regulatory protein 1
- KGM:
-
Keritinocyte growth medium
- NSF:
-
Nephrogenic systemic fibrosis
References
Grobner T, Prischl FC (2008) Semin Dial 21:135–139. doi:10.1111/j.1525-139X.2007.00406.x
Marckmann P, Skov L, Rossen K, Dupont A, Damholt MB, Heaf JG, Thomsen HS (2006) J Am Soc Nephrol 17:2359–2362. doi:10.1681/ASN.2006060601
Graziani G, Montanelli A, Brambilla S, Balzarini L (2009) J Nephrol 22:203–207
Cowper SE, Rabach M, Girardi M (2008) Eur J Radiol 66:191–199. doi:10.1016/j.ejrad.2008.01.016
Marckmann P, Nielsen AH, Sloth JJ (2008) Nephrol Dial Transplant 23:3280–3282. doi:10.1093/ndt/gfn217
Marckmann P, Skov L, Rossen K, Heaf JG, Thomsen HS (2007) Nephrol Dial Transplant 22:3174–3178. doi:10.1093/ndt/gfm261
Morcos SK, Thomsen HS (2008) Nephron Clin Pract 110:c24–c31; discussion c32. doi:10.1159/000151228
Schroeder JA, Weingart C, Coras B, Hausser I, Reinhold S, Mack M, Seybold V, Vogt T, Banas B, Hofstaedter F, Kramer BK (2008) Clin J Am Soc Nephrol 3:968–975. doi:10.2215/CJN.00100108
Boyd AS, Zic JA, Abraham JL (2007) J Am Acad Dermatol 56:27–30. doi:10.1016/j.jaad.2006.10.048
Swaminathan S, Shah SV (2007) J Am Soc Nephrol 18:2636–2643. doi:10.1681/ASN.2007060645
Todd DJ, Kagan A, Chibnik LB, Kay J (2007) Arthritis Rheum 56:3433–3441. doi:10.1002/art.22925
Thakral C, Abraham JL (2009) J Cutan Pathol 36:1244–1254. doi:10.1111/j.1600-0560.2009.01283.x
Swaminathan S, Horn TD, Pellowski D, Abul-Ezz S, Bornhorst JA, Viswamitra S, Shah SV (2007) N Engl J Med 357:720–722. doi:10.1056/NEJMc070248
Swaminathan S, High WA, Ranville J, Horn TD, Hiatt K, Thomas M, Brown HH, Shah SV (2008) Kidney Int 73:1413–1418. doi:10.1038/ki.2008.76
Chitambar CR, Sax D (1992) Blood 80:505–511
Kim Y, Olivi L, Cheong JH, Maertens A, Bressler JP (2007) Toxicol Appl Pharmacol 220:349–356. doi:10.1016/j.taap.2007.02.001
Richardson DR (2001) Biochim Biophys Acta 1536:43–54
Sturm B, Lassacher U, Ternes N, Jallitsch A, Goldenberg H, Scheiber-Mojdehkar B (2006) Biochimie 88:645–650. doi:10.1016/j.biochi.2005.12.001
Ghio AJ, Turi JL, Madden MC, Dailey LA, Richards JD, Stonehuerner JG, Morgan DL, Singleton S, Garrick LM, Garrick MD (2007) Am J Physiol Lung Cell Mol Physiol 292:L134–L143. doi:10.1152/ajplung.00534.2005
Tal TL, Simmons SO, Silbajoris R, Dailey L, Cho SH, Ramabhadran R, Linak W, Reed W, Bromberg PA, Samet JM (2010) Toxicol Appl Pharmacol 243:46–54. doi:10.1016/j.taap.2009.11.011
Wang X, Ghio AJ, Yang F, Dolan KG, Garrick MD, Piantadosi CA (2002) Am J Physiol Lung Cell Mol Physiol 282:L987–L995. doi:10.1152/ajplung.00253.2001
Abraham JL, Thakral C, Skov L, Rossen K, Marckmann P (2008) Br J Dermatol 158:273–280. doi:10.1111/j.1365-2133.2007.08335.x
High WA, Ranville JF, Brown M, Punshon T, Lanzirotti A, Jackson BP (2010) J Am Acad Dermatol 62:38–44. doi:10.1016/j.jaad.2009.07.018
Khurana A, Greene JF Jr, High WA (2008) J Am Acad Dermatol 59:218–224. doi.10.1016/j.jaad.2008.04.010
Kicic A, Chua AC, Baker E (2001) Cancer 92:3093–3110. doi:10.1002/1097-0142(20011215)92:12<3093::AID-CNCR10107>3.0.CO;2-B
Kaplan J, Jordan I, Sturrock A (1991) J Biol Chem 266:2997–3004
Balla G, Jacob HS, Balla J, Rosenberg M, Nath K, Apple F, Eaton JW, Vercellotti GM (1992) J Biol Chem 267:18148–18153
Cozzi A, Santambrogio P, Levi S, Arosio P (1990) FEBS Lett 277:119–122
Haile DJ, Rouault TA, Harford JB, Kennedy MC, Blondin GA, Beinert H, Klausner RD (1992) Proc Natl Acad Sci USA 89:11735–11739
Leibold EA, Munro HN (1988) Proc Natl Acad Sci USA 85:2171–2175
Davies NP, Rahmanto YS, Chitambar CR, Richardson DR (2006) J Pharmacol Exp Ther 317:153–162. doi:10.1124/jpet.105.099044
Salnikow K, Li X, Lippmann M (2004) Toxicol Appl Pharmacol 196:258–265. doi:10.1016/j.taap.2004.01.003
Hansson GK (2005) N Engl J Med 352:1685–1695. doi:10.1056/NEJMra043430
Shah SV, Alam MG (2003) Am J Kidney Dis 41:S80–S83. doi:10.1053/ajkd.2003.50091
Yachie A, Niida Y, Wada T, Igarashi N, Kaneda H, Toma T, Ohta K, Kasahara Y, Koizumi S (1999) J Clin Invest 103:129–135.doi:10.1172/JCI4165
Prockop DJ (1971) Fed Proc 30:984–990
Hutton JJ Jr, Trappel AL, Udenfriend S (1966) Biochem Biophys Res Commun 24:179–184
Pankalainen M, Kivirikko KI (1971) Biochim Biophys Acta 229:504–508
Giri SN, Misra HP, Chandler DB, Chen ZL (1983) Exp Mol Pathol 39:317–326
Franklin TJ, Hales NJ, Johnstone D, Morris WB, Cunliffe CJ, Millest AJ, Hill GB (1991) Biochem Soc Trans 19:812–815
Geesin JC, Hendricks LJ, Falkenstein PA, Gordon JS, Berg RA (1991) Arch Biochem Biophys 290:127–132
Hunt J, Richards RJ, Harwood R, Jacobs A (1979) Br J Haematol 41:69–76
Chandler DB, Barton JC, Briggs DD 3rd, Butler TW, Kennedy JI, Grizzle WE, Fulmer JD (1988) Am Rev Respir Dis 137:85–89
Kennedy JI, Chandler DB, Jackson RM, Fulmer JD (1986) Chest 89:123S–125S
Hope TA, Herfkens RJ, Denianke KS, Leboit PE, Hung YY, Weil E (2009) Invest Radiol. doi:10.1097/RLI.0b013e31819343ba
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ghio, A.J., Soukup, J.M., Dailey, L.A. et al. Gadolinium exposure disrupts iron homeostasis in cultured cells. J Biol Inorg Chem 16, 567–575 (2011). https://doi.org/10.1007/s00775-011-0757-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00775-011-0757-z