
Abstract
Upon phylogenetic analysis of a partial S gene sequence [396 nucleotides (nt)], 928 hepatitis B virus (HBV) strains obtained from 899 viremic subjects in 28 major cities on 15 islands of Indonesia in 1989–2007 segregated into four HBV genotypes. Genotype B was predominant (66%), followed by genotype C (26%), genotype D (7%), and genotype A (0.8%). Comparative and phylogenetic analyses of the 396-nt S gene sequence of 928 HBV isolates and whole genomic sequences of 25 selected HBV isolates revealed a total of 14 subgenotypes within genotypes A–D: two (A1 and A2) in genotype A (HBV/A), five (B2, B3, B5, B7, and a novel subgenotype, tentatively designated B8) in HBV/B, five (C1, C2, C5, C6, and another novel subgenotype, C7) in HBV/C, and two (D1 and D3) in HBV/D. The distribution of HBV genotypes/subgenotypes, including B8 and C7, seems to be associated with ethnological origins in Indonesia.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Hepatitis B is a major worldwide health problem, with over 350 million chronically infected individuals, some of whom develop severe liver disease including cirrhosis and hepatocellular carcinoma. The prevalence of hepatitis B virus (HBV) infection is generally high in Asia and Africa [17]. Indonesia has a moderate to high endemicity of HBV infection. The carrier rates among apparently healthy populations in Indonesia have been reported to range from 4.0 to 20.3% [13]. Its prevalence varies by island; in general, areas outside of Java Island have a higher prevalence of hepatitis B surface antigen (HBsAg) (9.2%) than areas within Java (5.0%) [22].
Eight genotypes of HBV, designated A to H, have been identified worldwide [2, 3, 24, 29, 36]. The genotypes B and C (HBV/B and HBV/C, respectively) are predominant in Asia [14, 32, 34, 37]. Subgenotypes have been identified within certain HBV genotypes, i.e., A1–A4 in HBV/A, B1–B7 in HBV/B, C1–C6 in HBV/C, and D1–D6 in HBV/D, with distinct geographical clustering [15, 19, 25, 26, 33]. An earlier classification system divided HBsAg into four major serological subtypes, adw, adr, ayw, and ayr [4, 16]. There is a correlation between HBsAg subtypes and HBV genotypes. In general, infected individuals with HBV genotype of A, B, F, G, or H have subtype adw; those with HBV/C have adr; and those with HBV/D and HBV/E have ayw [14].
Indonesia, one of the largest archipelagos in the world, consists of more than 17,000 islands and is inhabited by more than 400 ethnic groups [38]. A previous study showed that the distribution of HBsAg subtypes varied greatly among the islands. Subtype adw, ayw, and adr were predominant in the western part of Indonesia, Moluccas, and Papua Indonesia, respectively [21]. The distribution of HBsAg subtypes suggested that there is a molecular diversity of HBV among the ethnic groups in Indonesia. However, a nationwide study on the distribution of HBV genotypes in Indonesia has thus far not been reported. The present study aimed to elucidate the nationwide distribution of HBV genotypes and subgenotypes in relation to HBsAg subtypes in Indonesia and to find an association between HBV genotypes/subgenotypes and ethnic groups.
Materials and methods
Serum samples
Serum samples collected from a total of 899 subjects with HBsAg [701 males and 198 females; age, mean ± standard deviation (SD), 30.8 ± 11.3 years; range, 7–75 years] living in 28 cities on 15 islands of Indonesia (see Fig. 3 for location) between 1989 and 2007 were used in the present study (Table 1). The presence of HBsAg was determined by passive hemagglutination with commercial assay kits [Entebe HBsAg (R-PHA), Hepatika Laboratory, Mataram, Indonesia or Mycell HBsAg, Institute of Immunology Co. Ltd., Tokyo, Japan]. Ethical approval of this investigation was obtained from the ethics committees of the Faculty of Medicine, Mataram University in Mataram, Indonesia, and Jichi Medical University in Tochigi, Japan.
Detection of HBV DNA and determination of HBV genotype/subgenotype and HBsAg subtype
The presence of HBV DNA was determined by the method described previously [40], with slight modifications. Briefly, nucleic acids were extracted from 100 µl of serum using a commercially available kit (SMITEST EX-R&D; G&G Science Co. Ltd., Fukushima, Japan) and were tested for the presence of HBV DNA by nested polymerase chain reaction (PCR) using primers derived from the well-conserved areas in the S gene region of the HBV genomes of all 8 genotypes (A–H) reported thus far [3, 24, 29, 36] and TaKaRa Ex Taq polymerase (TaKaRa Bio, Shiga, Japan). The amplification product of the first-round PCR was 461 base pairs (bp) (nt 244–704), and that of the second-round PCR was 437 bp (nt 251–687): nucleotide numbers correspond to those of a genotype C HBV isolate of 3,215 nt (AB033550).
The HBsAg subtype was determined based on the nucleotide sequence of codons 122 and 160 of the S gene [27, 28]. The HBV genotype/subgenotype was determined by phylogenetic analysis of the above-mentioned S gene sequence (396 nt; primer sequences at both ends excluded) in comparison with reported HBV isolates with known genotype/subgenotype (see Figs. 1, 2 for accession nos.) and 25 selected HBV isolates whose entire genomic sequences were determined in the present study (see Figs. 1, 2 for isolate names).

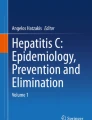
Phylogenetic tree constructed by the neighbor-joining method, based on the entire genomic sequence of 66 genotype B HBV isolates, using a genotype C HBV (AB033550) as an outgroup. In addition to the 13 Indonesian HBV isolates whose entire genomic sequences were determined in the present study and which are indicated in bold type for visual clarity, 53 representative HBV isolates of subgenotypes B1–B7 whose entire sequences are known, were included for comparison. The reported isolates are indicated with the accession no. followed by the name of the country where it was isolated. Bootstrap values are indicated for the major nodes as a percentage of the data obtained from 1,000 resamplings

Phylogenetic tree constructed by the neighbor-joining method based on the entire nucleotide sequence of 56 genotype C HBV isolates, using a genotype B HBV (D00329) as an outgroup. In addition to the 12 Indonesian HBV isolates whose entire genomic sequences were determined in the present study and which are indicated in bold type for visual clarity, 44 representative HBV isolates of subgenotypes C1–C5 whose entire sequences are known were included for comparison. The reported isolates are indicated with the accession no. followed by the name of the country of isolation. Bootstrap values are indicated for the major nodes as a percentage of the data obtained from 1,000 resamplings

Map of the Indonesian archipelago showing seven major zones. The 28 cities where serum samples were obtained are indicated. The seven major zones reflecting the distinct geographical distribution of HBV genotype/subgenotype and subtype in Indonesia are shaded
Detection of antibody to HDV and HDV RNA
The presence of antibodies to hepatitis delta virus (HDV) was determined using an in-house enzyme-linked immunosorbent assay (ELISA) with purified recombinant S-HDAg protein that had been expressed in the pupae of silkworm, as described previously [12]. The presence of HDV RNA was determined in RNAs extracted from 100 µl of test serum by reverse transcription (RT)-PCR with nested primers derived from conserved areas of all reported HDV genomes of genotypes I, II and III, as reported previously [40].
Amplification of the entire HBV genome
The complete nucleotide sequences of HBV genomes were determined by methods essentially similar to those described previously [10, 35]. Briefly, two overlapping regions of HBV DNA (primer sequences at both ends excluded) spanning nt 2332–3215 and 1–667 (1,551 bp) and nt 480–2380 (1,901 bp), respectively, were amplified by nested PCR with appropriate primers that had been derived from conserved areas of the HBV genomes of the eight genotypes (A–H) and TaKaRa Ex Taq polymerase.
Sequence analysis of PCR products
The amplification products were sequenced directly on both strands using the BigDye Terminator v3.1 Cycle Sequencing Kit on an ABI PRISM 3100 Genetic Analyzer (Applied Biosystems, Foster City, CA). When amplification products showed an ambiguous sequence, they were inserted into pT7Blue T-vector (TaKaRa Bio), and five independent clones of each were sequenced. Sequence analysis was performed using Genetyx-Mac version 12.2.7 (Genetyx Corp., Tokyo, Japan) and ODEN version 1.1.1 from the DNA Data Bank of Japan (DDBJ: National Institute of Genetics, Mishima, Japan) [11]. Sequence alignments were generated by CLUSTAL W (version 1.8) [41]. Phylogenetic trees were constructed by the neighbor-joining method [31]. Bootstrap values were determined on 1,000 resamplings of the data sets [8]. The final tree was obtained using the TreeView program (version 1.6.6) [30].
Results
Prevalence rate of HBV genotype in Indonesia
The prevalence rates of HBV genotypes among HBV-infected individuals in 28 cities on 15 islands covering nearly all major islands of Indonesia, are shown in Table 1. Among the eight known genotypes of HBV (A–H), a single genotype of A, B, C, or D was found in 873 (97%) of the 899 Indonesian HBsAg-positive subjects studied. Genotype B was predominant (66%), followed by genotype C (24%), genotype D (7%), and genotype A (0.4%); the remaining 26 subjects (3%) were infected with two or three distinct groups of HBV (see Table 4 for details). Genotype D was predominant in South Moluccas (Masohi and Ambon), while genotype A was found only in East Kalimantan (Balikpapan) and Timor (Kupang).
Presence of multiple subgenotypes within HBV genotypes A–D in Indonesia
Based on phylogenetic analyses of the 396-nt S gene sequence, 927 of the 928 HBV isolates, including those from 26 individuals with mixed infection, were grouped into 14 different sets of clusters of HBV genotypes A–D, i.e., two clusters each within genotypes A and D and five clusters each within genotypes B and C. The remaining one genotype C isolate [C0503133(DIL)] was not classified into any of the five clusters within genotype C. Upon comparison with known HBV/A isolates of subgenotypes A1–A4 whose entire genomic sequence is known, five of the seven HBV/A isolates obtained in the present study were 99.7–100% identical to subgenotype A2 isolates from the US (AB116078) and Japan (AB116079), and the remaining two isolates were 99.7–100% similar to a subgenotype A1 isolate from the Philippines (AY934774). When compared with known HBV/D isolates whose entire genomic sequence is known, the 65 HBV/D isolates obtained in the present study were divided into two groups (subgenotype D1, n = 32, and subgenotype D3, n = 33): the 32 subgenotype D1 isolates shared nucleotide sequence identities of 99.0–99.7% with a Chinese isolate of the same subgenotype (AF280817), and the 33 subgenotype D3 isolates shared nucleotide sequence identities of 99.5–100% with a representative European isolate of the same subgenotype (X65257). When the 615 HBV/B isolates found in the present study were compared within the 396-nt S gene sequence (Table 2), and when the entire genomic sequence (3,215 nt) of 13 selected HBV/B isolates was determined and compared phylogenetically with HBV/B isolates whose entire sequence is known (Fig. 1), 428 isolates (70%) were classified into subgenotype B3, represented by B0612746(JKT)F, whose entire genomic sequence was determined in the present study, 93 isolates (15%) into subgenotype B7, represented by B0607154(KDR)F, B0503213(MKS)F, B0715677(MMR)F, B0714202(BMA)F, and B0714189(WBK)F, 50 isolates (8%) into subgenotype B2, represented by B0503341(PTK)F, and five isolates (1%) into subgenotype B5, represented by B0503233(BJS)F and B0607171(KDR)F. The remaining 39 isolates (6%) were classified into a novel subgenotype, which was tentatively designated as B8 in the present study, represented by B0714157(WBK)F, B0308839(DPS)F, B0503102(DIL)F, and B0503138(KPG)F, with a bootstrap value of 100% (Fig. 1). Subgenotypes B1, B4, and B6 were not found in the studied population.
When the 241 HBV/C isolates obtained in the present study were compared within the 396-nt S gene sequence (Table 3), and when the entire genomic sequence (3,215 nt) of 12 selected HBV/C isolates was determined and subjected to phylogenetic analysis with HBV/C isolates whose entire sequence is known (Fig. 2), 106 isolates (44%) were grouped into subgenotype C1, represented by C0503296(PKT)F, 41 isolates (17%) into subgenotype C2, represented by C0714154(WBK)F, and 38 isolates (16%) into subgenotype C5, represented by C0503222(MND)F, C0715697(TNT)F, and C0607174(THN)F. Of note, 33 isolates (14%) were most closely related to the C6 (Papua) HBV/C isolates, whose subgenotype was provisionally designated as C6 based on their partial S gene and precore/core gene sequences [19], with identities of 97.6–99.4% within the overlapping 168-nt S sequence, and classified into subgenotype C6, represented by C0610090(BIK)F and C0610316(JYP)F, whose entire genomic sequence was determined in the present study. In addition, 22 isolates (9%) were classified into a novel subgenotype which was tentatively designated as C7 in the present study, represented by C0503236(BJS)F, C0503463(MTR)F, C0309374(DPS)F, and C0309392(DPS)F, with a bootstrap value of 100% (Fig. 2). The remaining one HBV/C isolate [C0503133(DIL)F] shared nucleotide sequence identities of only 94.5–95.7% with C1 isolates (n = 18), 95.2–96.5% with C2 isolates (n = 19), 95.5–95.9% with C3 isolates (n = 2), 93.7% with C4 isolates (n = 2), 94.1–94.4% with C5 isolates (n = 8), 95.5–95.9% with C6 isolates (n = 2), and 95.5–95.8% with C7 isolates (n = 4) over the entire genome (see Fig. 2 for accession nos.) and did not segregate into any clusters of HBV/C (Fig. 2), indicating that this particular HBV/C isolate may be classifiable into an eighth subgenotype within genotype C. However, since no other HBV isolate homologous to C0503133(DIL)F was available, this isolate was regarded as “Unclassified subgenotype of genotype C” in the current study.
Distribution of HBV genotype/subgenotype in Indonesia
Subgenotype B3 was distributed widely throughout Indonesia, being predominant in Sumatera and Java, and subgenotype B7 was scattered widely, with high prevalence in the southern part of Sulawesi (Kendari and Makassar), South Moluccas (Ambon and Masohi), Lombok (Mataram), Sumbawa (Sumbawa Besar and Bima), Sumba (Waikabubak), Flores (Maumere), and Timor (Kupang and Dili). Subgenotype B2 was also dispersed widely, with high prevalence in Sumatera (Bandar-Lampung), Java (Jakarta, Solo, Surabaya), Kalimantan (Pontianak), Lombok (Mataram), and Sumbawa (Bima), whereas subgenotype B5 was restricted to Sulawesi (Kendari) and Kalimantan (Banjarmasin). The novel subgenotype B8 was found mainly in Sumba, Flores and Timor Islands (Table 2). Subgenotype C1 was found to be dispersed throughout Indonesia, while subgenotype C2 was found mainly in Jakarta, Waikabubak, Maumere, Kupang, and Dili. Subgenotype C5 was found in the northern part of Sulawesi (Manado), Sangihe-Talaud (Tahuna), and North Moluccas (Ternate), whereas subgenotype C6 was found only in Papua Indonesia (Jayapura and Biak) (Table 3). The novel subgenotype C7 was found mainly in Jakarta, Kalimantan (Banjarmasin), Bali and Lombok Islands.
Reflecting the presence of multiple subgenotypes within genotypes A–D in Indonesia, 26 viremic subjects (3%) were infected with two or three distinct subgenotypes of HBV (Table 4). Of note, 11 (42%) of the 26 subjects had HBVs of predominant subgenotypes (B3 and C1) within each of the genotypes B and C.
Distribution of the HBsAg subtype in Indonesia
All four HBsAg subtypes (adw, adr, ayw, and ayr) were found in Indonesia, as shown in Table 5. Subtype adw was predominant in the western part of Indonesia (except for Padang, where adr was predominant); subtype ayw was predominant in the southern part of Sulawesi, South Moluccas, Lombok, Sumbawa, Sumba, Flores, and Timor; whereas adr was predominant in Papua Indonesia. Subtype ayr was found to be extremely rare; it was found in only 5 (1%) of 928 HBV isolates (2 in Jakarta, 2 in Manado, and 1 in Jayapura), including the 26 carriers with mixed HBV infection of different genotypes/subgenotypes (Tables 4, 5).
All seven HBV/A isolates and 65 HBV/D isolates were typed as adw and ayw, respectively, irrespective of the subgenotype, while 67% of the 615 HBV/B isolates and 79% of the 241 HBV/C isolates were typed as adw and adr, respectively (Table 6). Analysis of the association between HBsAg subtypes and subgenotypes showed that the predominant subtype of subgenotypes B2 and B3 was adw, accounting for 98 and 84% of each subgenotype, respectively, while the subtype in subgenotypes B5, B7 and B8 was exclusively ayw. The predominant subtype of subgenotypes C1, C2, C6, and C7 was adr, accounting for 85–100% of each subgenotype, while the subtype in all 38 subgenotype C5 isolates was adw. Table 6 indicates that subtypic determinant ‘r’ had a close association with genotype C, while subtypic determinant ‘w’ was associated with all four genotypes (A–D).
HDV infection in Indonesia
As for HDV infection in Indonesia, seven HBV-viremic subjects (0.8%) were reproducibly positive for anti-HDV antibodies. However, none had detectable HDV RNA, suggesting infrequent, if any, HDV infection in HBV-infected individuals in Indonesia.
Discussion
Previous studies showed that there were only three HBV genotypes (B, C, and D) in Indonesia [1, 18, 19, 26, 34]. However, the present study indicated that at least four major genotypes (A, B, C, and D) are present in Indonesia, although genotypes A and D were infrequent, and co-infection of HDV was at a negligible level. The present study also revealed the presence of a total of 14 subgenotypes within genotypes A–D in Indonesia, including two novel subgenotypes, B8 and C7, which were provisionally designated as the eighth subgenotype of genotype B and seventh subgenotype of genotype C, respectively, in the current study. It was reported that, for some HBV strains, analysis of S gene sequences alone might not be sufficient to classify HBV isolates into subgenotypes [25]. In the present study, however, one to five representative isolates were randomly selected from each of the phylogentic clusters (subgenotypes) that were generated based on the 396-nt S gene sequence, and their entire nucleotide sequences were determined to validate the appropriateness of the subgenotypic groupings. Notably, with regard to each of the 10 subgenotypes of genotypes B and C found in Indonesia, all HBV isolates of a particular subgenotype were more closely related to the representative isolate(s) of the subgenotype whose entire genomic sequence was determined than to the other subgenotypes.
Of the two HBV genotypes (B and C) found frequently in Indonesia, there was a remarkable difference in their subgenotype frequencies. The five subgenotypes within genotype B (B2, B3, B5, B7 and B8) were distributed unevenly in Indonesia. Among them, subgenotype B3 was most predominant (70%), followed by subgenotype B7 (15%), and the remaining three subgenotypes accounted for 15% (B2, 8%; B8, 6%; and B5, 1%). In contrast to genotype B, the five subgenotypes of genotype C (C1, C2, C5, C6, and C7) were observed at somewhat similar frequency. Among these five subgenotypes of genotype C, the most predominant subgenotype (C1) accounted for only 44%, followed by subgenotypes C2 (17%), C5 (16%), C6 (14%), and C7 (9%). Among the 14 subgenotypes found in the present study, subgenotype B3 accounted for 46%. HBV of subgenotype B3 (HBV/B3) was distributed widely throughout Indonesia, except for Biak in Papua (Table 2), and has not been reported in countries other than Indonesia. Taken altogether, it is very likely that HBV/B3 is indigenous to Indonesia. In contrast, subgenotypes B2, C1, and C2, accounting for 5, 11, and 4%, respectively, of the studied population, are distributed in many Asian countries including China where subgenotypes B2, C1 and C2 prevail [42], suggesting that HBV of these three subgenotypes may have been imported from neighboring Asian countries in the past.
Subgenotype B5, represented by B0503233(BJS)F and B0607171(KDR)F, has thus far been reported only in the Philippines [32] and was found to be restricted to Kalimantan (Banjarmasin) and Sulawesi (Kendari) in the present study. Subgenotype C5, represented by C0503222(MND)F, C0715607(TNT)F, and C0607174(THN)F, was found only in the northern part of Sulawesi (Manado), Sangihe-Talaud (Tahuna), and North Moluccas (Ternate), corroborating the previous study by Achwan et al. [1] who reported the presence of HBV of subgenotype C5 (HBV/C5) in Tahuna. HBV/C5 has also been reported in the Philippines [32] and Vietnam [9]. Interestingly, anthropologic evidence shows a close relationship between Filipino and Vietnamese peoples [5]. Hence, it seems likely that the inhabitants living in the northern part of Sulawesi, Sangihe-Talaud, and North Moluccas had originally come from Vietnam and directly migrated to Indonesia or via the Philippines. Alternatively, since HBV/C5 isolates in Indonesia were phylogenetically closer to those in the Philippines than those in Vietnam (Fig. 2), and since Tahuna, Manado, and Ternate are located adjacent to Mindanao Island of the Philippines, HBV/C5 and HBV/B5 may have simply been imported from the Philippines or vice versa, or each subgenotype may have been derived from a common ancestor as the respective subgenotype in the Philippines.
Of note, subgenotype B7, represented by B0607154(KDR)F, B0503213(MKS)F, B0715677(MMR)F, B0714202(BMA)F, and B0714189(WBK)F, were found to be distributed not only in West Nusa Tenggara, including Lombok and Sumbawa Islands, and East Nusa Tenggara including Sumba, Flores, and Timor Islands, where Nurainy et al. [26] first identified HBV/B7, but also in the southern part of Sulawesi and South Moluccas. A novel subgenotype of genotype B (B8), represented by B0714157(WBK)F, B0308839(DPS)F, B0503102(DIL)F, and B0503138(KPG)F, was identified mainly in East Nusa Tenggara. Lusida et al. [19] reported the presence of HBV/C6 in Papua, although only a partial sequence of the HBV genome was determined. In the present study, 33 HBV isolates classifiable into subgenotype C6 in Jayapura and Biak in Papua were found, and the entire genomic sequences of two representative HBV/C6 isolates, C0610090(BIK)F and C0610316(JYP)F, were determined. HBV/C6 isolates were not identified in any of the other cities on the 14 islands studied in Indonesia, suggesting that HBV/C6 is indigenous to Papua. Of interest, a novel subgenotype of genotype C (C7) represented by C0503236(BJS)F, C0503463(MTR)F, C0309374(DPS)F, and C0309392(DPS)F was identified in the present study. However, it remains unclear why HBV/C7 was distributed separately in particular places including Java (Jakarta), Kalimantan (Banjarmasin), Bali, and Lombok.
There are more than 400 ethnic groups and languages in Indonesia [38]. The present study enabled us to assess whether the distribution of HBV genotypes/subgenotypes reflects the national motto of Indonesia, i.e., “Bhinneka Tunggal Ika” or “Unity in diversity”. Courouce-Pauty et al. [7] and Mazzur et al. [20] showed that the geographical distribution of HBsAg subtypes can provide valuable information on ancestral migration. In a previous study [21], Indonesia was divided into four different zones based on the distribution of HBsAg subtypes, i.e., the adw-dominant zone, adr zone, ayw zone, and mixed-subtype zone. In the present study, based on the distribution and predominance of HBV genotypes/subgenotypes, the four subtype-based zones were found to be further divided into several subzones. The adw zone was divided into the B3/adw-dominant subzone in Sumatera, Bangka, Java, and Bali Islands and the C5/adw subzone in the northern part of Sulawesi (Manado), Sangihe-Talaud (Tahuna), and North Moluccas (Ternate). Padang in Sumatera was an exception, where C1/adr predominated, although it is far from the adr zone, consistent with the previous report [21]. The ayw zone was divided into the D/ayw subzone in South Moluccas, B7/ayw subzone in West Nusa Tenggara and B7/ayw&B8/ayw subzone in East Nusa Tenggara. The adr zone was rich in C6/adr in Papua (Jayapura and Biak). A mixed-subtype zone where the frequencies of adw, ayw, and adr were comparable (Kalimantan and southern part of Sulawesi) was found to be rich in B3/adw, B7/ayw and C1/adr.
The genotype/subgenotype/subtype-based subzones found in the present study may support further tracing of the migration of Indonesian ancestors. Although there are some theories about the origin of the Indonesian population, one of the most accepted theories is that proposed by Brandes [6]. According to Brandes, the inhabitants occupying Indonesia consist of people who originated from language speakers of Stocks Austronesia. Stocks Austronesia is divided into Substocks West Austronesia and East Austronesia. The Substocks West Austronesia populations occupied the western part of Indonesia from Sumatera to Kalimantan, Bali and West Nusa Tenggara Islands, where B3/adw is predominant (Table 2), while Substocks East Austronesia populations occupied the eastern part of Indonesia from Sulawesi to Nusa Tenggara and South Moluccas, where B7/ayw and B8/ayw prevail (Table 2). Of interest, the distribution of HBV/C7, which was seen in Banjarmasin, Denpasar, Mataram, and Sumbawa Besar, is consistent with the distribution of language speakers of the subfamily of Bali-Sasak-Sumbawa, which is a member of substock West Austronesia. Although it has not been reported thus far whether subgenotype C6 is also predominant in Papua New Guinea and Melanesia, it is possible that the ancestors of Papua Indonesia inhabitants originated from Papua New Guinea and Melanesia, where HBsAg with subtype adr predominate [23]. In support of this speculation, HBV isolates of compound subtype adwr, which share the highest nucleotide identity of 98.2% within the entire S gene sequence with subgenotype C6 isolates [C0610090(BIK)F and C0610316(JYP)F] among HBV isolates of all seven subgenotypes within genotype C, were obtained in Papua New Guinea [27]. According to the Summer Institute of Linguistics [39], the inhabitants of Papua Indonesia originated from language speakers of Stocks Austronesia and non-Austronesia. It is tempting to speculate that HBV carriers of subgenotype C6 in Papua are of the non-Austronesian-speaking group and those of subgenotype B3, B7, C1, or C2 in Papua are of the Austronesian-speaking group. To elucidate this interesting issue, further studies using HBV-positive serum samples obtained from various areas in Papua Indonesia as well as Papua New Guinea, Melanesia, Polynesia and the other islands are required.
Although the reason why HBV/A was distributed mainly in Balikpapan remains unknown, the presence of HBV/D in South Moluccas may be attributable to importation in accordance with the migration of Europeans (The Netherlanders), who came to South Moluccas around 400 years ago. In support of this, 26 HBV/D3 isolates in South Moluccas shared nucleotide sequence identities of 99.5–100% with a representative European isolate of the same subgenotype (X65257).
In conclusion, the present nationwide study on HBV genotypes/subgenotypes in Indonesia revealed the presence of a total of 14 subgenotypes within genotypes A–D, including two novel subgenotypes (tentatively designated B8 and C7) and suggested that the distribution of HBV genotypes/subgenotypes is associated with ethnological origins in Indonesia. The identification of an HBV isolate [C0503133(DIL)F] of unclassifiable subgenotype of genotype C in the present study suggests that further studies with greater number of samples in examined and unexamined areas would contribute to the discovery of HBV strains of novel subgenotype(s) or even of novel genotype(s) in Indonesia that may be closely related to particular ethnic groups.
References
Achwan WA, Muttaqin Z, Zakaria E, Depamede SA, Mulyanto Sumoharjo S, Tsuda F, Takahashi K, Abe N, Mishiro S (2007) Epidemiology of hepatitis B, C, and E viruses and human immunodeficiency virus infections in Tahuna, Sangihe-Talaud Archipelago, Indonesia. Intervirology 50:408–411
Arauz-Ruiz P, Norder H, Visoná KA, Magnius LO (1997) Molecular epidemiology of hepatitis B virus in Central America reflected in the genetic variability of the small S gene. J Infect Dis 176:851–858
Arauz-Ruiz P, Norder H, Robertson BH, Magnius LO (2002) Genotype H: a new Amerindian genotype of hepatitis B virus revealed in Central America. J Gen Virol 83:2059–2073
Bancroft WH, Mundon FK, Russell PK (1972) Detection of additional antigenic determinants of hepatitis B antigen. J Immunol 109:842–848
Bellwood P (1997) Prehistory of the Indo-Malaysian Archipelago, 2nd edn. University of Hawaii Press, Honolulu
Brandes JLA (1884) Contribution of the lexicon comparison to the western part of Malaysian-Polynesian Language Family. PhD Thesis, University of Utrecht, Utrecht, The Netherland (in Dutch)
Couroucé-Pauty AM, Plançon A, Soulier JP (1983) Distribution of HBsAg subtypes in the world. Vox Sang 44:197–211
Felsenstein J (1985) Confidence limits on phylogenies: an approach using the bootstrap. Evolution 39:783–791
Hannoun C, Norder H, Lindh M (2006) An aberrant genotype revealed in recombinant hepatitis B virus strains from Vietnam. J Gen Virol 81:2267–2272
Horikita M, Itoh S, Yamamoto K, Shibayama T, Tsuda F, Okamoto H (1994) Differences in the entire nucleotide sequence between hepatitis B virus genomes from carriers positive for antibody to hepatitis B e antigen with and without active disease. J Med Virol 44:96–103
Ina Y (1994) ODEN: a program package for molecular evolutionary analysis and database search of DNA and amino acid sequences. Comput Appl Biosci 10:11–12
Inoue J, Takahashi M, Nishizawa T, Narantuya L, Sakuma M, Kagawa Y, Shimosegawa T, Okamoto H (2005) High prevalence of hepatitis delta virus infection detectable by enzyme immunoassay among apparently healthy individuals in Mongolia. J Med Virol 76:333–340
Khan M, Dong JJ, Acharya SK, Dhagwahdorj Y, Abbas Z, Jafri SMW, Mulyono DH, Tozun N, Sarin SK (2004) Hepatology issues in Asia: perspectives from regional leaders. J Gastroenterol Hepatol 19:S419–S430
Kramvis A, Kew M, François G (2005) Hepatitis B virus genotypes. Vaccine 23:2409–2423
Kramvis A, Arakawa K, Yu MC, Nogueira R, Stram DO, Kew MC (2008) Relationship of serological subtype, basic core promoter and precore mutations to genotypes/subgenotypes of hepatitis B virus. J Med Virol 80:27–46
Le Bouvier GL (1971) The heterogeneity of Australia antigen. J Infect Dis 123:671–675
Lee WM (1997) Hepatitis B virus infection. N Engl J Med 337:1733–1745
Lusida MI, Surayah, Sakugawa H, Nagano-Fujii M, Soetjipto, Mulyanto, Handajani R, Boediwarsono, Setiawan PB, Nidom CA, Ohgimoto S, Hotta H (2003) Genotype and subtype analysis of hepatitis B virus (HBV) and possible co-infection of HBV and hepatitis C virus (HCV) or hepatitis D virus (HDV) in blood donors, patients with chronic liver disease patients on hemodialysis in Surabaya, Indonesia. Microbiol Immunol 47:969–975
Lusida MI, Nugrahaputra VE, Soetjipto, Handajani R, Nagano-Fujii M, Sasayama T, Utsumi T, Hotta H (2008) Novel subgenotypes of hepatitis B virus genotypes C and D in Papua, Indonesia. J Clin Microbiol 46:2160–2166
Mazzur S, Bastiaans MJ, Nath N (1981) Hepatitis B virus (HBV) infection among children and adults in the Solomon Islands. Am J Epidemiol 113:510–519
Mulyanto, Tsuda F, Karossi AT, Soewignyo S, Roestamsjah, Sumarsidi D, Trisnamurti RH, Sumardi, Surayah K, Udin LZ, Melani-Wikanta, Kanai K, Mishiro S (1997) Distribution of the Hepatitis B surface antigen subtypes in Indonesia: implications for ethnic heterogeneity and infection control measures. Arch Virol 142:2121–2129
Mulyanto, Surayah K, Depamede SN, Lestarini IA, Budianto W, Hafiludin, Umi K, Tsuda F, Takahashi M, Okamoto H (2008) Hepatitis B virus infection in Eastern part of Indonesia. Abstract book of the second China–Indonesia joint international symposium on hepatobiliary medicine and surgery, Chongqing, China
Nishioka K (1984) Predominant mode of transmission of hepatitis B virus: perinatal transmission in Asia. In: Vyas GN, Dienstag JL, Hoofnagle JB (eds) Viral hepatitis and liver disease. Grune & Stratton, Orlando, pp 423–432
Norder H, Couroucé AM, Magnius LO (1994) Complete genomes, phylogenetic relatedness, and structural proteins of six strains of the hepatitis B virus, four of which represent two new genotypes. Virology 198:489–503
Norder H, Couroucé AM, Coursaget P, Echevarria JM, Lee SD, Mushahwar IK, Robertson BH, Locarnini S, Magnius LO (2004) Genetic diversity of hepatitis B virus strains derived worldwide: genotypes, subgenotypes, and HBsAg subtypes. Intervirology 47:289–309
Nurainy N, Muljono DH, Sudoyo H, Marzuki S (2008) Genetic study of hepatitis B virus in Indonesia reveals a new subgenotype of genotype B in east Nusa Tenggara. Arch Virol 153:1057–1065
Okamoto H, Imai M, Tsuda F, Tanaka T, Miyakawa Y, Mayumi M (1987) Point mutation in the S gene of hepatitis B virus for a d/y or w/r subtypic change in two blood donors carrying a surface antigen of compound subtype adyr or adwr. J Virol 61:3030–3034
Okamoto H, Imai M, Miyakawa Y, Mayumi M (1987) Site-directed mutagenesis of hepatitis B surface antigen sequence at codon 160 from arginine to lysine for conversion of subtypic determinant from r to w. Biochem Biophys Res Commun 148:500–504
Okamoto H, Tsuda F, Sakugawa H, Sastrosoewignjo RI, Imai M, Miyakawa Y, Mayumi M (1988) Typing hepatitis B virus by homology in nucleotide sequence: comparison of surface antigen subtypes. J Gen Virol 69:2575–2583
Page RDM (1996) TREEVIEW: an application to display phylogenetic trees on personal computers. Comput Appl Biosci 12:357–358
Saitou N, Nei M (1987) The neighbor-joining method: a new method for reconstructing phylogenetic trees. Mol Biol Evol 4:406–425
Sakamoto S, Tanaka Y, Orito E, Co J, Clavio J, Ito K, Ozasa A, Quino A, Ueda R, Sollano J, Mizokami M (2006) Novel subtypes (subgenotypes) of hepatitis B virus genotypes B and C among chronic liver disease patients in the Philippines. J Gen Virol 87:1873–1882
Sakamoto T, Tanaka Y, Simonetti J, Osiowy C, Borresen ML, Koch A, Kurbanov F, Sugiyama M, Minuk GY, McMahon BJ, Joh T, Mizokami M (2007) Classification of hepatitis B virus genotype B into 2 major types based on characterization of a novel subgenotype in Arctic indigenous populations. J Infect Dis 196:1487–1492
Sastrosoewignjo RI, Sandjaja B, Okamoto H (1991) Molecular epidemiology of hepatitis B virus in Indonesia. J Gastroenterol Hepatol 6:491–498
Shibayama T, Masuda G, Ajisawa A, Hiruma K, Tsuda F, Nishizawa T, Takahashi M, Okamoto H (2005) Characterization of seven genotypes (A to E, G and H) of hepatitis B virus recovered from Japanese patients infected with human immunodeficiency virus type 1. J Med Virol 76:24–32
Stuyver L, De Gendt S, Van Geyt C, Zoulim F, Fried M, Schinazi RF, Rossau R (2000) A new genotype of hepatitis B virus: complete genome and phylogenetic relatedness. J Gen Virol 81:67–74
Sugauchi F, Mizokami M, Orito E, Ohno T, Kato H, Suzuki S, Kimura Y, Ueda R, Butterworth LA, Cooksley WG (2001) A novel variant genotype C of hepatitis B virus identified in isolates from Australian Aborigines: complete genome sequence and phylogenetic relatedness. J Gen Virol 82:883–892
Sugono D (2008) The mapping of languages in Indonesia. Language Center Press, Jakarta, p 7
Summer Institute of Linguistics (2006) Languages in Indonesia. SIL, Jakarta
Takahashi M, Nishizawa T, Gotanda Y, Tsuda F, Komatsu F, Kawabata T, Hasegawa K, Altankhuu M, Chimedregzen U, Narantuya L, Hoshino H, Hino K, Kagawa Y, Okamoto H (2004) High prevalence of antibodies to hepatitis A and E viruses and viremia of hepatitis B, C, and D viruses among apparently healthy populations in Mongolia. Clin Diagn Lab Immunol 11:392–398
Thompson JD, Higgins DG, Gibson TJ (1994) CLUSTAL W: improving the sensitivity of progressive multiple sequence alignment through sequence weighting, position-specific gap penalties and weight matrix choice. Nucleic Acids Res 22:4673–4680
Wang Z, Huang Y, Wen S, Zhou B, Hou J (2007) Hepatitis B virus genotypes and subgenotypes in China. Hepatol Res 37(s1):S36–S41
Acknowledgments
This study was supported in part by a grant from the Ministry of Education, Culture, Sports, Science and Technology of Japan. The authors are grateful to Dr. Patiiha and Dr. Achwan WA as well as all of the people who helped us to collect blood samples for their invaluable contributions.
Author information
Authors and Affiliations
Corresponding author
Additional information
The nucleotide sequence data reported in this study have been assigned DDBJ/EMBL/GenBank accession numbers AP011084–AP011108 for 25 entire HBV genomes and AB466339–AB467266 for 928 partial HBV sequences.
Rights and permissions
About this article
Cite this article
Mulyanto, Depamede, S.N., Surayah, K. et al. A nationwide molecular epidemiological study on hepatitis B virus in Indonesia: identification of two novel subgenotypes, B8 and C7. Arch Virol 154, 1047–1059 (2009). https://doi.org/10.1007/s00705-009-0406-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00705-009-0406-9