
Abstract
Viral diarrhea is a great threat to children’s health in developing countries. We conducted a prospective surveillance study of acute diarrhea of young children at Tianjin Children’s Hospital from April 2008 to April 2009. Viral infections were detected in 356 of the total 766 collected stool specimens (46.48%). Rotavirus infections were the most common (27.94%; predominant type G1), followed by adenovirus infections (17.62%; predominant type Ad41), norovirus infections (5.87%; predominant type GII-4/2006b), and astrovirus infections (3.15%; only HAstV-1). Children younger than 1 year old were the most susceptible population to viral infections (87.9%). Diarrhea, vomiting, and fever were the most frequent clinical symptoms among the infected patients. The viral infections had no age, sex, or regional differences. Most infection rates were higher in the autumn, winter, and spring. This study supported that the rotavirus vaccine should be included in the Expanded Programme on Immunization in China.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The World Health Organization (WHO) has reported that approximately two million deaths per year occur globally due to diarrheal diseases, mainly among children less than five years of age who live in developing countries (http://www.who.int/vaccineresearch/diseases/diarrhoeal/en/index.html). Viruses are a major cause of diarrheal illnesses. In particular, group A rotaviruses (RV) are the leading cause of severe diarrheal diseases and dehydration, which often lead to the hospitalizations of infants and young children throughout the world. Other viral agents, including enteric adenoviruses (AdV), astroviruses (AstV), and human caliciviruses (HucV) like norovirus (NoV) and sapovirus (SaV), are also believed to be major causes of sporadic cases and outbreaks of childhood diarrhea [1].
China has one-fifth of the world’s population and the second largest birth cohort in the world [2]. Currently, hospitalizations associated with viral diarrhea are common for Chinese children. In 2008, the mortality rate of children under 5 years of age was 18.5% in China and 5.98% in Tianjin City [3]. In 2002, approximately 13,400 children under the age of 5 died from RV in China, and 70% of these deaths occurred in rural areas [2]. Although the molecular epidemiology of single RV, AdV, NoV, and AstV infections has been examined in Chinese children, information on the subject is still limited. In fact, only a few studies have investigated the main enteric viruses (RV, AdV, NoV, and AstV) in hospitalized Chinese children [4–6]. Currently, the related clinical, epidemiological, and meteorological information is lacking. These data would be helpful to explore the causes of the disease and to provide an accurate estimate of disease burden. Additionally, these data would help prevent acute viral diarrheal cases in developing countries.
In this study, we aimed to provide intact etiology and epidemiology data on viral diarrhea in Tianjin so that the Tianjin data can be compared with other studies. We collected 766 stool specimens from April 2008 to April 2009 from patients hospitalized in Tianjin Children’s Hospital. We then investigated the prevalence of major viral etiologic agents and examined their molecular characteristics. Moreover, we described the epidemiological characteristics of the hospitalized children and evaluated the climate information and its relationship to the different viral infections.
Materials and methods
Study population and fecal specimens
The study was based in Tianjin City, an independently administered municipal district in China. Tianjin has a permanent population of 11.97 million, representing approximately 0.89% of the Chinese population [3]. A total of 766 fecal specimens were prospectively collected from hospitalized pediatric patients younger than 5 years old. All of the patients were admitted with acute diarrhea to Tianjin Children’s Hospital between April 2008 and April 2009. The hospitalization criteria in these cases were diarrhea, fever, vomiting, convulsions, neurasthenia, and dehydration. The decision whether to hospitalize the patients was made by a hospital pediatrician after a clinical examination was performed in the pediatric emergency department. The clinical examination was used to confirm the diagnosis of acute diarrhea, which was defined as diarrhea (≥3 loose, or looser-than-normal, stools in a 24-hour period) [7]. Case notes for children admitted with a diagnosis of vomiting alone were reviewed to determine whether the children developed diarrhea 48 hours after admission. Dehydration was assessed for severity and was categorized as none, mild to moderate (3%–9%), or severe (≥10%), according to WHO criteria. The patients’ medical reports were provide by the hospital, and the meteorological information about rainfall in Tianjin was collected by consulting the National Bureau of Statistics of China [3, 8].
Stool specimens were collected within 48 h of admission to the hospital for all patients. All fecal samples were screened for enteropathogenic bacterial agents by conventional culture methods and polymerase chain reaction (PCR) assays described previously [9]. The stool specimens, which were reported to be free of pathogenic bacteria by the local investigators, were stored at −70°C and were transported frozen to the Institute of Health and Environmental Medicine for detection of viruses weekly. The study was approved by the local ethics committee, and consent was obtained from the parents of the children.
Detection of viruses
The stool samples were tested for the presence of RV, AdV, HucV (NoV and SaV), AstV, and human enteroviruses (EVs) using polymerase chain reaction (PCR) or reverse transcription PCR (RT-PCR) in the Institute laboratory. Viral RNA was extracted from stool supernatant using a QIAamp® Viral RNA Mini Kit (QIAGEN, Germany), and viral DNA was extracted using an E.Z.N.A® Viral DNA Kit (Omega Bio-Tek, USA). Both kits were used according to the manufacturer’s instructions. We used previously published methods and primers to detect RV [6], AdV [10], HucV [11], AstV [5], and the EVs [12].
Cell culture and PCR detection
The virus-positive specimens were confirmed by cell culturing after the (RT-)PCR. Virus isolation was performed by using three cell lines: MA-104, CaCO-2, and 293 cells. First, the 10% virus-positive stool suspensions were filtered using a sterile syringe filter (pore size 0.22 μm, Millipore, 25 mm). The RV- and AstV-positive filtrates were activated with 10 μg/ml (for RV) or 5 μg/ml (for AstV) porcine pancreas trypsin (Sigma, USA) at 37°C for 40 min. Monolayers were then inoculated with 150 μl of RV-positive or AstV-positive filtrates. After incubation for 1 h at 37°C, 1 ml of high-glucose Dulbecco’s modified Eagle medium (DMEM; for RV) or RPMI 1640 medium (for AstV) containing 2 μg/ml (for RV) or 5 μg/ml (for AstV) trypsin was added to each well. AdV isolation was similar to that for RV and AstV, but trypsin was not required. The culture fluids were harvested 2–5 days after infection and were serially inoculated onto the three cell lines until the fourth passage.
Viral gene amplification and sequence analyses were carried out using culture fluid from the final passage. (RT-)PCR was used to detect RV [13], AstV [14], and AdV [10, 14] in the culture fluids of the MA-104, CaCO-2, and 239 cell lines, respectively.
Nucleotide sequencing and phylogenetic analysis
Nucleotide sequencing was performed using a BigDye Terminator Cycle Sequencing Kit and an ABI PRISM 3730XL Genetic Analyzer (Applied Biosystems Inc., Foster City, USA). The final consensus sequence for each sample was aligned with homologous sequences in GenBank using the Clustal W method with the BioEdit program, and the identities between the aligned sequences were calculated.
Data analysis
The Statistical Package for the Social Sciences (SPSS) 17.0 was employed to perform statistical analysis on the collected data. The chi-square test, Fisher’s exact test, median test, and bivariate correlations were used to test for statistical significance. A P-value of less than 0.05 was considered significant.
Results
Molecular epidemiology of viral infections
A total of 766 fecal specimens were prospectively collected. Enteric viral infections were found in 356 of the 766 cases (46.48%), and mixed infections were detected in 8.09% of the patients. RV, AdV, NoV, and AstV were detected in 27.94%, 17.62%, 5.87%, and 3.39% of the 766 fecal specimens, respectively. Of the mixed infection cases, RV+AdV infections were the most common in 58.06% (36/62), followed by RV+NoV in 19.35%, and AdV+NoV in 12.90% of the cases. Two patients were infected by three viruses, one with RV+AdV+NoV, and the other with RV+AdV+AstV. SaV and EVs were not detected in any of the samples (Table 1).
The NoV genotypes all were GII, and of these, 80.65% (25/31) were GII-4/2006b and 19.35% were GII-3. The MA-104 cell supernatants were genotyped as RV by RT-PCR, and G1 was the most common serotype (41/54, 75.93%), followed by G3 (20.37%), G2 (1.85%), and G9 (1.85%). In 30 cases, the cell supernatants of the 293 cell line were positive for AdV, of which Ad41 was the most frequent infection type (86.67%), followed by Ad1 (13.33%). Of the CaCo-2 cell lysates, 19 cases had positive amplicons, and all were HAstV-1.
The GenBank accession numbers described in this study are GQ379132–GQ379155 (NoV), GU586154–GU586173 (AdV), HM473149–HM473174 (RV), and HM450036–HM450043 (AstV).
Age, sex, and regional distribution
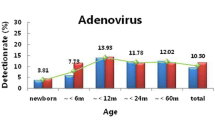
The median age of the 766 children was 7 months. Most of the children with acute diarrhea due to RV, AdV, NoV, and mixed viral infections were aged 7-12 months (38.9%, 40.4%, 53.8%, and 45.2%, respectively). The one exception was that most of the children with acute diarrhea due to AstV infections were aged 1-6 months (41.2%). Of the total viral infections, 87.9% occurred in children younger than 1 year old (Fig. 1).

Distribution of different viral infections by age. Different viral infections are indicated by the following symbols:  , group A rotaviruses;
, group A rotaviruses;  , enteric adenoviruses;
, enteric adenoviruses;  , mixed viral infection;
, mixed viral infection;  , norovirus;
, norovirus;  , astroviruses
, astroviruses
The sex ratio (male:female) was 1.73:1 for the 766 hospitalized pediatric patients. Among the 356 virus-positive patients, which included 237 boys (66.57%) and 119 girls (33.43%), there was a similar detection rate for both sexes (48.9% in boys vs. 42.4% in girls, P = 0.081). Of the total viral infections, the children who came from rural areas (52.2%) had a similar infection rate to the children from urban areas (47.8%) (P = 0.696) (Table 2).
Meteorological analysis
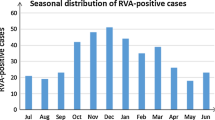
The single RV infections were distributed throughout the year, except for July, the peak occurred in October 2008 (43.66%), and the infection rate was inversely proportional to the amount of precipitation (Spearman r = −0.633, P = 0.020). AdV infection was detected throughout most of the year, and the cases peaked in July 2008 (57.89%). NoV infections peaked in November 2008 (14.71%). Mixed infections were detected throughout the year. Overall, there were more RV infections among children in the autumn (October–December) and winter (January–March) than in the summer (July–September). NoV had a high infection rate in the autumn, while AdV infections were highest in the summer. Most AstV and mixed infections occurred during the autumn and winter (Fig. 2).

Monthly distribution of target viruses in children with acute diarrhea. Rainfall and different viral infections are indicated by the following symbols:  , precipitation (mm);
, precipitation (mm);  , group A rotaviruses;
, group A rotaviruses;  , astroviruses;
, astroviruses;  , norovirus;
, norovirus;  , enteric adenoviruses;
, enteric adenoviruses;  , mixed viral infection
, mixed viral infection
Clinical characteristics
Diarrhea was the most common clinical feature (100%). Vomiting was observed in 163 patients and was more frequently observed in viral infection cases (45.79%, P = 0.030). Fever was detected in 254 virus infection cases and was more common (71.35%) than in non-virus infection (63.9%) cases (P = 0.028). Dehydration was diagnosed in 53 patients and was more frequent in virus infections (14.9% vs. 9.0%, P = 0.012) (Table 2). Patients with NoV and mixed infections were more prone to dehydration, but no dehydration was found in AstV-positive cases. Apart from mixed infections, duration of hospitalization for patients with diarrhea due to AstV (range: 3-39 days, median age: 10 days) was significantly longer than that due to RV, AdV, and NoV infections (P = 0.042) (Table 3).
Discussion
In this study, we observed that nearly half (46.48%) of the cases of diarrhea in children under five years old in Tianjin, China, were caused by at least one of the following four major viruses: RV, AdV, NoV, and AstV. The proportion of positive samples was higher than or equal to previous reports from different countries [9, 15]. RV was the most frequently detected infection at 27.94%, which was similar to the level of infection in Hong Kong [16] and India [17]. However, the level of infection was lower than that in other studies, which reported infections up to 54.0% [7, 18], and higher than that in France (17.3%) [15]. A previous report demonstrated that five RV genotypes (G1-G4, G9) were the most common globally [19]. In this study, we found that the G1-G3 and G9 strains were circulating in Tianjin, and G1 was the predominant strain. Fang et al. [20] found RV in 41% of stools, with the G1 serotype being the most common and boys also about twice as likely as girls to have it.
In many countries, the RV infection rate and the rate of hospitalization has decreased significantly due to use of the RV vaccine [21]. In China, the first RV vaccine was licensed and introduced in 2000, and it is a lamb-derived, monovalent (P[12]-G10), live-attenuated, 3-dose, oral vaccine [20]. After introduction of the RV vaccine, the RV infection rate decreased [2]. The WHO recommends that the RV vaccine should be included in all national immunization programs. In countries where diarrheal deaths account for ≥10% of the mortalities among children <5 years old, the introduction of the vaccine is strongly recommended. However, in China, RV vaccination is not mandatory, and it is not included in the Expanded Program on Immunization. In addition, non-mandatory attempts to propagate and adopt the vaccine have resulted in a low inoculation rate. In this study, we found that less than 1% of the children received RV vaccine.
AdV was the second most common agent of acute diarrhea (17.62%) in our population, and this result was similar to previous results in Germany (19.89%) [22] and higher than what has been observed in the UK (14%) [7]. In Tianjin, the prevailing AdV subtype was Ad41 (86.67%), and no Ad40 was detected. Although Ad40 was often detected in Iran and Bangladesh [23, 24], our findings were in line with previous reports from Hong Kong [15], Japan [25], and South Korea [26]. This phenomenon might reveal the occurrence of an antigenic drift of Ad41 [25] and/or the presence of environmental or geographical factors affecting all of these countries in Northeast Asia. In this study, the NoV detection frequency was 5.87%, which was lower than in some studies [22, 27] but very similar to previous results from China in Beijing [5], Lanzhou [4], and Shanghai [28]. Reports have indicated that the emergence of two novel GII-4 variants, 2006a and 2006b, was increasing globally [4, 29]. In this study, GII-4/2006b was the predominant circulating strain. A relatively low infection rate of AstV (3.39%) was detected, which is in agreement with previous reports [4, 30, 31]. Only AstV genotype 1 was detected during the molecular characterization of AstV in Tianjin, as has been reported previously [32, 33].
The mixed infection rate was 8.09% in this study, and RV was often present in patients who had mixed infections, as reported previously [15, 34]. Among the mixed infections, RV+AdV and RV+NoV were the major mixed infections in Tianjin, and these results were consistent other recent investigations [9, 27, 35].
Our results demonstrate that children younger than 1 year old are the most susceptible population to viral diarrhea. The majority of mixed viral infections occurred in the 7- to 12-month age group, which is similar to results reported in Germany [27]. We hypothesize that the potential reason for infections in young children involves the environmental sanitation of hospitals and/or family homes. Since babies suck their fingers, they can easily take in viruses that pollute the environment.
Viral diarrhea in Tianjin is happening more in dry and/or cold months, i.e., the spring, autumn and winter seasons. The viral diarrhea caused by RV and mixed viruses should be prevented in spring, autumn and winter. Prevention of NoV infection should be a particular concern in the autumn, and more attention should be paid to AdV in summer.
In children with viral diarrhea, the most common clinical features were diarrhea, fever, vomiting, and dehydration. The different single viral infections and mixed infections were similar in most of their clinical features except that in NoV and mixed diarrheal infections, dehydration was more common. Patients with AstV infections had a longer duration of hospitalization.
In conclusion, we have systematically and comprehensively studied the molecular epidemiology and clinical characteristics of acute viral diarrhea in Tianjin. We demonstrate that there is a high incidence of viral diarrhea, particularly due to RV infections in Tianjin. We recommend that preventing diarrhea in young children requires close attention. Most importantly, it is essential that the RV vaccine be included in the Expanded Program on Immunization. Simultaneously, it is essential to improve the environmental sanitation of hospitals and family homes in large cities like Tianjin, China, in developing countries.
References
Musher DM, Musher BL (2004) Contagious acute gastrointestinal infections. N Engl J Med 351:2417–2427
Yee EL, Fang ZY, Liu N, Hadler SC, Liang X, Wang H, Zhu X, Jiang B, Parashar U, Widdowson MA, Glass RI (2009) Importance and challenges of accurately counting rotavirus deaths in China, 2002. Vaccine 27(Suppl 5):F46–F49
China NBoSo (ed) (2009) China statistical yearbook
Jin Y, Cheng WX, Yang XM, Jin M, Zhang Q, Xu ZQ, Yu JM, Zhu L, Yang SH, Liu N, Cui SX, Fang ZY, Duan ZJ (2009) Viral agents associated with acute gastroenteritis in children hospitalized with diarrhea in Lanzhou, China. J Clin Virol 44:238–241
Liu C, Grillner L, Jonsson K, Linde A, Shen K, Lindell AT, Wirgart BZ, Johansen K (2006) Identification of viral agents associated with diarrhea in young children during a winter season in Beijing, China. J Clin Virol 35:69–72
Qiao H, Nilsson M, Abreu ER, Hedlund KO, Johansen K, Zaori G, Svensson L (1999) Viral diarrhea in children in Beijing, China. J Med Virol 57:390–396
Cunliffe NA, Booth JA, Elliot C, Lowe SJ, Sopwith W, Kitchin N, Nakagomi O, Nakagomi T, Hart CA, Regan M (2010) Healthcare-associated viral gastroenteritis among children in a large pediatric hospital, United Kingdom. Emerg Infect Dis 16:55–62
China NBoSo (2010) China statistical yearbook
Lee JI, Chung JY, Han TH, Song MO, Hwang ES (2007) Detection of human bocavirus in children hospitalized because of acute gastroenteritis. J Infect Dis 196:994–997
Rohayem J, Berger S, Juretzek T, Herchenroder O, Mogel M, Poppe M, Henker J, Rethwilm A (2004) A simple and rapid single-step multiplex RT-PCR to detect Norovirus, Astrovirus and Adenovirus in clinical stool samples. J Virol Methods 118:49–59
Yan H, Yagyu F, Okitsu S, Nishio O, Ushijima H (2003) Detection of norovirus (GI, GII), Sapovirus and astrovirus in fecal samples using reverse transcription single-round multiplex PCR. J Virol Methods 114:37–44
Caro V, Guillot S, Delpeyroux F, Crainic R (2001) Molecular strategy for ‘serotyping’ of human enteroviruses. J Gen Virol 82:79–91
O’Neill HJ, McCaughey C, Coyle PV, Wyatt DE, Mitchell F (2002) Clinical utility of nested multiplex RT-PCR for group F adenovirus, rotavirus and norwalk-like viruses in acute viral gastroenteritis in children and adults. J Clin Virol 25:335–343
Resque HR, Munford V, Castilho JG, Schmich H, Caruzo TA, Racz ML (2007) Molecular characterization of astrovirus in stool samples from children in Sao Paulo, Brazil. Mem Inst Oswaldo Cruz 102:969–974
Marie-Cardine A, Gourlain K, Mouterde O, Castignolles N, Hellot MF, Mallet E, Buffet-Janvresse C (2002) Epidemiology of acute viral gastroenteritis in children hospitalized in Rouen, France. Clin Infect Dis 34:1170–1178
Li CS, Chan PK, Tang JW (2009) Prevalence of diarrhea viruses in hospitalized children in Hong Kong in 2008. J Med Virol 81:1903–1911
Bahl R, Ray P, Subodh S, Shambharkar P, Saxena M, Parashar U, Gentsch J, Glass R, Bhan MK (2005) Incidence of severe rotavirus diarrhea in New Delhi, India, and G and P types of the infecting rotavirus strains. J Infect Dis 192(Suppl 1):S114–S119
Colomba C, De Grazia S, Giammanco GM, Saporito L, Scarlata F, Titone L, Arista S (2006) Viral gastroenteritis in children hospitalised in Sicily, Italy. Eur J Clin Microbiol Infect Dis 25:570–575
Santos N, Hoshino Y (2005) Global distribution of rotavirus serotypes/genotypes and its implication for the development and implementation of an effective rotavirus vaccine. Rev Med Virol 15:29–56
Fang ZY, Yang H, Qi J, Zhang J, Sun LW, Tang JY, Ma L, Du ZQ, He AH, Xie JP, Lu YY, Ji ZZ, Zhu BQ, Wu HY, Lin SE, Xie HP, Griffin DD, Ivanoff B, Glass RI, Gentsch JR (2002) Diversity of rotavirus strains among children with acute diarrhea in China: 1998–2000 surveillance study. J Clin Microbiol 40:1875–1878
Gurgel RG, Bohland AK, Vieira SC, Oliveira DM, Fontes PB, Barros VF, Ramos MF, Dove W, Nakagomi T, Nakagomi O, Correia JB, Cunliffe N, Cuevas LE (2009) Incidence of rotavirus and all-cause diarrhea in northeast Brazil following the introduction of a national vaccination program. Gastroenterology 137:1970–1975
Silva PA, Stark K, Mockenhaupt FP, Reither K, Weitzel T, Ignatius R, Saad E, Seidu-Korkor A, Bienzle U, Schreier E (2008) Molecular characterization of enteric viral agents from children in northern region of Ghana. J Med Virol 80:1790–1798
Dey SK, Shimizu H, Phan TG, Hayakawa Y, Islam A, Salim AF, Khan AR, Mizuguchi M, Okitsu S, Ushijima H (2009) Molecular epidemiology of adenovirus infection among infants and children with acute gastroenteritis in Dhaka City, Bangladesh. Infect Genet Evol 9:518–522
Saderi H, Roustai MH, Sabahi F, Sadeghizadeh M, Owlia P, De Jong JC (2002) Incidence of enteric adenovirus gastroenteritis in Iranian children. J Clin Virol 24:1–5
Shimizu H, Phan TG, Nishimura S, Okitsu S, Maneekarn N, Ushijima H (2007) An outbreak of adenovirus serotype 41 infection in infants and children with acute gastroenteritis in Maizuru City, Japan. Infect Genet Evol 7:279–284
Huh JW, Kim WH, Moon SG, Lee JB, Lim YH (2009) Viral etiology and incidence associated with acute gastroenteritis in a 5-year survey in Gyeonggi province, South Korea. J Clin Virol 44:152–156
Oh DY, Gaedicke G, Schreier E (2003) Viral agents of acute gastroenteritis in German children: prevalence and molecular diversity. J Med Virol 71:82–93
Xu J, Yang Y, Sun J, Ding Y (2009) Molecular epidemiology of norovirus infection among children with acute gastroenteritis in Shanghai, China, 2001–2005. J Med Virol 81:1826–1830
Tu ET, Bull RA, Greening GE, Hewitt J, Lyon MJ, Marshall JA, McIver CJ, Rawlinson WD, White PA (2008) Epidemics of gastroenteritis during 2006 were associated with the spread of norovirus GII.4 variants 2006a and 2006b. Clin Infect Dis 46:413–420
Papaventsis DC, Dove W, Cunliffe NA, Nakagomi O, Combe P, Grosjean P, Hart CA (2008) Human astrovirus gastroenteritis in children, Madagascar, 2004–2005. Emerg Infect Dis 14:844–846
Victoria M, Carvalho-Costa FA, Heinemann MB, Leite JP, Miagostovich MP (2007) Genotypes and molecular epidemiology of human astroviruses in hospitalized children with acute gastroenteritis in Rio de Janeiro, Brazil. J Med Virol 79:939–944
Mendez-Toss M, Griffin DD, Calva J, Contreras JF, Puerto FI, Mota F, Guiscafre H, Cedillo R, Munoz O, Herrera I, Lopez S, Arias CF (2004) Prevalence and genetic diversity of human astroviruses in Mexican children with symptomatic and asymptomatic infections. J Clin Microbiol 42:151–157
Mitchell DK, Matson DO, Jiang X, Berke T, Monroe SS, Carter MJ, Willcocks MM, Pickering LK (1999) Molecular epidemiology of childhood astrovirus infection in child care centers. J Infect Dis 180:514–517
Medici MC, Martinelli M, Arcangeletti MC, Pinardi F, De Conto F, Dodi I, Virdis R, Abelli LA, Aloisi A, Zerbini L, Valcavi P, Calderaro A, Bernasconi S, Izzi GC, Dettori G, Chezzi C (2004) Epidemiological aspects of human rotavirus infection in children hospitalized with acute gastroenteritis in an area of northern Italy. Acta Biomed 75:100–106
Roman E, Wilhelmi I, Colomina J, Villar J, Cilleruelo ML, Nebreda V, Del Alamo M, Sanchez-Fauquier A (2003) Acute viral gastroenteritis: proportion and clinical relevance of multiple infections in Spanish children. J Med Microbiol 52:435–440
Acknowledgments
This study was supported a Grant from National Natural Science Foundation of China (No. 30930078).
Author information
Authors and Affiliations
Corresponding authors
Additional information
Y. Ouyang and H. Ma contributed equally to the paper.
Rights and permissions
About this article
Cite this article
Ouyang, Y., Ma, H., Jin, M. et al. Etiology and epidemiology of viral diarrhea in children under the age of five hospitalized in Tianjin, China. Arch Virol 157, 881–887 (2012). https://doi.org/10.1007/s00705-012-1235-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00705-012-1235-9