
Abstract
The aim of this analysis was to determine the relationship between monosodium glutamate (MSG) intake and change in hemoglobin (Hb) levels and the risk of anemia over 5 years in 1197 Chinese men and women who participated in the Jiangsu Nutrition Study (JIN). MSG intake and Hb were quantitatively assessed in 2002 and followed up in 2007. Diet and lifestyle factors were assessed at both time points. There was a positive association between MSG intake and increase in Hb among men but not women. In the multivariate model adjusting for demographic and lifestyle factors as well as baseline dietary pattern, the beta values and 95% confidence interval for Hb changes across quartiles of MSG intake were 0, 0.67(0.04–1.29), 0.99(0.38–1.60), 0.73(0.13–1.34) among men (p for trend 0.091); 0, −0.01(−0.45–0.43), 0.23(−0.25–0.71), and −0.45(−0.96–0.05) among women (p for trend 0.087). Among anemic participants at baseline, there was a significant inverse association between MSG intake and the risk of anemia at follow-up. Comparing extreme quartiles of MSG intake among those anemic at baseline, the relative risk for persistent anemia at follow-up was 0.49 (95% CI: 0.28–0.86, p < 0.01). The association was independent of dietary patterns and lifestyle factors. A dose–response relationship between MSG intake and increase in Hb levels among anemic participants was seen. MSG intake may have independent Hb-increasing effects, especially among men and those anemic at baseline.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Three decades ago more than half of the population of China was anemic (Chang et al. 1998). With economic development and improvements in nutrition the prevalence of anemia has decreased dramatically (Li et al. 2005). Nevertheless, data from the 2002 Chinese National Nutrition Survey showed that more than 15% of the population remained anemic (Li et al. 2005) despite the average intake of iron of about 23 mg/d (Zhai et al. 2007). Dietary patterns (Shi et al. 2006a), tofu intake (Shi et al. 2008d), and magnesium intake (Shi et al. 2008a) have been shown to be associated with anemia in Chinese population. Previously we have shown that anemia coexists with components of metabolic syndrome; isolated anemia is uncommon (Shi et al. 2008c).
Monosodium glutamate (MSG) is a widely used food taste enhancer, especially in Asia. Over the past three decades extensive studies have been undertaken to determine potential health effects of MSG, both adverse and beneficial (Kwok 1968; Jinap and Hajeb 2010; He et al. 2008; Baad-Hansen et al. 2010; Stamler et al. 2009).
A significant increase in hemoglobin levels was found among children using vitamin A fortified MSG in a population trial (Muhilal et al. 1988). MSG intake stimulates gastric acid secretion (Uneyama et al. 2008), which is important for non-heme iron absorption (Lynch 1997). Although amino acids have been shown to enhance the absorption of iron (Martinez-Torres and Layrisse 1970; Forth and Rummel 1973), to our knowledge no study has ever assessed the association between MSG intake and hemoglobin levels or the risk of anemia. The objective of the study was to assess these associations over 5 years among Chinese adults using data from the Jiangsu Nutrition Study.
Subjects and methods
Sample
The methodologies of the Jiangsu Nutrition (JIN) Cohort Study have been described previously (Shi et al. 2009b, 2010a, b). The sample was based on a subsample of the Chinese national nutrition and health survey representing Jiangsu province and the year 2002 was used as a base line. The rural sample was selected from six counties (Jiangyin, Taichang, Shuining, Jurong, Sihong, and Haimen). From each of the six counties, three smaller towns were randomly selected. The urban sample was selected from the capital cities of the two prefectures, Nanjing and Xuzhou, and from each capital city three streets were randomly selected. The six counties and the two prefectures represented a geographically and economically diverse population. In each town/street, two villages/neighborhoods were randomly selected, and 90 households were further selected randomly from each village/neighborhood. All the members in the households were invited to take part in the study. In addition, one-third of the households were interviewed on dietary intake.
In 2002, detailed questionnaire-based and observational dietary information was obtained from 2,849 adults aged 20 and above living in two cities and six rural areas. In 2007, all the baseline participants were contacted and 1,682 participants were identified through household visits, and 1,492 of them participated in the follow-up interview. Of these 1,282 (76.2%) attended clinic visits where anthropometric and other measurements were obtained, and 210 participants completed the interview at home but missed the measurement in the clinic. For the current analyses, we excluded those participants who had extreme values of weight change (i.e. >20 kg, n = 11), and those who had known diabetes, stroke, or cancer at baseline (n = 40). Four participants had missing values for MSG intake at baseline. Thirty participants did not have hemoglobin (Hb) data at baseline or follow-up. The final sample size examined for Hb change consisted of 494 men and 703 women (total n = 1197). Compared with the retained participants, those lost to follow-up were generally younger (45.5 vs. 49.3 years), but there were no differences in mean BMI, or energy intake. The study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving human subjects/patients were approved by Jiangsu Provincial Centre for Disease Control and Prevention. Written consent to participate was obtained from all the participants.
Data collection and measurements
Participants were interviewed at their homes by health workers using a standard questionnaire (Shi et al. 2010a). The health workers were intensively trained in all aspects of data collection.
Outcome variables
An overnight fasting blood sample was collected at baseline and follow-up. The blood samples were analyzed for hemoglobin (Hb) using the cyanmethemoglobin method (Dallman 1984) in the local Centers for Disease Control and Prevention. Anemia was defined as a Hb level below 13 g/dl for men and 12 g/dl for women (WHO 1968).
Dietary intake
In 2002 and 2007, dietary intake patterns during the previous year were investigated by a series of detailed questions about the usual frequency and quantity of intake of 33 food groups and beverages using a food frequency questionnaire (FFQ) administered by a trained health care worker. The FFQ administered in this manner has been validated with weighted food records (Li et al. 2006; Zhao et al. 2002; He et al. 2009). To determine the amount of MSG and other seasonings consumed by individuals, each household was specifically asked about their usual monthly consumption of these items. Average total glutamate intake was also calculated by adding the glutamate concentrations of all foods/seasonings consumed by an individual per day. Baseline nutrient (e.g. sodium, potassium, fiber), alcohol, and vegetable oil intakes were assessed using a 3-day weighed food diary which recorded all foods consumed by each individual, on three consecutive days; this was done to confirm the intakes reported from the FFQ data and was not undertaken at follow-up. We did not consider under- and over-reporting of energy intake to be an issue, because upon reviewing the food diaries with the subjects, the health workers would clarify any intake value for a particular food that fell below or above the usual value reportedly consumed by the population within the region. Not everyone in the household was asked for dietary information at follow-up (FFQ was only used among those 15 years and above); however, the household MSG intake was determined, and thus the mean household MSG intake was calculated. Food consumption data were analyzed using the Chinese Food Composition Table (Yang 2005).
Exposure variable: MSG intake at baseline
Individual consumption of MSG was calculated according to the total amount of MSG consumed in the household (assessed by the FFQ) divided by the number of individuals per household and then adjusted for the proportion of the household energy intake energy consumed by each individual (assessed by the 3-day weighted food diary).
Dietary patterns
Baseline dietary patterns were identified by factor analysis based on food intake measured by the FFQ, using standard principal component analysis as described elsewhere (Shi et al. 2008a, b, c, d). In short, four food patterns were obtained: Factor 1 (‘macho’) was characterized by various kinds of animal foods and alcohol; Factor 2 (the ‘traditional’ pattern) loaded heavily on rice, fresh vegetables, and inversely on wheat flour; Factor 3 (‘sweet tooth’) contained cake, milk, yoghurt, and drinks; and Factor 4 (‘vegetable rich’ pattern) included whole grains, fruits, root vegetables, fresh and pickled vegetables, milk, eggs, and fish. The four factors explained 28.5% of the variance in intake. Similarly, four dietary patterns were identified at follow-up. The correlation coefficient for corresponding dietary patterns between baseline and follow-up ranged from 0.139 (‘vegetable rich’ pattern) to 0.593 (‘traditional’ pattern).
Other lifestyle factors
Cigarette smoking was assessed by asking the frequency of daily cigarette smoking in the past 30 days. Passive smoking was defined as exposure to another person’s tobacco smoke at home or in the workplace for at least 15 min daily for >1 day every week. Information on passive smoking was obtained among non-smokers. Eating out was assessed by asking whether individuals ate out on a frequent basis and was coded as yes or no. If a person reported his/her usual eating place for breakfast, lunch or dinner was away from home, the value for eating out was yes. Education was recoded into either ‘Low’ (illiteracy, primary school); ‘Medium’ (junior middle school); or, ‘High’ (high middle school or higher), based on six categories of education levels in the questionnaire. Occupation was recoded into ‘Manual’ or ‘Non-manual’ based on a question with 12 occupational categories. Hypertension medication use (yes/no) was asked at baseline and follow-up.
Anthropometric and other measurements
In both 2002 and 2007, anthropometric measurements were obtained using standard protocols and techniques (Wu et al. 2008; He et al. 2009). Body weight was measured unshod, in light indoor clothing to the nearest 100 g with a balance-beam scale, and height to the nearest mm using a stadiometer. Waist circumference was measured to the nearest mm midway between the inferior margin of the last rib and the crest of the ilium, in the mid-axillary line in a horizontal plane. Family history of hypertension was defined as the presence of known family members with hypertension in any of three generations (siblings, parents, or grandparents). Blood pressure was measured twice by mercury sphygmomanometer on the right upper arm of the subject, who was seated for 5 min before the measurement. The mean of these two measurements was used in the analyses. The cuff size was selected on the basis of the upper arm circumference to ensure that the cuff did not overlap (Wu et al. 2008). Hypertension was defined as systolic blood pressure above 140 mmHg and/or diastolic blood pressure above 90 mmHg, or use of antihypertensive medications.
Statistics
MSG intake was coded into quartiles. Chi square test was used to compare differences between categorical variables, and ANOVA was used to compare differences in continuous variables between groups. A Kernel density plot was used to visually examine the relationship between MSG intake quartiles and Hb change by anemia status at baseline. Mixed-effects linear regression was used to determine the association between MSG intake (quartiles) and Hb change adjusted for age (model 1) and further adjustment for education, occupation, smoking, alcohol drinking, hypertension, overweight (yes/no) at baseline, eating out, energy, iron and vitamin C intake (as continuous variables) (model 2), baseline dietary patterns (model 3), and follow-up dietary patterns (model 4). We tested for linear trend across categories of MSG intake by assigning each participant the median value for the category and modeling this value as a continuous variable. These multivariate models were adjusted for household cluster using the xtmixed command. Poisson regression with robust variance models were also used to assess the association between MSG intake quartiles and anemia at follow-up (Barros and Hirakata 2003). Food patterns were also put into the multivariate models to control for residual confounding, as suggested by Imamura et al. (Imamura et al. 2009). In the provinces, a distinct definition of urban/rural dwelling is difficult due to ongoing economic development. Since we have adjusted for education and job status as well as dietary patterns, the decision was made not to adjust for urban/rural. All the analyses were performed using STATA 11 (Stata Corporation, College Station). Statistical significance was considered to be when p < 0.05 (two sided).
Results
At baseline 23.9% of men and 35.6% of women were anemic (Table 1). Smoking and alcohol consumption were common among men but rare among women. At follow-up, the prevalence of anemia was 17.0% in men and 25.3% in women. In total, 12.8% developed anemia, while anemia resolved in 21.6%. Only 9.1% of the participants had persistent anemia after the 5-year follow-up.
The mean intake of MSG for the entire sample was 3.8 g/day (SD 4.2). Of the 1197 participants, 70 participants reported no use of MSG and median intakes across the quartiles were 0.8, 2.0, 3.7, and 7.0 g/day, respectively. Some of the food and nutrient intakes, including those of MSG, alcohol, and heme iron were characterized by very large variances with the SD larger than the mean.
MSG intake was inversely associated with non-heme iron intake but positively associated with heme iron intake (Table 2). At baseline the prevalence of anemia was 24.0, 32.4, 41.5, and 25.1%, across the MSG intake quartiles, respectively (p < 0.01). Quartiles 2 and 3 of MSG intake had a higher prevalence of anemia than the other two quartiles. However, an inverse association between MSG intake and prevalence of anemia was found at follow-up; the prevalence of anemia at follow-up across quartiles of MSG intake was 25.3, 24.8, 21.1, and 16.4% (p value 0.030).
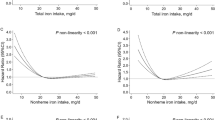
Figure 1 shows the distribution of change in Hb levels according to MSG intake quartiles by anemia status at baseline. A clear dose–response shift of the distribution towards the right according to MSG quartiles was found among the anemic participants. In the linear regression, MSG intake (continuous) was significantly positively associated with Hb increase among anemic participants (p < 0.001) (data not shown).

Kernel density estimation of 5-year change in Hb levels according to MSG intake quartiles by anemic status at baseline among Chinese adults. Q1 represents the lowest quartile of MSG intake
Table 3 shows the associations between MSG intake and Hb changes using regression analyses. There was a positive association between MSG intake and changes in Hb levels in men but not women. In the model including baseline dietary pattern adjustment (model 3), the beta values and 95% CI for Hb changes across quartiles of MSG intake were 0, 0.67(0.04–1.29), 0.99(0.38–1.60), 0.73(0.13–1.34) among men (p for trend 0.091); and 0, −0.01(−0.45–0.43), 0.23(−0.25–0.71), and −0.45(−0.96–0.05) among women (p for trend 0.087). Additional adjustment for dietary patterns at follow-up did not change the association. When we limited the analysis to women with age >45 years, the beta values for Hb change across quartiles of MSG intake were 0, 0.50(−0.07–1.08), 0.63(0.02–1.23), and −0.33(−0.98–0.32) (p for trend 0.183).
At baseline 45 participants reported that they had changed their diet to control chronic disease. During follow-up, 21 participants reported using medication to control anemia and eight participants used iron-fortified soy sauce. After excluding these participants (in total 72), the above associations between MSG intake and Hb change did not change (data not shown). Adjusting for the change in blood pressure did not change the association.
Table 4 shows the inverse association between MSG intake and risk of anemia, especially among those anemic at baseline using Poisson regression. Comparing extreme quartiles of MSG intake among those anemic at baseline, the relative risk (RR) for anemia at follow-up was 0.49(0.28–0.86, p < 0.01) in the quartile with the highest MSG intake. Additional adjustment of heme iron or red meat consumption did not change the association. Further adjusting for dietary patterns at follow-up did not change the association. Among those non-anemic at baseline, there was a positive association between follow-up ‘macho’ food pattern and incident anemia (data not shown).
When we used the mean household MSG intake at follow-up as the exposure variable, the associations between MSG intake and Hb change were consistent with those of baseline MSG intake. After adjusting for the covariates in Model 3 of Table 3, the beta (95% CI) for Hb changes across quartiles of mean household MSG intake was 0, 0.12(−0.43–0.66), 0.55(−0.04–1.14) and 0.70(0.14–1.25) (p for trend 0.006) for men; 0, 0.71(0.26–1.17), 0.27(−0.22–0.77) and 0.14(−0.33–0.61) (p for trend 0.777) for women; and 0, 0.51(0.14–0.89), 0.47(0.06–0.88) and 0.47(0.07–0.86) (p for trend 0.020) for gender combined (data not shown).
Discussion
To our knowledge, this is the first population cohort study showing a positive association between MSG intake and Hb change; an association observed in men but not in women. Among participants who were anemic at baseline, there was a significant inverse relationship between MSG intake and the risk of anemia at follow-up, independent of dietary patterns and lifestyle factors. A significant dose–response relationship between MSG intake and increase in Hb levels among anemic participants was observed.
The gender-specific effect of MSG on Hb might be because of an inability to adjust for blood loss from menstruation. When we limit our analysis to women aged above 45, there was a significant difference in Hb change between first and third quartiles of MSG intake.
The study was undertaken in a generally affluent area and the mean iron intake (mainly non-heme iron) in the sample was much higher than the average for Western populations. The mean iron intake among women, for example, of 23.4 mg/d (Shi et al. 2006b) was almost double the amount observed among participants in The Women’s Health Initiative study (Thomson et al. 2011). After the baseline survey, an anemia intervention program, using iron-fortified soy sauce, was launched. The number of participants reporting use of this iron-fortified soy sauce was very small, and very few people reported taking medication of any sort to control anemia. Nevertheless, over the 5 years of the study, the increase in Hb was generally only seen in those who were anemic at baseline, suggesting that anemic participants either improved overall nutrition or took other measures to control anemia. Even when we excluded those reporting using iron-fortified soy sauce, taking medication and accounted for dietary pattern at both baseline and follow-up, the link between MSG and Hb change remains the same. Figure 1 shows a clear dose–response shift in the distribution of Hb change by levels of MSG intake among baseline anemic participants. In the multivariate models, after adjusting for potential confounders including sociodemographic factors, the association between MSG intake and Hb change remained significant. The discrepancy between the positive association between MSG intake and anemia at baseline and the opposite effect at follow-up might be the result of reverse causation at baseline in that anemic participants may have already changed their diet at baseline. We previously found anemic participants ate more meat but less Tofu (which is cheap) than non-anemic participants at baseline (Shi et al. 2008d, 2009a). A positive association between follow-up ‘macho’ pattern and incident anemia may suggest such reverse causation.
Several mechanisms may explain the relationship between MSG intake and Hb levels. First, MSG intake has been demonstrated to increase the secretion of gastric acid in dogs (Zolotarev et al. 2009). In humans, as in animals, MSG has significant effects on gastric secreto-motor activity (Uneyama et al. 2008), and it has recently been shown that after a standard meal, MSG raises antral distension in humans, and it is therefore likely that MSG also increases gastric acid secretion (Boutry et al. 2011). Gastric acid is necessary for optimal non-heme iron absorption (Lynch 1997). MSG intake increases the level of plasma amino acids in human (Boutry et al. 2011). It has been known for more than 40 years that amino acids increase iron intestinal absorption (Martinez-Torres and Layrisse 1970; Forth and Rummel 1973). Second, MSG may mediate an effect on Hb via leptin. MSG intake was positively related to levels of leptin in animal studies (Diniz et al. 2005); leptin and its receptors play an important role in hematopoiesis (Bennett et al. 1996). Leptin upregulates hepatic hepcidin expression suggesting an effect on iron absorption (Chung et al. 2007), and leptin may act synergistically with erythropoietin (EPO) in the regulation of erythropoiesis. The potential role of leptin in hematopoiesis has recently been the subject of a review (Fantuzzi and Faggioni 2000). Leptin levels have been shown to be a predictor of erythropoietin sensitivity in end-stage renal disease (Axelsson et al. 2005). Using data from China Nutrition and Health Study, we found a positive link between leptin levels and hemogoblin levels among adults in Jiangsu China (unpublished data). Our previous studies suggest infection or inflammation may have an important role in the etiology of anemia in the region (Shi et al. 2006a, 2008a, d). Further research is needed to assess whether MSG intake has a direct effect on hepcidin, the main iron regulator under the condition of infection/inflammation. Finally, MSG stimulates L-type Ca2 + channels (LVDCC). LVDCC is found to provide a pathway for iron entry into cardimyocytes (Oudit et al. 2003). Overactivation of N-methyl-d-asparate receptor (NMDA glutamate receptor) increases the uptake of iron in neuronal cells (Cheah et al. 2006).
The situation in China (as also true from other Asian countries) is characterized by a high level of MSG uptake and a relatively high prevalence of anemia. This suggests that the amount of glutamate in the diet would not represent a limiting factor for iron intestinal absorption. How can we explain that there is a dose relationship between MSG intake and increase of Hb levels among anemic patients? The high intake of MSG in China did not start until 1980s. In 1970s MSG use was not prevalent in the rural areas, where farmers used eggs in exchange for soysauce and MSG. With the process of nutrition transition (also the increase of MSG intake), the prevalence of anemia decreased.
The main limitation of this study is the measurement of MSG consumption was determined by the total amount of MSG consumed in the household divided by the number of individuals per household and then adjusted for the proportion of the household energy intake energy. This method may under or overestimate MSG intake, although in a large epidemiological study, this would be the most practical way of measuring MSG consumption. This over or under estimation could happen to both anemic and non-anemic participants. We would expect the bias to be non-differential with regard to the impact on the analysis and interpretation of the results. Other limitations include the inability to account for a change in MSG consumption during the 5-year follow-up period. The high rate of attrition limits the ability to generalize the findings in the population. The strength of the study is the relatively large sample size and the prospective study design. Furthermore, we are able to adjust for a range of covariates including overall dietary patterns at both baseline and follow-up. The large variation of MSG intake as well as the high prevalence of anemia adds to the power of the study.
In conclusion, MSG intake was positively associated with Hb change over 5 years and may reduce the risk of anemia among Chinese adults.
References
Axelsson J, Qureshi AR, Heimburger O, Lindholm B, Stenvinkel P, Barany P (2005) Body fat mass and serum leptin levels influence epoetin sensitivity in patients with ESRD. Am J Kidney Dis 46:628–634
Baad-Hansen L, Cairns BE, Ernberg M, Svensson P (2010) Effect of systemic monosodium glutamate (MSG) on headache and pericranial muscle sensitivity. Cephalalgia 30:68–76
Barros A, Hirakata V (2003) Alternatives for logistic regression in cross-sectional studies: an empirical comparison of models that directly estimate the prevalence ratio. BMC Med Res Methodol 3:21
Bennett BD, Solar GP, Yuan JQ, Mathias J, Thomas GR, Matthews W (1996) A role for leptin and its cognate receptor in hematopoiesis. Curr Biol 6:1170–1180
Boutry C, Matsumoto H, Airinei G, Benamouzig R, Tome D, Blachier F, Bos C (2011) Monosodium glutamate raises antral distension and plasma amino acid after a standard meal in humans. Am J Physiol Gastrointest Liver Physiol 300:G137–G145
Chang S, Ge K, Zhai F, Jia F, Xu X (1998) The analysis of nutritional factors on anemia in Chinese adults. Acta Nutrimenta Sinica 20:132–137
Cheah JH, Kim SF, Hester LD, Clancy KW, Patterson SE, Papadopoulos V, Snyder SH (2006) NMDA receptor-nitric oxide transmission mediates neuronal iron homeostasis via the GTPase Dexras1. Neuron 51:431–440
Chung B, Matak P, McKie AT, Sharp P (2007) Leptin increases the expression of the iron regulatory hormone hepcidin in HuH7 human hepatoma cells. J Nutr 137:2366–2370
Dallman PR (1984) Diagnosis of anemia and iron deficiency: analytic and biological variations of laboratory tests. Am J Clin Nutr 39:937–941
Diniz YS, Faine LA, Galhardi CM, Rodrigues HG, Ebaid GX, Burneiko RC, Cicogna AC, Novelli ELB (2005) Monosodium glutamate in standard and high-fiber diets: metabolic syndrome and oxidative stress in rats. Nutrition 21:749–755
Fantuzzi G, Faggioni R (2000) Leptin in the regulation of immunity, inflammation, and hematopoiesis. J Leukoc Biol 68:437–446
Forth W, Rummel W (1973) Iron absorption. Physiol Rev 53:724–792
He K, Zhao L, Daviglus ML, Dyer AR, van Horn L, Garside D, Zhu L, Guo D, Wu Y, Zhou B, Stamler J (2008) Association of monosodium glutamate intake with overweight in Chinese adults: the INTERMAP study. Obesity 16:1875–1880
He Y, Ma G, Zhai F, Li Y, Hu Y, Feskens EJ, Yang X (2009) Dietary patterns and glucose tolerance abnormalities in Chinese adults. Diabetes Care 32:1972–1976
Imamura F, Lichtenstein AH, Dallal GE, Meigs JB, Jacques PF (2009) Confounding by dietary patterns of the inverse association between alcohol consumption and type 2 diabetes risk. Am J Epidemiol 170:37–45
Jinap S, Hajeb P (2010) Glutamate. Its applications in food and contribution to health. Appetite 55:1–10
Kwok RHM (1968) Chinese-restaurant syndrome. N Engl J Med 278:796
Li L, Rao K, Kong L, Yao C, Xiang H, Zhai F, Ma G, Yang X (2005) A description on the Chinese national nutrition and health survey in 2002. Zhonghua liu Xing Bing Xue Za Zhi 26:474–484
Li YP, He YN, Zhai FY, Yang XG, Hu XQ, Zhao WH, Ma GS (2006) Comparison of assessment of food intakes by using 3 dietary survey methods. Zhonghua Yu Fang Yi Xue Za Zhi 40:273–280
Lynch SR (1997) Interaction of iron with other nutrients. Nutr Rev 55:102–110
Martinez-Torres C, Layrisse M (1970) Effect of amino acids on iron absorption from a staple vegetable food. Blood 35:669–682
Muhilal, Permeisih D, Idjradinata YR, Muherdiyantiningsi, Karyadi D (1988) Vitamin A-fortified monosodium glutamate and health, growth, and survival of children: a controlled field trial. Am J Clin Nutr, 48, 1271–1276
Oudit G, Sun H, Trivieri M, Koch S, Dawood F, Ackerley C, Yazdanpanah M, Wilson G, Schwartz A, Liu P, Backx P (2003) L-type Ca2 + channels provide a major pathway for iron entry into cardiomyocytes in iron-overload cardiomyopathy. Nat Med 9:1187–1194
Shi Z, Hu X, Yuan B, Pan X, Dai Y, Holmboe-Ottesen G (2006a) Association between dietary patterns and anaemia in adults from Jiangsu Province in Eastern China. Br J Nutr 96:906–912
Shi Z, Hu X, Yuan B, Pan X, Meyer HE, Holmboe-Ottesen G (2006b) Association between serum ferritin, hemoglobin, iron intake, and diabetes in adults in Jiangsu, China. Diabetes Care 29:1878–1883
Shi Z, Hu X, He K, Yuan B, Garg M (2008a) Joint association of magnesium and iron intake with anemia among Chinese adults. Nutrition 24:977–984
Shi Z, Hu X, Yuan B, Hu G, Pan X, Dai Y, Byles JE, Holmboe-Ottesen G (2008b) Vegetable rich food pattern is related to obesity in China. Int J Obes (Lond) 32:975–984
Shi Z, Hu X, Yuan B, Hu G, Pan X, Holmboe-Ottesen G (2008c) Coexistence of anaemia and the metabolic syndrome in adults in Jiangsu, China. Asia Pac J Clin Nutr 17:505–513
Shi Z, Hu X, Yuan B, Pan X, Dai Y, Holmboe-Ottesen G, Byles JE (2008d) Strong negative association between intake of tofu and anemia among Chinese adults in Jiangsu, China. J Am Diet Assoc 108:1146–1153
Shi Z, Pan X, Holmboe-Ottesen G (2009a) Meat consumption and anemia in Chinese adults in Jiangsu Province. In: Amesel L, Hirsch L (eds.) Food Science and Security. Nova Science Publisher, New York
Shi Z, Zhou M, Yuan B, Qi L, Dai Y, Luo Y, Holmboe-Ottesen G (2009b) Iron intake and body iron stores, anaemia and risk of hyperglycaemia among Chinese adults: the prospective Jiangsu Nutrition Study (JIN). Public Health Nutr 13:1319–1327
Shi Z, Luscombe-Marsh ND, Wittert GA, Yuan B, Dai Y, Pan X, Taylor AW (2010a) Monosodium glutamate is not associated with obesity or a greater prevalence of weight gain over 5 years: findings from the Jiangsu Nutrition Study of Chinese adults. Br J Nutr 104:457–463
Shi Z, Yuan B, Qi L, Dai Y, Zuo H, Zhou M (2010b) Zinc intake and the risk of hyperglycemia among Chinese adults: the prospective Jiangsu Nutrition Study (JIN). J Nutr Health Aging 14:332–335
Stamler J, Brown IJ, Daviglus ML, Chan Q, Kesteloot H, Ueshima H, Zhao LC, Elliott P, INTERMAP Research group (2009) Glutamic Acid, the main dietary amino acid, and blood pressure the INTERMAP Study (International collaborative study of macronutrients, micronutrients and blood pressure). Circulation 120:221–228
Thomson CA, Stanaway JD, Neuhouser ML, Snetselaar LG, Stefanick ML, Arendell L, Chen Z (2011) Nutrient intake and anemia risk in the women’s health initiative observational study. J Am Diet Assoc 111:532–541
Uneyama H, Sangabriel A, Kawai M, Tomoe M, Torii K (2008) Physiological role of dietary free glutamate in the food digestion. Asia Pac J Clin Nutr 17(Suppl 1):372–375
WHO (1968) Nutritional anaemias. Report of a WHO scientific group. World Health Organ Tech Rep Ser 405:5–37
Wu YF, Huxley R, Li LM, Anna V, Xie GQ, Yao CH, Woodward M, Li X, Chalmers J, Gao RL, Kong LZ, Yang XG, China NNHS Steering Comm; China NNHS working (2008) Prevalence, awareness, treatment, and control of hypertension in china: data from the China National Nutrition and Health Survey 2002. Circulation 118:2679–2686
Yang Y (2005) Chinese food composition Table 2004. Peking University Medical Press, Beijing
Zhai F, Wang H, Du S, He Y, Wang Z, Ge K, Popkin BM (2007) Lifespan nutrition and changing socio-economic conditions in China. Asia Pac J Clin Nutr 16(Suppl 1):374–382
Zhao W, Hasegawa K, Chen J (2002) The use of food-frequency questionnaires for various purposes in China. Public Health Nutr 5:829–833
Zolotarev V, Khropycheva R, Uneyama H, Torii K (2009) Effect of free dietary glutamate on gastric secretion in dogs. Ann N Y Acad Sci 1170:87–90
Acknowledgments
Z.S. had full access to all data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Z.S. devised the study concept; Z.S. and B.Y. acquired the data; Z.S. conducted the statistical analysis; Z.S. drafted of the manuscript; B.Y., A.W.T., E.D.G, and G.A.W. critically revised the manuscript for important intellectual content. Z.S. had primary responsibility for final content. The authors thank the participating Regional Centers for Disease Control and Prevention in Jiangsu Province, including the Nanjing, Xuzhou, Jiangyin, Taicang, Suining, Jurong, Sihong and Haimen Centers, for their support in the data collection. The study was financed by Jiangsu Provincial Natural Science Foundation BK2008464 and Jiangsu Provincial Health Bureau. The data analysis was supported a research grant from International Glutamate Technical Committee. The contents of this publication do not necessarily reflect the views of the funding bodies.
Conflict of interest
Shi Z, Yuan B, Wittert G, and Taylor A received a research grant from International Glutamate Technical Committee. Dal Grande E has no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Shi, Z., Yuan, B., Taylor, A.W. et al. Monosodium glutamate intake increases hemoglobin level over 5 years among Chinese adults. Amino Acids 43, 1389–1397 (2012). https://doi.org/10.1007/s00726-011-1213-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00726-011-1213-7