
Abstract
Dual-energy X-ray absorptiometry-based hip structural analysis was performed to evaluate the effect of a bisphosphonate, minodronic acid hydrate, on the geometry of the proximal femur in Japanese patients with osteoporosis. The subjects were 103 postmenopausal patients (average age 63.9 ± 6.4 years) with primary osteoporosis. Minodronic acid hydrate was administered orally at a dose of 1 mg/day for 12 months. Significant early responses at 3–6 months after the start of administration were observed in all three regions of the proximal femur (narrow neck, intertrochanter, and shaft) in terms of bone density, geometry, and bone strength indices. The outcomes of therapy included a reduction of the internal diameter of the cortical bone (−0.1, −0.6, and −0.2% in the neck, intertrochanter, and shaft, respectively, at 12 months; not significant) and a significant increase in cortical thickness (3.1, 3.7, and 2.0% in the respective regions at 12 months). Furthermore, minodronic acid hydrate induced a significant enlargement of the cross-sectional bone area, which is related to compressive strength; a significant increase in cross-sectional moment of inertia and section modulus (SM 4.9, 5.8, and 2.9% in the neck, intertrochanter, and shaft, respectively, at 12 months; P < 0.001), which are related to the bending strength; and a significant reduction in buckling ratio (BR −3.0% (P < 0.001), −4.2% (P < 0.001), and −1.4% (P < 0.05) in the respective regions at 12 months), which reflects improved cortical stability. These findings show that minodronic acid hydrate reduces age-related endocortical bone resorption, leading to increased cortical thickness and sustained or enhanced bone strength.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Bone geometry refers to bone tissue distribution and alignment, which are critical for both the structural and biomechanical properties of bone [1]. For those parts of the skeletal system with a complex shape, such as the proximal femur, bone geometry plays a particularly important role in biomechanical assessment. In this context, the hip structure analysis (HSA) algorithm was developed for noninvasive clinical evaluation of dual X-ray absorptiometry (DXA) of the proximal femur [2]. Three prominent prospective epidemiological studies demonstrated the ability of this method to predict hip fracture using analysis of hip geometry. In a prospective case–control study of 71 women and 25 men more than 60 years old [3], the femoral neck diameter, cross-sectional moment of inertia (CSMI), and section modulus (SM) were identified as independent predictors of hip fracture risk after adjustment for bone mineral density (BMD) in both women and men. However, the contribution of these measures to hip fracture prediction over and above BMD is likely modest. A part of the Rotterdam study included 147 incident hip fracture cases in 4806 participants [4]; the geometrical parameters did not have a better discrimination than BMD, and the buckling ratio did not offer additional predictive value. Among 7474 women from the Study of Osteoporosis Fracture (SOF) with hip DXA at baseline, 635 incident hip fractures were recorded over 13 years [5]. HSA showed the geometrical parameters, and biomechanical parameters derived from them were not more able than BMD to predict hip fracture.
This limitation may be linked to the ex vivo measurement of the cross-sectional femoral neck geometry and bone density using high-resolution computed tomography (CT), which has shown that site-dependent cortical thickness and a shifted centroid are important geometrical parameters related to bone strength [6]. HSA based on the two-dimensional bone density distribution is limited to an evaluation of the morphology of the cross section of the femoral neck, including the local cortical thickness and centroid in the cross-sectional femoral neck. Moreover, the HSA program is also limited, because most of the derived geometrical parameters depend on assumptions regarding the cross-sectional shape and on fixed percentages of cortical bone, and all the parameters are derived from bone density.
The evaluation of hip fracture risk following drug intervention requires a different point of view from that taken in epidemiological studies. The purpose of a prospective epidemiological study is to identify risk factors (e.g., geometry, BMD) that have a significant association with a future fracture. In contrast, the purpose of an intervention study is to determine whether the assessment tool (i.e., HSA) can detect a change in bone geometry and density of an individual patient after treatment, and to show whether the intervention induces an enhancement of bone strength. Taking bone geometry and BMD into account may improve the accuracy of an assessment of bone strength because an antiosteoporotic drug may modify bone geometry as well as density. A treatment-induced increase in bone density that involves an overall change in bone mass, bone size, and bone mineralization also affects bone biomechanical properties. The DXA–BMD value is influenced by all these changes but does not afford a means to determine how much the medication may influence bone biomechanical properties, because an observation of elevation in bone mass/mineralization may be offset by an increase in bone size. Therefore, evaluation of changes in bone density and geometry based on simultaneous measurement of different indices is required to properly gauge the response to treatment.
Minodronic acid hydrate is a new third-generation bisphosphonate with potent pharmacological activity that has been developed in Japan. Nonclinical studies have shown that this agent is a strong inhibitor of bone resorption at low doses [7], with inhibitory effects on the reduction of bone density or strength that are comparable with those of other bisphosphonates [8, 9]. A clinical study showed that administration of minodronic acid hydrate at 1 mg/day for 12 months produced increases of 6.0% in average lumbar bone density (L2–L4) and 3.6% in total bone density of the proximal femur in Japanese postmenopausal female patients with osteoporosis [10]. This trial also provided the first evidence that minodronic acid hydrate was superior to a placebo in preventing vertebral body fracture, with 2-year cumulative incidence of vertebral body fracture of 10.4% in the treatment group and 24.0% in the placebo group, corresponding to a 59% reduction in the relative risk of vertebral body fracture over 2 years [11]. In the present study, we report the effects of minodronic acid hydrate on hip geometry in Japanese female patients with osteoporosis, the first report of HSA results in a multicenter clinical trial in Japan.
Materials and methods
Subjects
The subjects were 103 postmenopausal female ambulatory patients with osteoporosis (>45 years old; average age, 63.9 ± 6.4 years) who were enrolled at 43 centers. Osteoporosis was defined by the criteria of the Japanese Society for Bone and Mineral Research [12, 13]. The exclusion criteria have been given elsewhere [10]. The 103 patients were not selected deliberatory from the original clinical trial (n = 135). The other 32 hip DXA data cases were obtained by the previous version of the QDR4500 series, or the DXA data were not adapted for the HSA program. The characteristics of the subjects at baseline and 12 months after the start of administration are shown in Table 1, which shows the subjects in the present study were not a deliberately selected subgroup from the original clinical trial [10]. The subjects were asked to take a 1-mg minodronic acid hydrate tablet once daily for 12 months and to remain in an upright position for 30 min before the first food or beverage of the day after taking the medication. In addition to the study medication, all subjects received a 1.6-g oral dose of calcium lactate (200 mg elemental Ca) once a day after the evening meal. Vitamin D was not supplied as a supplement.
The study was conducted with consideration for the protection of subjects as outlined in the Declaration of Helsinki, and was approved by the appropriate institutional review boards. All subjects gave written informed consent before undergoing examinations or study procedures, which were conducted in compliance with Good Clinical Practice.
Methods
The BMD of the proximal femur was measured by DXA at baseline and 3, 6, 9, and 12 months after administration. All DXA devices were of the Hologic QDR Series, and each machine was adjusted for differences by calibration with standard phantoms to verify the reproducibility of the measurements within ±1.5% during the study period. DXA image data for the proximal femur were analyzed using the HSA program (Version 12.7.3.1), and all analyses were conducted by the same technician (T.T.) in the Department of Nuclear Medicine, Kawasaki Medical School.
The HSA algorithm is based on a principle first articulated by Martin and Burr [14], who demonstrated that mineral profiles created during a single photon absorptiometry bone density scan are a projection of the corresponding bone cross section and can be used to define its geometry. As described previously [2, 15, 16], the HSA algorithm derives the conventional BMD (g/cm2), the outer diameter (OD, cm), the endocortical diameter (ED, cm), the average cortical thickness (CoTh, cm), the total mineralized bone area in the cross section (CSA, cm2), the cross-sectional moment of inertia (CSMI, cm4), and the section modulus (SM, cm3) directly from the mass profiles. SM is computed as CSMI/d max, where d max (cm) is the maximum distance between the center of the mass (centroid) and the outer cortex. Another parameter, the buckling ratio (BR), is estimated as the ratio of d max to the estimated average CoTh derived from an annulus model of the cross section using the measured OD, assuming that a fixed proportion of CSA is in the cortex. CSA and SM are indices of resistance to axial compressive and bending loads, respectively, and BR is an index of susceptibility to local buckling under bending loads.
The HSA software generates profiles of pixel values traversing the proximal femur at three locations: the narrow neck (NN) across the femoral neck at its narrowest point, the intertrochanter (IT) along the angle bisector defined by the neck and shaft axes, and across the shaft at 30 mm below the most prominent portion of the lesser trochanter. To avoid variation in the visualization of the lower border of the lesser trochanter depending on the inner rotation of the hip joint, the distance from the highest part of the lesser trochanter was made constant to improve the reproducibility of bone shaft regions and to correctly determine the region of interest (ROI). At each of these locations, five parallel profiles were generated, spaced one pixel apart, proximal and distal to the three defined locations. The five profiles were averaged within each region, and the BMD, CSA, OD, ED, CoTh, CSMI, SM, and BR were reported. The reproducibility of the HSA parameters was calculated using two measurements at a 1- or 2-month interval from 30 women [age 56–86 years old (range 71.8 ± 7.6 years)] (Table 2).
Statistical analysis
For each case, the change (%) from baseline was calculated for each parameter, and summary statistics were obtained at individual time points. These data are expressed as average values and standard deviations (SD). Comparison of the findings before and after administration of minodronic acid hydrate was performed by Wilcoxon test, assuming a two-sided level of significance of 5% (P < 0.05).
Results
Changes in BMD from baseline
Percentage changes in BMD of individual femoral regions from baseline are shown in Fig. 1. The BMD significantly increased in all regions after 3–6 months administration of minodronic acid hydrate and increased by 3.2% (P < 0.001), 4.1% (P < 0.001), and 1.6% (P < 0.001) in the NN, IT, and shaft, respectively, after 12 months. The largest change was observed in the trochanteric region. The femoral BMD, geometry, and bone strength indices at baseline and 12 months are shown in Table 3.

Percentage changes from baseline of bone mineral density (BMD) in the femoral neck, trochanter, and shaft at 3, 6, 9, and 12 months of treatment. Data are shown as means ± SE (n = 103); *P < 0.05 versus baseline (Wilcoxon test). NN narrow neck, IT intertrochanter
Changes in bone geometry from baseline
Percentage changes in bone geometry from baseline are shown in Fig. 2. CSA significantly increased in all the femoral regions starting 3 months after administration and increased by 3.3% (P < 0.001), 3.9% (P < 0.001), and 2.0% (P < 0.001) in the NN, IT, and shaft after 12 months. The changes in OD from baseline were 0.1, −0.2, and 0.4% in the NN, IT, and shaft, respectively, at 12 months after administration, with none of these changes reaching a significant level, except for OD in the shaft at 12 months (P = 0.015). ED deceased from baseline by −0.1, −0.6, and −0.2% in the NN, IT, and shaft, respectively, after 12 months, showing a trend for a decrease but without significance in any region. CoTh significantly increased from baseline at 3 months after administration and increased by 3.1% (P < 0.001), 3.7% (P < 0.001), and 2.0% (P < 0.001) in the NN, IT, and shaft, respectively, after 12 months. Overall, the most significant changes were observed in IT.

Percentage changes from baseline of the cross-sectional area, outer and endocortical diameters, and cortical thickness of the femoral head, trochanter, and shaft at 3, 6, 9, and 12 months of treatment. Data are shown as means ± SE (n = 103); *P < 0.05 versus baseline (Wilcoxon test). CSA cross-sectional area, OD outer diameter, ED endocortical diameter, CoTh cortical thickness, NN narrow neck, IT intertrochanter
Changes in bone strength indices from baseline
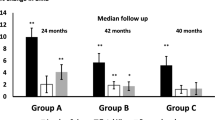
Percentage changes from baseline in CSMI, SM, and BR, all of which are bone strength indices for the femoral region, are shown in Fig. 3. CSMI and SM showed significant increases in all the femoral regions examined 3 months after administration; CSMI increased by 4.8% (P < 0.001), 4.9% (P < 0.001), and 3.2% (P < 0.001) and SM by 4.9% (P < 0.001), 5.8% (P < 0.001), and 2.9% (P < 0.001) in the NN, IT, and shaft, respectively, after 12 months. BR significantly decreased at 3 months after administration in the IT and at 6 months after administration in the NN and shaft. BR significantly decreased by −3.0% (P < 0.001), −4.2% (P < 0.001), and −1.4% (P = 0.028) in the NN, IT, and shaft, respectively, after 12 months.

Percentage changes from baseline of bone strength indices (CSMI, SM, BR) of the femoral neck, trochanter, and shaft at 3, 6, 9, and 12 months of treatment. Data are shown as means ± SE (n = 103); *P < 0.05 versus baseline (Wilcoxon test). CSMI cross-sectional moment of inertia, SM section modulus, BR buckling ratio, NN narrow neck, IT intertrochanter
As seen for BMD and the geometry indices, the effects of minodronic acid hydrate on the bone strength indices most significantly appeared in the IT, followed by the NN, and then the shaft.
Discussion
The present study demonstrates that minodronic acid hydrate, a new bisphosphonate, improves bone strength indices in the proximal femur in patients with osteoporosis. The comparison of femoral geometry and bone strength indices before and after administration allows investigation of the mechanism of drug action in the prevention of fracture. Specifically, most changes in the indices for bone density, geometry, and strength were observed in all femoral regions starting from an early stage (3–6 months) after administration of minodronic acid hydrate. The strongest effect occurred in the femoral trochanteric region as a result of the dominant action of the bisphosphonate on cancellous bone. No significant increase in the outer diameter, which is reported to typically occur with aging, was observed during the 12-month follow-up period; in contrast, it is of interest that a slight decrease in endocortical diameter (−0.1% in the NN, −0.6% in the IT, and −0.2% in the shaft) was observed, which is generally thought to increase with aging. This change might be caused by an inhibition of endocortical resorption by minodronic acid hydrate, resulting in a significantly increased CSA (3.3% in the NN, 3.9% in the IT, and 2.0% in the shaft) and CoTh (3.1% in the NN, 3.7% in the IT, and 2.0% in the shaft). The bone strength parameters calculated by the HSA algorithm include the cortical CSA as an index of strength against axial compressive load, CSMI and SM as strength indices against bending load, and BR as an index for predisposition to local buckling caused by thinned cortices. In the present study, we found a significant change in CSMI, SM (4.9% in the NN, 5.8% in the IT, and 2.9% in the shaft at 12 months), and BR (−3.0% in the NN, −4.2% in the IT, and −1.4% in the shaft at 12 months). These improvements were observed at 3 months after administration of minodronic acid hydrate, suggesting that potent inhibition of endocortical resorption results in an increase in cortical thickness so as to sustain or improve bone strength. These effects of the bisphosphonate appeared in high metabolic turnover regions such as the cancellous and endocortical bone.
A clinical study based on HSA-based assessment of the effects of alendronate (ALN) or estrogen (EST) reported the effects on SM for IT and NN to be 9.1 and 7.3%, respectively, with ALN; 5.8 and 6.9%, respectively, with EST; and 3.4 and 3.2%, respectively, with a placebo [17]. BR increased with the placebo, whereas no change or a decrease occurred with ALN or EST (P < 0.05). This study was performed in 373 women over the age of 65 years for 3 years. In the Fosamax Actonel Comparison Trial (FACT study), ALN and risedronate (RIS) were administered once weekly (70 and 35 mg/week, respectively) for 2 years, and HSA-based assessment showed that both bisphosphonates improved bone geometry [18]. ALN and RIS increased SM by 6–7% and approximately 4%, respectively, while ALN decreased BR by approximately 2% and RIS increased BR by approximately 1% in the narrow neck. It is difficult to compare the results in the present study with previous studies on bisphosphonates because of differences in the race and age of the subjects, the criteria for diagnosis of osteoporosis in patients with low bone density, and dose and administration method (daily or weekly). However, prominent effects of minodronic acid hydrate were observed that were similar to those reported for other bisphosphonates.
The current study has the limitation that no control group was included; however, the multicenter design should help to limit any bias in the findings. Furthermore, several previous papers have reported there are no positive effects on HSA parameters in the placebo group receiving calcium supplementation at 1 year [19–22]. Data were collected for 1 year, and the effects of the agent may increase over a 2-year time-course based on changes in bone biomarkers and bone density [10, 11]. The beneficial effect on hip BMD is thought to be an important preventative factor for not only hip fracture but also vertebral fractures [23], and the early significant effects on hip BMD and HSA parameters are thought to be important for the near term as well as a longer-term preventive effect. The next few years of follow-up, to observe the incidence of hip fracture in the HSA-based assessment of intervention studies, will ultimately reveal whether geometry derived by HSA effectively serves as a surrogate marker of hip fracture. In fact, a review of reports using HSA in evaluation of the efficacy of antiosteoporotic agents [17–22] suggests that potent increase in bone strength indices derived from HSA does have an association with reduction in the incidence of hip fracture [24–26].
Previous HSA-based studies of bisphosphonate effects on the proximal femur have only included Caucasian patients. As there may be a racial difference in hip geometry, bone size, and bone density, HSA results might differ among races. Only one study using HSA assessment in Japanese patients has been performed to investigate the effects of an antiosteoporotic agent (raloxifene) [27], and therefore our study provides the first multicenter evidence of the efficacy of a bisphosphonate on hip geometry in a Japanese population. We conclude that minodronic acid hydrate may prevent hip fracture by inhibiting aging-related endocortical resorption, resulting in increased cortical thickness and improved bone strength indices in the proximal femoral region.
References
Yoshikawa T, Turner CH, Peacock M, Slemenda CW, Weaver CM, Teegarden D, Markwardt P, Burr DB (1994) Geometric structure of the femoral neck measured using dual-energy X-ray absorptiometry. J Bone Miner Res 9:1053–1064
Beck TJ, Ruff CB, Warden KE, Scott WW Jr, Rao GU (1990) Predicting femoral neck strength from bone mineral data. A structural approach. Invest Radiol 25:6–18
Ahlborg HG, Nguyen ND, Nguyen TV, Center JR, Eisman JA (2005) Contribution of hip strength indices to hip fracture risk in elderly men and women. J Bone Miner Res 20:1820–1827
Rivadeneira F, Zillikens MC, De Leat CE, Hofman A, Uitterlinden AG, Beck TJ, Pols HA (2007) Femoral neck BMD is a strong predictor of hip fracture susceptibility in elderly men and women because it detects cortical bone instability: the Rotterdam study. J Bone Miner Res 22:1781–1790
Kaptoge S, Beck TJ, Reeve J, Stone KL, Hiller TA, Cauley JA, Cummings SR (2008) Prediction of incident hip fracture risk by femur geometry variables measured by hip structural analysis in the study of osteoporotic fractures. J Bone Miner Res 23:1892–1904
Mayhew P, Kaptoge S, Loveridge N, Power J, Kroger HP, Parker M, Reeve J (2004) Discrimination between cases of hip fracture and controls is improved by hip structural analysis compared to areal bone mineral density. An ex vivo study of the femoral neck. Bone (NY) 34:352–361
Mori H, Kayasuga R, Tanaka M, Kawabata K, Nozaki K, Mori M, Sasamata M (2008) Inhibitory effect of minodronic acid on bone resorption in vitro and in vivo. Clin Pharmacol Ther 18:S19–S32
Tanaka M, Mori H, Kayasuga R, Ochi Y, Kawada N, Yamada H, Kishikawa K (2008) Long-term minodronic acid (ONO-5920/YM529) treatment suppresses increased bone turnover, plus prevents reduction in bone mass and bone strength in ovariectomized rats with established osteopenia. Bone (NY) 43:894–900
Mori H, Tanaka M, Kayasuga R, Masuda T, Ochi Y, Yamada H, Kishikawa K, Ito M, Nakamura T (2008) Minodronic acid (ONO-5920/YM529) prevents decrease in bone mineral density and bone strength, and improves bone microarchitecture in ovariectomized cynomolgus monkeys. Bone (NY) 43:840–848
Hagino H, Nishizawa Y, Sone T, Morii H, Taketani Y, Nakamura T, Itabashi A, Mizunuma H, Ohashi Y, Shiraki M, Minamide T, Matsumoto T (2009) A double-blinded head-to-head trial of minodronate and alendronate in women with postmenopausal osteoporosis. Bone (NY) 44:1078–1084
Matsumoto T, Hagino H, Shiraki M, Fukunaga M, Nakano T, Takaoka K, Morii H, Ohashi Y, Nakamura T (2009) Effect of daily oral minodronate on vertebral fractures in Japanese postmenopausal women with established osteoporosis: a randomized placebo-controlled double-blind study. Osteoporos Int 20(8):1429–1437
Orimo H, Sugioka Y, Fukunaga M, Muto Y, Hotokebuchi T, Gorai I, Nakamura T, Kushida K, Tanaka H, Ikai T, Oh-hashi Y, The Committee of the Japanese Society for Bone and Mineral Research for Development of Diagnosis Criteria of Osteoporosis (1998) Diagnostic criteria of primary osteoporosis. J Bone Miner Metab 16:139–150
Orimo H, Hayashi Y, Fukunaga M, Sone T, Fujiwara S, Shiraki M, Kushida K, Miyamoto S, Soen S, Nishimura J, Oh-Hashi Y, Hosoi T, Gorai I, Tanaka H, Igai T, Kishimoto H, Osteoporosis Diagnostic Criteria Review Committee: Japanese Society for Bone and Mineral Research (2001) Diagnostic criteria for primary osteoporosis: year 2000 revision. J Bone Miner Metab 19:331–337
Martin RB, Burr DB (1984) Non-invasive measurement of long bone cross-sectional moment of inertia by photon absorptiometry. J Biomech 17:195–201
Beck TJ (2007) Extending DXA beyond bone mineral density: understanding hip structure analysis. Curr Osteoporos Rep 5:49–55
Beck T (2003) Measuring the structural strength of bones with dual-energy X-ray absorptiometry: principles, technical limitations, and future possibilities. Osteoporos Int 14:S81–S88
Greenspan SL, Beck TJ, Resnick NM, Bhattacharya R, Parker RA (2005) Effect of hormone replacement, alendronate, or combination therapy on hip structural geometry: a 3-year, double-blind, placebo-controlled clinical trial. J Bone Miner Res 20:1525–1532
Bonnick SL, Beck TJ, Cosman F, Hochberg MC, Wang H, de Papp AE (2009) DXA-based hip structural analysis of once-weekly bisphosphonate-treated postmenopausal women with low bone mass. Osteoporos Int 20:911–921
Beck TJ, Stone KL, Oreskovic TL, Hochberg MC, Nevitt MC, Genant HK, Cummings SR (2001) Effects of current and discontinued estrogen replacement therapy on hip structural geometry: the study of osteoporotic fractures. J Bone Miner Res 16:2103–2110
Uusi-Rasi K, Semanick LM, Zanchetta JR, Bogado CE, Eriksen EF, Sato M, Beck TJ (2005) Effects of teriparatide [rhPTH (1–34)] treatment on structural geometry of the proximal femur in elderly osteoporotic women. Bone (NY) 36:948–958
Uusi-Rasi K, Beck TJ, Semanick LM, Daphtary MM, Crans GG, Desaiah D, Harper KD (2006) Structural effects of raloxifene on the proximal femur: results from the multiple outcomes of raloxifene evaluation trial. Osteoporos Int 17:575–586
Beck TJ, Lewiecki EM, Miller PD, Felsenberg D, Liu Y, Ding B, Libanati C (2008) Effects of denosumab on the geometry of the proximal femur in postmenopausal women in comparison with alendronate. J Clin Densitom 11:351–359
Bauer DC, Black DM, Garnero P, Hochberg M, Ott S, Orloff J, Thompson DE, Ewing SK, Delmas PD, for the Fracture Intervention Trial Study Group (2004) Change in bone turnover and hip, non-spine, and vertebral fracture in alendronate-treated women: the Fracture Intervention Trial. J Bone Miner Res 19:1250–1258
Black DM, Thompson DE, Bauer DC, Ensrud K, Musliner T, Hochberg MC, Nevitt MC, Suryawanshi S, Cummings SR, Fracture Intervention Trial (2000) Fracture risk reduction with alendronate in women with osteoporosis: the Fracture Intervention Trial. FIT Research Group. J Clin Endocrinol Metab 85:4118–4124
Black DM, Cummings SR, Karpf DB, Cauley JA, Thompson DE, Nevitt MC, Bauer DC, Genant HK, Haskell WL, Marcus R, Ott SM, Torner JC, Quandt SA, Reiss TF, Ensrud KE (1996) Randomised trial of effect of alendronate on risk of fracture in women with existing vertebral fractures. Fracture Intervention Trial Research Group. Lancet 348:1535–1541
McClung MR, Geusens P, Miller PD, Zippel H, Bensen WG, Roux C, Adami S, Fogelman I, Diamond T, Eastell R, Meunier PJ, Reginster JY, Hip Intervention Program Study Group (2001) Effect of risedronate on the risk of hip fracture in elderly women. Hip Intervention Program Study Group. N Engl J Med 344:333–340
Takada J, Beck TJ, Miki T, Imanishi Y, Nakatsuka K, Wada H, Naka H, Iba K, Yoshizaki T, Yamashita T (2008) Hip structure analysis for raloxifene treatment in Japanese women with osteoporosis. J Bone Miner Res 23(Suppl 1):S211
Acknowledgments
We express our gratitude to Dr. Tatsushi Tomomitsu, the Department of Nuclear Medicine, Kawasaki Medical School, for his help with the HSA-based assessment. Pacific Edit reviewed the manuscript before submission.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Ito, M., Sone, T. & Fukunaga, M. Effect of minodronic acid hydrate on hip geometry in Japanese women with postmenopausal osteoporosis. J Bone Miner Metab 28, 334–341 (2010). https://doi.org/10.1007/s00774-009-0138-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00774-009-0138-7