
Abstract
Elevated cortisol during pregnancy is associated with adverse birth outcomes and may alter fetal development and subsequent adult health. Numerous studies link elevated cortisol to depression and anxiety, but only a few have examined these relationships during pregnancy and in response to laboratory stressors. No studies have investigated the impact of comorbid anxiety and depression on cortisol during pregnancy. Salivary cortisol samples were collected twice before and once after a set of computer-based tasks (Stroop color-word matching task and either mental arithmetic or a controlled breathing task) from 180 pregnant women at approximately 36 weeks gestation. Based on psychiatric diagnoses, four groups of women were compared: 121 control, 16 depression, 34 anxiety, and 9 comorbid. Women also completed symptom and stress self-report scales. There was a significant main effect for maternal diagnosis on cortisol levels. Post hoc comparisons showed that comorbid subjects had higher salivary cortisol levels than controls, but subjects with only one diagnosis did not. Similar to cortisol, the comorbid subjects also had higher ratings on pregnancy-specific distress. Comorbidity during pregnancy, versus depression or an anxiety disorder alone, is uniquely associated with elevated cortisol and a negative evaluation of pregnancy. The potential impact of this combined psychiatric diagnosis on fetal development and future adult health needs further investigation.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The developing fetus and its placental interface are susceptible to changes mediated by the experiences of the mother. Maternal hypothalamic-pituitary-adrenal (HPA) axis activity during pregnancy is one factor that can alter fetal development and subsequent physical and mental health outcomes in the adult (for reviews, see Seckl 2001, Seckl and Meaney 2004, and Clark 1998). Elevated maternal cortisol is associated with decreased fetal size, lowered birth weight, and premature birth in humans (Diego et al. 2006; Field et al. 2006; Sandman et al. 2006). In animals, a number of studies show poor physical outcomes in adults who had increased fetal exposure to glucocorticoids. For example, administration of dexamethasone (a synthetic glucocorticoid that freely crosses the placenta) to pregnant rats results in offspring with elevated blood pressure as adults (Benediktsson et al. 1993). In humans, a direct link between elevated maternal glucocorticoids and later problems in the offspring has yet to be clearly demonstrated, although a number of epidemiological studies show associations between small birth size and health problems in adulthood such as hypertension and insulin resistance (Seckl 2001).
Psychiatric disorders are known to be associated with raised cortisol concentrations. Depression in the non-pregnant state is associated with increased cortisol levels (Carroll 1976; Carroll et al. 1976; Siever et al. 1984; Halbreich et al. 1985; Dinan 1994). During pregnancy, depression, as determined by self-report questionnaires in two reports, also is linked to higher basal cortisol levels in both the second and third trimesters compared to controls (Lundy et al. 1999; Field et al. 2004). Another study showed similar associations but the method of determining diagnosis is not described (Diego et al. 2004). To our knowledge, only one study examining cortisol in adult pregnant women used a diagnostic interview to classify depressed subjects for comparison to non-depressed subjects. That study showed that women meeting criteria for depression had elevated cortisol, however women comorbid for depression and anxiety disorders were included in the depression group (Field et al. 2007).
Three anxiety disorders — panic, obsessive compulsive (OCD), and generalized anxiety (GAD) — also are associated with elevated basal cortisol levels in adults (Roy-Byrne et al. 1986; Goldstein et al. 1987; Gehris et al. 1990; Catapano et al. 1992; Monteleone et al. 1994; Abelson and Curtis 1996; Monteleone et al. 1997, 1998; Tafet et al. 2001; Kluge et al. 2007). The evidence, however, is not quite as strong as with depression since some studies have shown cortisol levels equal to those in controls for all three disorders (Holsboer et al. 1987; Uhde et al. 1988; Hoehn-Saric et al. 1991; Maes et al. 1994; Millet et al. 1998). Comparisons of cortisol levels in pregnant women with panic disorder, OCD, and GAD to controls have not been reported; nevertheless, the association of three anxiety disorders with elevated basal cortisol suggests that anxiety disorders during pregnancy may also be associated with elevated cortisol. In contrast to these anxiety disorders, posttraumatic stress disorder (PTSD) is consistently linked to lower basal and 24-hour cortisol levels compared to controls (Yehuda et al. 1990, 1995, 1996). In pregnancy, research has shown that PTSD continues to be associated with low basal cortisol levels (Seng et al. 2005; Brand et al. 2006).
In the present study, we hypothesized that compared to healthy controls, pregnant women with depression and/or an anxiety disorder would have elevated salivary cortisol levels across all time points in a laboratory session. To separate the effects of depression and anxiety on cortisol, women with these two types of disorders were placed in separate groups and women comorbid for both depression and anxiety were assigned to a third group. The comorbid group allowed us to assess potential additive effects of depression and anxiety on cortisol levels as has been seen in non-pregnant individuals previously (Kathol et al. 1988) while also removing the difficulty of determining whether to place comorbid subjects in the depression group or in the anxiety group.
For this study, pregnant women underwent a psychiatric evaluation using a diagnostic interview during the second trimester and a psychophysiological assessment with two computer tasks and repeated salivary cortisol sampling in the third trimester. Obtaining multiple cortisol assays allowed us to assess differences in overall levels of cortisol, which was important since elevated cortisol levels during pregnancy have been linked to adverse outcomes in the infant and possibly the adult (Clark 1998; Seckl 2001; Seckl and Meaney 2004; Diego et al. 2006; Field et al. 2006; Sandman et al. 2006). In addition, even though several studies indicate that acute cortisol reactivity to laboratory stressors such as the cold pressor test and white noise may be blunted during pregnancy (Hartikainen-Sorri et al. 1991; Kammerer et al. 2002; Saisto et al. 2004), use of laboratory challenge tasks and repeated measures of cortisol enabled us to examine differences in reactivity to other stressors. As surmised in a review article by de Weerth and Buitelaar (2005), although stress reactivity may be blunted in pregnancy, there is substantial inter-individual variability in the results, as indicated by large standard deviations, some of which may be associated with psychiatric disorders and psychosocial functioning.
Materials and methods
Subjects
Two-hundred seventy-three women between the ages of 18 and 40 with singleton fetuses were recruited from clinics affiliated with Columbia University Medical Center between July 1999 and March 2006 via flyers and waiting room announcements that stated we were looking for pregnant volunteers. Subjects were recruited as part of a larger study investigating fetal and infant development in relation to women’s psychiatric and physiological profiles during pregnancy, including patterns of cortisol activity and reactivity. Women were excluded from the study if they smoked during pregnancy, were taking any medications including psychotropic ones, or if there were any maternal or fetal complications including hypertension, diabetes mellitus, or suspected fetal growth restriction. Additionally, cases were excluded because they (1) provided saliva samples that were insufficient in quantity for cortisol analysis at one or more of the three collection points (n = 49), (2) they refused to submit a sample (n = 2), or (3) data were lost due to equipment problems or experimenter error (n = 10). Women who gave birth before 37 weeks gestation (n = 8) also were excluded from all analyses, as were women whose gestational age at birth could not be determined from electronic medical records (n = 3). Since we were primarily interested in diagnoses that potentially raise cortisol levels, women with PTSD (n = 16) were excluded from all analyses so as not to mask any elevations in cortisol in the comorbid and anxiety groups. Subjects with bipolar depression (n = 3) also were excluded in an effort to reduce variability in the depression group.
Of the remaining 182 women, 60% were Latina, 19% were Caucasian, 10% were African American, 5% were Asian, and 6% were of another or mixed ethnicity. Women’s age was (mean ± SD) 26.3 ± 6.0 years. Twenty-six percent of subjects had an annual household income between $0 and $15,000, 17% between $16,000 and $25,000, 21% between $26,000 and $50,000, 19% between $51,000 and $99,000, 12% between $100,000 and $250,000, 2% above $250,000, and 3% declined to answer. Forty-five percent of subjects were married. Women in this study had babies with a mean birth weight of 3,368 ± 36 grams and a mean gestational age of 39.7 ± 0.08 weeks. Forty-nine percent of the babies were female, and for 57% of the subjects, this was their first live delivery. This study was approved by the New York State Psychiatric Institute Institutional Review Board. All subjects gave written, informed consent.
Procedures
During the second trimester, subjects came to the laboratory at Columbia University Medical Center and underwent a psychiatric interview with a psychologist using the Scheduled Clinical Interview for DSM-IV Axis I Disorders (SCID; First et al. 1997). Based on this assessment, each woman was placed in one of the four following groups: control if she had no current Axis I diagnosis (n = 123), depression if she had a current major depressive disorder episode or dysthymia (n = 16), anxiety if she had one or more current anxiety disorders (n = 34), or comorbid if she currently met criteria for both a depressive and an anxiety disorder (n = 9). (Of the 61 total subjects excluded from the study because of inadequate saliva samples, refusal to submit saliva samples, or experimenter error, 31 had no psychiatric diagnosis, 7 were depressed, 8 were comorbid, and 15 had anxiety disorders. Of the 49 subjects with inadequate saliva samples, 26 had no diagnosis, 3 were depressed, 8 were comorbid, and 12 had anxiety disorders.) Women who met criteria for a psychiatric diagnosis were referred for treatment.
At approximately 36 weeks gestation (33–39 weeks), subjects returned to the laboratory to complete self-report scales, participate in a psychophysiology recording session, and to give cortisol samples. All laboratory visits began between 10:30 and 11:30 am to control for diurnal variations in salivary cortisol levels. Once consent was obtained, women completed symptom and stress self-report scales including the Center for Epidemiological Studies Depression Scale (CES-D; Radloff 1977), the State-Trait Anxiety Inventory (STAI; Spielberger 1983), the Perceived Stress Scale (PSS; Cohen et al. 1983) and the Pregnancy Experience Scale (PES), which evaluates pregnancy-specific hassle frequency, hassle intensity, uplift frequency, uplift intensity, and a composite score of hassle intensity divided by uplift intensity (such that a larger number indicates a more negative overall evaluation of pregnancy) (DiPietro et al. 2002, 2004). Convergent and discriminant validity of the PSS has been established by comparison with other self-report data on depression and anxiety. The internal scale reliability is high (Cronbach’s alpha 0.91 to 0.95) and the frequency and intensity scores on the PES have been found to be stable over the course of pregnancy (DiPietro et al. 2004).
At the start of the psychophysiology assessment, subjects received instructions, practiced the laboratory stress tasks they would encounter in the session, and were outfitted with physiological recording equipment for ECG, blood pressure, respiration, and fetal heart rate collection. The psychophysiological recording sessions were as follows: 5 min quiet rest period, 5 min Stroop task, 5 min quiet rest period, 5 min laboratory task (mental arithmetic or paced breathing), and 5 min rest period. Subjects were asked to refrain from talking during the psychophysiology session except when asked to appraise their stress level on a scale from 1 to 10 at the end of each rest or stress period. Salivary cortisol was collected at three time points during the laboratory visit — after the subject arrived and consent was obtained (baseline), just before the psychophysiology recording session started but after a brief practice of the forthcoming tasks (anticipation), and just after the psychophysiology recording session ended (reaction) — with approximately 25 to 30 min between each sample. Subjects were instructed to suck and chew on a cotton roll for 1 min or until saturated.
Each subject completed two of the following computer-based laboratory tasks during the psychophysiological recording session: the Stroop task and either a mental arithmetic task or a controlled breathing task. Based on prior findings in a different sample of subjects, it was determined that the arithmetic task caused less physiological arousal in pregnant women than the Stroop as measured by blood pressure and heart rate changes from the prior resting period (Monk et al. 2001). As a result, an alternative to the mental arithmetic task was added to the protocol, paced breathing, which was chosen to examine maternal and fetal reactivity to rapid alterations in women’s breathing rate. Each of the three tasks used during the psychophysiological session are described below.
Stroop
The Stroop task presents subjects with color words in either congruently or incongruently colored letters and asks the subject to identify the color of the letters. It is commonly used to induce stress in a laboratory setting or as a cognitive assessment of executive function. In our version, the subject was required to push keys that corresponded to the correct color responses, and the computer indicated if the subject’s responses were “correct” or “incorrect” on the screen.
Mental arithmetic
The mental arithmetic task requires subjects to subtract serial 7s from a large number shown on the computer screen without the use of pen and paper. This task is commonly used as a stressor or as a cognitive assessment of concentration.
Paced breathing
Paced breathing requires subjects to control their breathing by inhaling when a bar on the computer screen rises and to exhale when it falls. During the task, subjects alternate between periods of breathing at a faster than normal rate, approximately 30 breaths per minute, a slower than normal rate, about 10 breaths per minute, and at an approximately normal rate, 20 breaths per minute. As paced by the computer, the breathing rates change every 30–60 s.
Salivary cortisol analyses
Cortisol samples were analyzed at the Analytical Psychopharmacology Laboratories at the Nathan Kline Institute. After denaturation of the binding proteins by heat, salivary cortisol was measured by radioimmunoassay using primary antibodies (raised in rabbit against cortisol-3-0-carboxymethyloxime-BSA) and I125 labeled cortisol purchased from ICN Biomedicals. The cortisol standards used were from Sigma Chemical. Anti-rabbit globulin serum in conjunction with polyethylene glycol was used for separation of the bound and free fractions. Samples were assayed in duplicate. The intra- and interassay coefficient of variation was 2.95% and 6.0% at the 3.1 ug/dL level, 2.53% and 3.93% at the 19.3 ug/dL level, and 2.00% and 2.91% at the 32.7 ug/dL level.
Statistical analyses
Before initiating statistical analyses to test our main hypothesis, outliers were removed from the data set. Two subjects (both from the control group) were found to have cortisol levels greater than 5 SD above the mean at one or more time points and were excluded from the analyses. Thus, all of the cortisol related analyses were run with a total of 180 subjects.
We hypothesized that pregnant women with depression, anxiety, or both diagnoses would have elevated salivary cortisol levels across all time points when compared to controls. To test for group differences and the effects of the three laboratory time points on cortisol, we used repeated measures ANOVA with the four diagnosis groups (control, depression, comorbid, and anxiety) as the between-subjects factor. We followed this with planned post hoc comparisons between controls and each diagnosis group via two-sided Dunnett t tests. Significance levels for within-subjects comparisons of cortisol levels over time use the Huynh-Feldt correction.
We followed our primary analyses with a number of secondary analyses to identify potential confounding factors contributing to our initial results. Using one-way ANOVAs we compared diagnosis groups with regard to maternal age, maternal education level, parity, gestational age at the time of assessment, and number of weeks before birth. We also examined ethnic group, income group, marital status, and second laboratory task (mental arithmetic or paced breathing) as categorical variables in relation to diagnosis group using Pearson chi-square tests. Finally we ran a t test to examine the subjective stress levels caused by the two secondary laboratory tasks (either mental arithmetic or paced breathing) and another repeated measures ANOVA to examine the differential effects of these two tasks in relation to diagnostic status on cortisol levels. After these secondary analyses, further analyses were run to incorporate the significant covariates and to make group contrasts.
A third set of analyses using one-way ANOVAs was utilized to look for self-reported psychometric corollaries (i.e. STAI state anxiety) to the diagnosis group differences that we uncovered in our sample. Post hoc two-sided Dunnett t tests were used to compare each diagnosis group to the control group and to determine if diagnostic group differences in the self-report scales paralleled group differences in cortisol.
Results
Diagnosis group and cortisol
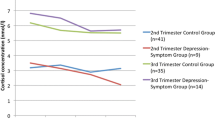
A between-subjects effect for diagnosis group was found on cortisol levels with the initial repeated measures ANOVA (F(3, 176) = 3.98, p = 0.009). Two-sided Dunnett t tests comparing the control group to each diagnostic group revealed that comorbid subjects had significantly higher salivary cortisol levels than controls (p = 0.006) but depressed and anxious subjects did not differ significantly from controls (p = 1.00 and 0.67, respectively). Figure 1 illustrates the salivary cortisol estimated marginal means for the four groups across the three time points. Using Huynh-Feldt corrected degrees of freedom, there was no significant within-subjects effect for time point on cortisol (F(1.5, 270.6) = 1.44, p = 0.24) nor a significant interaction effect of time by diagnosis (F(4.6, 270.6) = 1.05, p = 0.39).

Mean cortisol (and SE) over three time points in a laboratory session. Controls are represented by circles, depression by squares, comorbid by inverted triangles, and anxiety disorders by upright triangles
Potential confounds
Demographics
Descriptive statistics and one-way ANOVA results for each diagnosis group regarding maternal age, maternal education level, parity, gestational age at assessment, and number of weeks before birth are given in Table 1. As can be seen in this table, maternal age significantly differed across diagnosis groups in a one-way ANOVA (F(3, 176) = 4.07, p = 0.008) as well as maternal education level (F(3, 175) = 7.99, p < 0.001). Parity, gestational age at assessment, and weeks before birth did not differ. Post-hoc Dunnett t tests revealed that depressed subjects were significantly younger than controls (p = 0.05) and that all diagnostic groups (depression, comorbid, and anxiety) had fewer years of education than controls (p = 0.01, p = 0.01, p = 0.001, respectively). Since maternal age and education level significantly differed between diagnostic groups, we ran an ANCOVA examining group differences in cortisol including these two covariates. Our results did not differ –— a significant between-subjects effect for diagnosis group on cortisol level was found (F(3, 170) = 3.79, p = 0.01). Neither maternal age (F(1, 170) = 2.77, p = 0.10) nor education (F(1, 170) = 0.77, p = 0.38) was found to be significant a covariate.
In chi-square tests, ethnic group was significantly different across diagnosis groups (Χ 2 (9) = 18.39, p = 0.03) but income group (Χ 2 (15) = 15.05, p = 0.45) and marital status (Χ 2 (3) = 1.44, p = 0.70) were not. Upon examination, it was concluded that all depressed women and nearly all (seven out of nine) of the comorbid women were Latina. To ensure that the cortisol results did not simply reflect ethnic differences in our subject groups, a subsequent repeated measures ANCOVA was completed with only Latina subjects (n = 110) across all diagnostic groups (68 control, 15 depressed, 7 comorbid, and 20 anxiety subjects). When only Latina subjects were examined using a 4 × 3 (diagnosis group, cortisol repeated measures) ANCOVA design with maternal age and education level as covariates, the significant between-subjects effect for diagnosis group remained (F(3, 102) = 4.47, p = 0.005). Maternal age was determined to be a significant covariate F(1, 102) = 6.93, p = 0.01) but maternal education level was not F(1, 102) = 1.27, p = 0.26).
Effects of paced breathing versus mental arithmetic
Subjective stress ratings indicated that the arithmetic task was perceived to be more stressful than paced breathing (t (176) = 10.4, p < 0.0001). However, as determined by a repeated measures ANOVA, the second laboratory task (mental arithmetic versus paced breathing) did not differentially affect overall cortisol levels (F(1, 178) = 1.44, p = 0.23). A chi-square test indicated that there was no difference in the second laboratory task assignment related to diagnostic group status (Χ 2 (3) = 2.32, p = 0.51). To determine that in the context of diagnostic group there was no difference between task effects, a 4 × 2 × 3 (diagnosis group, secondary laboratory task, cortisol repeated measures) ANCOVA with maternal age and education level as covariates was completed. The results still showed a significant between-subjects effect for diagnosis group (F(3, 166) = 4.22, p = 0.007). A between-subjects main effect for the second laboratory task (F(1, 166) = 3.88, p = 0.05) was also found, with higher overall cortisol levels appearing to be associated with the paced breathing task. However, no between-subjects diagnosis by secondary task interaction effect was evident (F(3, 166) = 0.60, p = 0.61). Neither maternal age nor education level was found to be a significant covariate (F(1, 166) = 2.45, p = 0.12 and F(1, 166) = 0.83, p = 0.36, respectively).
Psychometric corollaries
One-way ANOVAs revealed significant differences across diagnosis groups for the self-report scales of state anxiety (F(3, 174) = 4.10, p = 0.008), trait anxiety (F(3, 174) = 6.25, p = 0.0005), depression (F(3, 172) = 10.60, p < 0.0001), perceived stress (F(3, 172) = 6.76, p = 0.0002), pregnancy-specific uplift frequency (F(3, 160) = 3.15, p = 0.03), and the PES composite score computed as the ratio of hassle intensity to uplift intensity (F(3, 160) = 9.39, p < 0.0001). No significant difference across groups was found for pregnancy-specific hassle frequency (F(3, 160) = 0.50, p = 0.68) but trends towards significance were noted for pregnancy-specific hassle intensity (F(3, 160) = 2.30, p = 0.08) and uplift intensity (F(3, 160) = 2.22, p = 0.09). Table 2 contains descriptive statistics and indicates which of the two-sided Dunnett t tests comparisons between diagnosis groups and controls were significant for the self-report mood and symptom scores. Table 3 contains similar statistics for the self-report scores specific to pregnancy. Compared to controls, the comorbid, but not the anxiety and depression groups, scored higher on hassle intensity, lower on uplift frequency, and higher on a composite score of hassles to uplifts (using Dunnett t tests; p = 0.03, p = 0.02, and p < 0.0001, respectively).
Discussion
Late in pregnancy, women comorbid for depression and anxiety had higher salivary cortisol levels than controls at three time points during laboratory sessions involving three types of challenges. In contrast, subjects with a diagnosis of either depression or anxiety disorder alone did not differ from controls. This difference in cortisol levels between comorbid subjects and controls remained even when maternal age and education were added as covariates and when only Latinas, a group overly represented in the depression and comorbid groups, were included in the analyses. Groups did not show significant cortisol changes to the laboratory stressors.
When the nature of the second laboratory task (mental arithmetic versus paced breathing) was entered into the analysis with diagnosis group and with maternal age as a covariate, an effect for secondary task was found with higher cortisol levels being associated with the paced breathing task. However, there was no significant interaction between the second laboratory task and diagnosis group.
Our results are somewhat counter to earlier findings in that our pregnant depressed subjects without a comorbid anxiety disorder do not have higher cortisol levels than controls. However, these differences in results may stem largely from variation in methodology. Two previous studies showing elevated cortisol in depressed pregnant women compared to controls used the CES-D with a score of 16 or greater to classify women as depressed rather than a diagnostic interview (Lundy et al. 1999; Field et al. 2004). Although using a questionnaire to determine diagnostic status is more time-efficient than an interview, specificity is lost. Individuals with other diagnoses can score high on a self-report depression scale; additionally, other psychiatric diagnoses, which are commonly comorbid with depression, are not assessed. Our own data (Table 2) indicate that the mean CES-D depression scores for all three groups of women with psychiatric diagnoses, including those with only an anxiety diagnosis, exceed the traditional depression cutoff of 16. It is therefore possible that in these studies, subjects with comorbid anxiety disorders were driving the elevated cortisol results and the findings are thus consistent with ours (Lundy et al. 1999; Field et al. 2004). In the one study that used a diagnostic interview to classify and compare cortisol in depressed and non-depressed subjects, which also found elevated cortisol in the depressed group, individuals comorbid for anxiety disorders were included in the depression group, and the percentage of comorbid subjects was not stated (Field et al. 2007). As with the two studies using self-report questionnaires to determine a depression diagnosis, in this report the specific diagnosis or diagnoses actually linked to elevated antenatal cortisol levels remain unclear. Finally, another study linking depression to elevated cortisol during pregnancy did not indicate diagnostic methods or exclusions and thus associations between specific diagnostic classifications and higher cortisol are unknown (Diego et al. 2004). The discrepancies in study results in the context of variation in methodology suggest that it is possible that the greater specificity of the psychiatric interview enabled us to determine the unique association of elevated maternal cortisol and depression when there is also comorbid anxiety. Comorbid anxiety and depression in non-pregnant individuals has previously been associated with cortisol levels above those seen in subjects with only one class of psychiatric disorder (Kathol et al. 1988). Given the potential clinical significance of elevated maternal cortisol for fetal development, further studies are needed to confirm that this is the form of maternal mood dysregulation most associated with increased cortisol levels.
Our results also appear to be counter to findings showing elevated cortisol in non-pregnant subjects with panic disorder, OCD, and GAD (Abelson and Curtis 1996; Goldstein et al. 1987; Roy-Byrne et al. 1986; Kluge et al. 2007; Catapano et al. 1992; Monteleone et al. 1994, 1997, 1998; Gehris et al. 1990; Tafet et al. 2001). Our report is the first to assess cortisol in pregnant women with these disorders. Among the 34 subjects in the anxiety group, only 3 subjects met criteria for panic disorder (1 with agoraphobia), 1 subject had clinically significant obsessions, 16 had GAD, 15 had a specific phobia, 8 had a social phobia, and 3 had agoraphobia without panic disorder. We cannot say with certainty that pregnant women with particular anxiety disorders did not have elevated cortisol levels; rather it does appear that subjects with anxiety disorders as a general group did not. Further research into the associations of specific anxiety disorders with antenatal cortisol levels is needed.
The findings here are consistent with others (Hartikainen-Sorri et al. 1991; Kammerer et al. 2002; Saisto et al. 2004) showing blunted cortisol response to stressors during the third trimester as there were no significant increases to either of the laboratory challenges. Moreover, despite significant individual variation in reactivity in past studies, cortisol response to these laboratory stressors did not differ by psychiatric status. Our findings add to the growing list of studies showing buffered stress reactivity in pregnant women (Hartikainen-Sorri et al. 1991; Matthews and Rodin 1992; Glynn et al. 2001; Kammerer et al. 2002; Saisto et al. 2004; Glynn et al. 2004). During pregnancy, experiences of significant life stressors, such as earthquakes, are associated with earlier births (Glynn et al. 2001), which is hypothesized to be mediated by HPA-axis and inflammatory reactivity. However, it may be that there is an evolutionary advantage to perinatal outcome of suppressed HPA–axis reactivity during pregnancy so that minimal stressors such as tasks in a laboratory fail to elicit responses. Interestingly, in a recent study of the effects of women’s depression and anxiety on the cortisol awakening response, there was no difference between women with and without depression although here too comorbidity was not evaluated (Shea et al. 2007).
The results regarding self-report measures of pregnancy-specific experiences from the PES were consistent with the finding that elevated cortisol during late pregnancy was found only in women comorbid for depression and anxiety. Comorbid women had significantly lower uplift frequency scores and significantly higher hassle intensity scores and composite scores (ratio of hassle intensity to uplift intensity) than controls, while all other group comparisons to controls were non-significant. This closely mirrors the cortisol results where comorbid subjects had higher overall cortisol levels than controls but other diagnostic groups did not. It seems that comorbid women experience pregnancy as having more hassles and fewer uplifts than women with only depression or anxiety. Whether physiological differences in comorbid women such as cortisol levels precipitate this difference in perception (or the converse) should be further explored.
There are several limitations to the study. As described in the methods section, 49 women did not provide adequate saliva samples at one or more of the time points for the cortisol assay and were not used in the analyses. The distribution among these excluded subjects is fairly different from that seen in the 180 subjects used in our analyses. This may indicate a selection bias since almost half of those excluded from our analyses because of inadequate saliva samples had a psychiatric diagnosis and their cortisol levels could have been different from those able to give adequate samples. This also may indicate a psychopathology-related physiological difference. Perhaps pregnant women with certain psychiatric disorders produce lower levels of saliva than women without such disorders. There is also the possibility that women with a psychiatric disorder are less motivated to submit adequate saliva samples. Another weakness in the study is that subjects experienced slightly different protocols; however, we found no difference in laboratory task assignment by diagnosis group and thus interpreted the difference in task as not accounting for diagnosis group differences in cortisol reactivity. Also, psychiatric diagnoses and cortisol levels were not assessed contemporaneously. It is possible that by the time of the third trimester laboratory assessment women’s psychiatric status, assessed in the second trimester, had changed; although the results of the self-report symptoms, taken during the third trimester, counter this concern.
Conclusions
In our sample of pregnant women, comorbid anxiety and depression — but not depression or anxiety alone — is associated with elevated cortisol levels. Moreover, comorbidity is associated with more negative pregnancy-specific experiences. These data suggest that during pregnancy, the HPA axis is altered in comorbidity, and therefore comorbidity may be a risk factor to the fetus with the potential to influence development. On the other hand, our results also suggest that the mechanisms by which antenatal depression or anxiety influence fetal development may not involve differential cortisol reactivity to stress, at least with regard to reactivity patterns that were be assessed in our laboratory paradigm. Other alterations in women’s HPA axis, such as that associated with social or family stressors remains to be investigated. These findings highlight the need to characterize the unique psychophysiological profiles associated with different psychiatric disorders during pregnancy to better determine how women’s experiences influence fetal development.
References
Abelson JL, Curtis GC (1996) Hypothalamic–pituitary–adrenal axis activity in panic disorder. 24-hour secretion of corticotropin and cortisol. Arch Gen Psychiatry 53:323–331
Benediktsson R, Lindsay RS, Noble J, Seckl JR, Edwards CR (1993) Glucocorticoid exposure in utero: new model for adult hypertension. Lancet 341:339–341
Brand SR, Engel SM, Canfield RL, Yehuda R (2006) The effect of maternal PTSD following in utero trauma exposure on behavior and temperament in the 9-month-old infant. Ann NY Acad Sci 1071:454–458
Carroll BJ (1976) Limbic system-adrenal cortex regulation in depression and schizophrenia. Psychosom Med 38:106–121
Carroll BJ, Curtis GC, Mendels J (1976) Cerebrospinal fluid and plasma free cortisol concentrations in depression. Psychol Med 6:235–244
Catapano F, Monteleone P, Fuschino A, Maj M, Kemali D (1992) Melatonin and cortisol secretion in patients with primary obsessive-compulsive disorder. Psychiatry Res 44:217–225
Clark PM (1998) Programming of the hypothalamo–pituitary–adrenal axis and the fetal origins of adult disease hypothesis. Eur J Pediatr 157:S7–S10
Cohen S, Kamarck T, Mermelstein R (1983) A global measure of perceived stress. J Health Soc Behav 24:385–396
de Weerth C, Buitelaar JK (2005) Physiological stress reactivity in human pregnancy—a review. Neurosci Biobehav Rev 29:295–312
Diego MA, Field T, Hernandez-Reif M, Cullen C, Schanberg S, Kuhn C (2004) Prepartum, postpartum, and chronic depression effects on newborns. Psychiatry 67:63–80
Diego MA, Jones NA, Field T, Hernandez-Reif M, Schanberg S, Kuhn C, Gonzalez-Garcia A (2006) Maternal psychological distress, prenatal cortisol, and fetal weight. Psychosom Med 68:747–753
Dinan TG (1994) Glucocorticoids and the genesis of depressive illness. A psychobiological model. Br J Psychiatry 164:365–371
DiPietro JA, Hilton SC, Hawkins M, Costigan KA, Pressman EK (2002) Maternal stress and affect influence fetal neurobehavioral development. Dev Psychol 38:659–668
DiPietro JA, Ghera MM, Costigan K, Hawkins M (2004) Measuring the ups and downs of pregnancy stress. J Psychosom Obstet Gynaecol 25:189–201
Field T, Diego M, Hernandez-Reif M, Vera Y, Gil K, Schanberg S, Kuhn C, Gonzalez-Garcia A (2004) Prenatal maternal biochemistry predicts neonatal biochemistry. Int J Neurosci 114:933–945
Field T, Hernandez-Reif M, Diego M, Figueiredo B, Schanberg S, Kuhn C (2006) Prenatal cortisol, prematurity and low birthweight. Infant Behav Dev 29:268–275
Field T, Diego M, Hernandez-Reif M, Figueiredo B, Schanberg S, Kuhn (2007) Sleep disturbances in depressed pregnant women and their newborns. Infant Behav Dev 30:127–133
First M, Spitzer R, Gibbon M, Williams J (1997) Structured clinical interview diagnostic (SCID) for DSM-IV axis I disorders 3/4 clinical version (SCID-CV). American Psychiatric Press, Washington
Gehris TL, Kathol RG, Black DW, Noyes R Jr (1990) Urinary free cortisol levels in obsessive-compulsive disorder. Psychiatry Res 32:151–158
Glynn LM, Wadhwa PD, Dunkel-Schetter C, Chicz-Demet A, Sandman CA (2001) When stress happens matters: effects of earthquake timing on stress responsivity in pregnancy. Am J Obstet Gynecol 184:637–642
Glynn LM, Schetter CD, Wadhwa PD, Sandman CA (2004) Pregnancy affects appraisal of negative life events. J Psychosom Res 56:47–52
Goldstein S, Halbreich U, Asnis G, Endicott J, Alvir J (1987) The hypothalamic–pituitary–adrenal system in panic disorder. Am J Psychiatry 144:1320–1323
Halbreich U, Asnis GM, Shindledecker R, Zumoff B, Nathan RS (1985) Cortisol secretion in endogenous depression. I. Basal plasma levels. Arch Gen Psychiatry 42:904–908
Hartikainen-Sorri AL, Kirkinen P, Sorri M, Anttonen H, Tuimala R (1991) No effect of experimental noise exposure on human pregnancy. Obstet Gynecol 77:611–615
Hoehn-Saric R, McLeod DR, Lee YB, Zimmerli WD (1991) Cortisol levels in generalized anxiety disorder. Psychiatry Res 38:313–315
Holsboer F, von Bardeleben U, Buller R, Heuser I, Steiger A (1987) Stimulation response to corticotropin-releasing hormone (CRH) in patients with depression, alcoholism and panic disorder. Horm Metab Res Suppl 16:80–88
Kammerer M, Adams D, von Castelberg B, Glover V (2002) Pregnant women become insensitive to cold stress. BMC Pregnancy Childbirth 2:8
Kathol RG, Noyes R Jr, Lopez AL, Reich JH (1988) Relationship of urinary free cortisol levels in patients with panic disorder to symptoms of depression and agoraphobia. Psychiatry Res 24:211–221
Kluge M, Schussler P, Kunzel HE, Dresler M, Yassouridis A, Steiger A (2007) Increased nocturnal secretion of ACTH and cortisol in obsessive compulsive disorder. J Psychiatr Res 41:928–933
Lundy BL, Jones NA, Field T, Nearing G, Davalos M, Pietro PA, Schanberg S, Kuhn C (1999) Prenatal depression effects on neonates. Infant Behav Dev 22:119–129
Maes M, Meltzer HY, Bosmans E (1994) Psychoimmune investigation in obsessive–compulsive disorder: assays of plasma transferrin, IL-2 and IL-6 receptor, and IL-1 beta and IL-6 concentrations. Neuropsychobiology 30:57–60
Matthews KA, Rodin J (1992) Pregnancy alters blood pressure responses to psychological and physical challenge. Psychophysiology 29:232–240
Millet B, Touitou Y, Poirier MF, Bourdel MC, Hantouche E, Bogdan A, Olie JP (1998) Plasma melatonin and cortisol in patients with obsessive–compulsive disorder: relationship with axillary temperature, physical activity, and clinical symptoms. Biol Psychiatry 44:874–881
Monk C, Fifer WP, Sloan RP, Myers MM, Bagiella E, Ellman L, Hurtado A (2001) Physiologic responses to cognitive challenge during pregnancy: effects of task and repeat testing. Int J Psychophysiol 40:149–159
Monteleone P, Catapano F, Del Buono G, Maj M (1994) Circadian rhythms of melatonin, cortisol and prolactin in patients with obsessive-compulsive disorder. Acta Psychiatr Scand 89:411–415
Monteleone P, Catapano F, Tortorella A, Maj M (1997) Cortisol response to d-fenfluramine in patients with obsessive–compulsive disorder and in healthy subjects: evidence for a gender-related effect. Neuropsychobiology 36:8–12
Monteleone P, Catapano F, Fabrazzo M, Tortorella A, Maj M (1998) Decreased blood levels of tumor necrosis factor-alpha in patients with obsessive–compulsive disorder. Neuropsychobiology 37:182–185
Radloff LS (1977) The CES-D scale: a self-report depression scale for research in the general population. J Appli Psychol Meas 1:385–401
Roy-Byrne PP, Uhde TW, Post RM, Gallucci W, Chrousos GP, Gold PW (1986) The corticotropin-releasing hormone stimulation test in patients with panic disorder. Am J Psychiatry 143:896–899
Saisto T, Kaaja R, Helske S, Ylikorkala O, Halmesmaki E (2004) Norepinephrine, adrenocorticotropin, cortisol and beta-endorphin in women suffering from fear of labor: responses to the cold pressor test during and after pregnancy. Acta Obstet Gynecol Scand 83:19–26
Sandman CA, Glynn L, Schetter CD, Wadhwa P, Garite T, Chicz-DeMet A, Hobel C (2006) Elevated maternal cortisol early in pregnancy predicts third trimester levels of placental corticotropin releasing hormone (CRH): priming the placental clock. Peptides 27:1457–1463
Seckl JR (2001) Glucocorticoid programming of the fetus; adult phenotypes and molecular mechanisms. Mol Cell Endocrinol 185:61–71
Seckl JR, Meaney MJ (2004) Glucocorticoid programming. Ann NY Acad Sci 1032:63–84
Seng JS, Low LK, Ben-Ami D, Liberzon I (2005) Cortisol level and perinatal outcome in pregnant women with posttraumatic stress disorder: a pilot study. J Midwifery Womens Health 50:392–398
Shea AK, Streiner DL, Fleming A, Kamath MV, Broad K, Steiner M (2007) The effect of depression, anxiety and early life trauma on the cortisol awakening response during pregnancy: preliminary results. Psychoneuroendocrinology 32:1013–1020
Siever LJ, Uhde TW, Jimerson DC, Post RM, Lake CR, Murphy DL (1984) Plasma cortisol responses to clonidine in depressed patients and controls. Evidence for a possible alteration in noradrenergic-neuroendocrine relationships. Arch Gen Psychiatry 41:63–68
Spielberger CD (1983) Manual for the State-Trait Anxiety Inventory (STAI). Consulting Psychologists Press, Palo Alto, CA
Tafet GE, Idoyaga-Vargas VP, Abulafia DP, Calandria JM, Roffman SS, Chiovetta A, Shinitzky M (2001) Correlation between cortisol level and serotonin uptake in patients with chronic stress and depression. Cogn Affect Behav Neurosci 1:388–393
Uhde TW, Joffe RT, Jimerson DC, Post RM (1988) Normal urinary free cortisol and plasma MHPG in panic disorder: clinical and theoretical implications. Biol Psychiatry 23:575–585
Yehuda R, Southwick SM, Nussbaum G, Wahby V, Giller EL Jr, Mason JW (1990) Low urinary cortisol excretion in patients with posttraumatic stress disorder. J Nerv Ment Dis 178:366–369
Yehuda R, Kahana B, Binder-Brynes K, Southwick SM, Mason JW, Giller EL (1995) Low urinary cortisol excretion in Holocaust survivors with posttraumatic stress disorder. Am J Psychiatry 152:982–986
Yehuda R, Teicher MH, Trestman RL, Levengood RA, Siever LJ (1996) Cortisol regulation in posttraumatic stress disorder and major depression: a chronobiological analysis. Biol Psychiatry 40:79–88
Acknowledgements
This research was supported by the March of Dimes, the National Alliance for Research on Schizophrenia and Depression, the Sackler Institute, a Career Development Award (MH01928) to Catherine Monk, and an NIMH postdoctoral training grant (T32 MH018264). We would like to thank the many women and children who participated in this research, as well as Felice Tager, Lauren Ellman, Elizabeth Werner and Sylvia Cabral for their contributions in the collection of these data.
Financial Disclosures
Drs. Evans, Myers, and Monks reported no biomedical financial interests or potential conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Evans, L.M., Myers, M.M. & Monk, C. Pregnant women’s cortisol is elevated with anxiety and depression — but only when comorbid. Arch Womens Ment Health 11, 239–248 (2008). https://doi.org/10.1007/s00737-008-0019-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00737-008-0019-4