
Abstract
ITIH3 and ITIH4 are involved in the stabilization of the extracellular matrix. Several genome-wide association studies and case–control studies regarding psychiatric disorders have identified ITIH3 and ITIH4 single nucleotide polymorphisms (SNPs). The present case–control study examined the relationship between ITIH3 SNPs rs2535629 and rs736408 and ITIH4 SNPs rs3821831 and rs2239547 and depressive symptoms during pregnancy in Japan. Cases comprised 273 women with depressive symptoms during pregnancy defined as a Center for Epidemiological Studies Depression Scale (CES-D) score ≥ 16. Control subjects comprised 1176 women without depressive symptoms during pregnancy, according to the CES-D criteria, who had not been diagnosed with depression by a doctor. Adjustment was made for age, gestation at baseline, region of residence, the presence of children, family structure, smoking, employment, and education. Compared with the TT genotype of ITIH4 SNP rs2239547, the CC genotype was significantly related to a reduced risk of depressive symptoms during pregnancy: the adjusted odds ratio (95% CI) was 0.84 (0.63–1.11) for the TC genotype and 0.57 (0.36–0.91) for the CC genotype. ITIH3 SNPs rs2535629 and rs736408 and ITIH4 SNP rs3821831 were not related to depressive symptoms during pregnancy. The GCCT haplotype of rs2535629, rs736408, rs3821831, and rs2239547 was significantly positively associated with depressive symptoms during pregnancy. A significant interaction was found between rs2239547 and the presence of children. This is the first study to show significant associations of ITIH4 SNP rs2239547 and the GCCT haplotype with depressive symptoms during pregnancy. The effect of the presence of children might depend on rs2239547.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
In 2011, ITIH3 single nucleotide polymorphism (SNP) rs736408 was identified in a combined genome-wide association study (GWAS) analysis of schizophrenia and bipolar disorder (Psychiatric GWAS Consortium Bipolar Disorder Working Group 2011) while ITIH4 SNP rs2239547 was detected in another joint GWAS analysis of schizophrenia and bipolar disorder (Schizophrenia Psychiatric GWAS Consortium 2011). ITIH3 SNP rs2535629 was most strongly associated with five psychiatric disorder groups in the Psychiatric Genomics Consortium: autism spectrum disorder, attention-deficit-hyperactivity disorder, bipolar disorder, major depressive disorder, and schizophrenia in a GWAS (Cross-Disorder Group of the Psychiatric Genomics Consortium 2013). In a case–control study in China, ITIH4 SNP rs3821831 was significantly related to major depressive disorder (He et al. 2014).
ITIH3 and ITIH4 are located on chromosome 3p21.1. ITIH3 and ITIH4 are inter-alpha-trypsin inhibitor heavy chain (ITIH) proteins involved in the stabilization of the extracellular matrix (Salier et al. 1996; Bost et al. 1998). Serum levels of ITIH4 were associated with depressive disorder (Lee et al. 2015; Wang et al. 2016). In addition, ITIH4 is suggested as a biomarker of neuro-inflammation (Kashyap et al. 2009; Yang et al. 2012).
From the perspective of the absence of epidemiological information regarding the associations of ITIH3 SNPs rs2535629 and rs736408 and ITIH4 SNPs rs3821831 and rs2239547 with depressive symptoms during pregnancy, the present case–control study investigated this issue in Japan using data from the Kyushu Okinawa Maternal and Child Health Study (KOMCHS). Furthermore, a haplotype analysis was performed, and the possibility of an interaction between the SNP and the presence of children, which was inversely related to depressive symptoms during pregnancy in this population, was examined.
Methods
Study population
The KOMCHS is an ongoing prospective prebirth cohort study. Details of the baseline survey of the KOMCHS were described previously (Miyake et al. 2013; Kawasaki et al. 2017). Eligible women were those who became pregnant while living in one of seven prefectures on Kyushu Island in southern Japan, with a total population of approximately 13.26 million, or in Okinawa Prefecture, an island chain in the southwest of Japan, with a total population of nearly 1.37 million. Between April 2007 and March 2008, we requested that 423 obstetric hospitals in the above-mentioned eight prefectures provide as many pregnant women as possible with a set of leaflets explaining the KOMCHS, an application form to participate in the study, and a self-addressed and stamped return envelope. Pregnant women who were willing to participate in the KOMCHS returned the application form to the data management center. In total, 1757 pregnant women between the 5th and 39th weeks of pregnancy gave their written informed consent to participate in the KOMCHS and completed the baseline survey. Around 4 months after delivery, 1492 women gave informed consent for genotyping. The KOMCHS was approved by the ethics committees of the Faculty of Medicine at Fukuoka University and Ehime University Graduate School of Medicine.
Selection of cases and control subjects
In the baseline survey, each participant filled out a self-administered questionnaire and mailed the completed questionnaire to the data management center. Research technicians completed missing or illogical data by telephone interview.
The questionnaire included a Japanese version (Shima et al. 1985) of the Center for Epidemiologic Studies Depression Scale (CES-D) (Radloff 1977). The CES-D consists of 20 questions addressing six typical symptoms of depression experienced during the preceding week, including depressed mood, feelings of guilt or worthlessness, helplessness or hopelessness, psychomotor retardation, loss of appetite, and sleep disturbance. Each question is scored on a scale of 0–3 according to the frequency of the symptom, and the total CES-D score ranges from 0 to 60. Based on the validation study (Radloff 1977; Shima et al. 1985), a score of 16 or more on the CES-D is considered indicative of depressive symptoms. A history of smoking was defined as having smoked at least once per day for at least 1 year. Information on employment status was elicited for the year in which the questionnaire was conducted and for the preceding year; women were classified as unemployed if they were unemployed both in the year in which the questionnaire was completed and in the preceding year.
According to the above-mentioned definition, 273 cases of depressive symptoms during pregnancy were identified among the 1492 women. Among the remaining women, who would serve as control subjects, 42 women were excluded who were not considered to have depressive symptoms during pregnancy as defined by the CES-D but who had answered “yes” to the question: “Have you ever been diagnosed by a physician as having depression?” Additionally, one woman with incomplete data on smoking was excluded. The final analysis comprised 273 cases and 1176 control subjects.
DNA extraction and genotyping
Genomic DNA from buccal specimens collected with BuccalAmp swabs (Epicenter BioTechnologies, Madison, WI, USA) was extracted using a QIAmp DNA mini kit (Qiagen, Inc., Valencia, CA, USA). Genotyping of ITIH3 SNPs rs2535629 and rs736408 and ITIH4 SNPs rs3821831 and rs2239547 was performed using TaqMan SNP Genotyping Assays on the StepOnePlus machine (Applied Biosystems, Foster City, CA, USA), according to the manufacturer’s instructions.
Statistical analysis
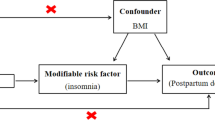
We tested for agreement with Hardy–Weinberg equilibrium among the control subjects using the Chi-square test. Linkage disequilibrium was examined using Haploview software version 4.2 (Broad Institute, Cambridge, MA, USA) (Barrett et al. 2005). Logistic regression analysis was performed to estimate crude odds ratios (ORs) and 95% confidence intervals (CIs) for depressive symptoms during pregnancy relative to the SNPs under investigation, with the reference category being the homozygote of the major allele. Multiple logistic regression analysis was employed to control for age, gestation at baseline, region of residence, the presence of children, family structure, smoking, employment, and education; these variables were selected a priori as potential confounding factors. The statistical power calculation was performed using QUANTO version 1.2 (Gauderman 2002). Haplotypes and their frequencies were inferred according to the expectation maximization algorithm. For differences in haplotype frequency between the cases and control groups, crude ORs and 95% CIs were estimated based on the frequency of each haplotype relative to all other haplotypes combined. The multiplicative interaction was tested using a term of the product of ITIH4 SNP rs2239547 and the presence of children together with terms of the products of the other confounding factors and the presence of children and the products of the other confounding factors and SNP rs2239547 in a multiple logistic regression model (Keller 2014). Excluding the calculation of linkage disequilibrium and statistical power calculation, all statistical analyses were carried out using STATA/SE software version 13.1 (StataCorp, College Station, TX, USA).
Results
Compared with control subjects, case subjects were more likely to be younger, to participate in the baseline survey at earlier gestational age, and to have ever smoked and were less likely to have one or more children and to be educated (Table 1). There were no differences between case and control subjects with regard to region of residence, family structure, and employment.
Among the control subjects, the genetic distributions of ITIH3 SNPs rs2535629 and rs736408 and ITIH4 SNPs rs3821831 and rs2239547 did not deviate from Hardy–Weinberg equilibrium (P = 0.91, 0.81, 0.07, and 0.62, respectively). Of the six SNP pairs, ITIH4 SNPs rs3821831 and rs2239547 were in strong linkage disequilibrium (D′ = 1.00, r2 = 0.04), and one haplotype block was identified in this region (Table 2).
Compared with a reference group of women with the TT genotype of ITIH4 SNP rs2239547, those with the CC genotype had a significantly reduced risk of depressive symptoms during pregnancy, while no significant relationship was found between the TC genotype and depressive symptoms during pregnancy (Table 3). Adjustment for the confounders under study did not appreciably change the results: the adjusted OR for the CC genotype was 0.57 (95% CI 0.36–0.91). After inclusion of the gene in the multivariable adjusted model, the value of the pseudo R2 changed from 0.0370 to 0.0415. ITIH3 SNPs rs2535629 and rs736408 and ITIH4 SNP rs3821831 were not related to depressive symptoms during pregnancy. Adjusted OR for ITIH3 SNP rs2535629 under the additive model was 0.86 (95% CI 0.71–1.04, P = 0.13): the statistical power calculation revealed that, using our sample size, we could detect the gene-disease association for an OR of 0.763 with an accuracy of more than 80% at a significance level of 0.05 with a two-sided alternative hypothesis under the log-additive model.
When haplotypes with a frequency of less than 1% in either case or control subjects were deleted, six haplotypes remained (Table 4). The haplotype carrying the rs2535629 G allele, the rs736408 C allele, the rs3821831 C allele, and the rs2239547 T allele was significantly positively associated with depressive symptoms during pregnancy, as compared with all other haplotypes combined. The other haplotypes were not associated with depressive symptoms during pregnancy.
Compared with having no children, the presence of one or more children was independently inversely associated with the prevalence of depressive symptoms during pregnancy: the adjusted OR was 0.55 (95% CI 0.41–0.75). An independent inverse relationship was found between the presence of one or more children and depressive symptoms during pregnancy in women with at least one T allele of ITIH4 SNP rs2239547, while a non-significant positive association was observed between the presence of one or more children and depressive symptoms during pregnancy in women with the CC genotype: the multiplicative interaction between SNP rs2239547 and the presence of children was significant (P for interaction = 0.01) (Table 5). No significant multiplicative interaction was shown between SNP rs2239547 and the other confounding factors under study affecting depressive symptoms during pregnancy.
Discussion
To our knowledge, the current study is the first to find that, compared with the TT genotype of ITIH4 SNP rs2239547, the CC genotype, occurring in 14.6% of control subjects, is significantly inversely related to depressive symptoms during pregnancy, while the TC genotype is not associated with depressive symptoms during pregnancy. This SNP contributes to 0.45% of the total variability of the phenotypes studied. There were no relationships between ITIH3 SNPs rs2535629 and rs736408 and ITIH4 SNP rs3821831 and depressive symptoms during pregnancy. Haplotype analyses revealed a significant positive relationship between the GCCT haplotype of rs2535629, rs736408, rs3821831, and rs2239547, occurring in 44.1% of control subjects, and depressive symptoms during pregnancy.
A case–control study conducted in Japan (868 cases and 1193 controls) showed that ITIH3 SNP rs2535629 was not significantly associated with major depressive disorder (Sasayama et al. 2014). In a case–control study performed in the Han Chinese population (1045 cases and 1235 controls), no significant relationship was observed between ITIH3 SNP rs2535629 and major depressive disorder, while ITIH4 SNP rs3821831 and SNP rs1042779, which can be used as a proxy of SNP rs736408, were significantly associated with major depressive disorder (He et al. 2014). A study conducted in Norway in a sample of 1009 patients with bipolar disorder, schizophrenia, and related psychosis spectrum disorders, ITIH4 SNP rs2239547 was significantly associated with a history of suicide attempt (Finseth et al. 2014). These results are in partial agreement with our findings.
There is no immediate explanation of the underlying mechanisms for the significant relationship between ITIH4 SNP rs2239547 and depressive symptoms during pregnancy. A study conducted in China based on a proteomic approach showed that ITIH4 levels in serum samples from 22 depressed patients were higher than those from 20 healthy controls (Wang et al. 2016). In another proteomic analysis conducted in Korea, ITIH4 levels were increased in the serum obtained before antidepressant treatment compared with the serum levels after antidepressant treatment among five patients with major depressive disorder; moreover, serum ITIH4 levels in eight patients with major depressive disorder were higher than those in eight normal controls (Lee et al. 2015). Given a relationship between ITIH4 SNP rs2239547 and serum ITIH4 levels, rs2239547 might influence the susceptibility to depressive symptoms during pregnancy. A previously cited Japanese study also showed that the number of G alleles of SNP rs2535629 was positively correlated with the gene expression levels of GLT8D1, which is located within 100 kb of rs2535629, in whole blood and that the gene expression levels of GLT8D1 were significantly higher in patients with major depressive disorder than those in controls and were positively correlated with the severity of depression (Sasayama et al. 2014). These findings might partially explain our findings regarding the positive association between the GCCT haplotype of rs2535629, rs736408, rs3821831, and rs2239547 and depressive symptoms during pregnancy.
To our knowledge, the present study is the first to assess gene–environment interactions in relation to ITIH4 SNPs and depressive symptoms; we found a multiplicative interaction between ITIH4 SNP rs2239547 and the presence of children with regard to depressive symptoms during pregnancy.
The present study had methodological advantages in that the outcome was restricted to depressive symptoms during pregnancy and in that several confounders were controlled for.
Several weaknesses of the present study have to be considered. At baseline, the participation rate could not be estimated because we do not have exact figures for the number of pregnant women who were provided with a set of leaflets explaining the KOMCHS, an application form, and a self-addressed and stamped return envelope by the 423 collaborating obstetric hospitals. In the KOMCHS, 978 pregnant women who lived in Fukuoka Prefecture completed the baseline survey between April 2007 and March 2008. On the other hand, according to the government of Fukuoka Prefecture, the number of childbirths was 46,393 in 2007 and 46,695 in 2008. The participation rate must have been low, and the study participants were probably not representative of perinatal Japanese women in the general population. For example, the distribution of educational status among participants differed considerably from that among the general population. According to the 2000 population census of Japan, the proportions of women aged 30 to 34 years in Fukuoka Prefecture with years of education of < 13, 13–14, ≥ 15, and unknown were 52.0, 31.5, 11.8, and 4.8%, respectively (Statistics Bureau, Ministry of Public Management, Home Affairs, Posts and Telecommunications, 2002). The corresponding figures for the present study in the control group were 21.8, 33.3, 45.0, and 0.0%, respectively. Nevertheless, the distribution of all four SNPs under investigation in the control group was consistent with the Hardy–Weinberg equilibrium.
Cases were identified according to the CES-D scale rather than structured diagnostic interviews. Our study subjects completed the baseline survey anywhere between the 5th and 39th week of pregnancy. The possible non-differential outcome misclassification would have led to an underestimation of values in our results.
The present study size, especially the number of cases, was rather small for a valid genetic association study; however, significant associations between SNP and haplotype and depressive symptoms during pregnancy were detected. The lack of association between ITIH3 SNP rs2535629 and depressive symptoms during pregnancy might be attributable to insufficient statistical power. Although adjustment was made for some confounders, residual confounding effects could not be ruled out. Correction for multiple testing, an appropriate element in initial exploratory analyses, was not performed in the present study. As this is a hypothesis testing study, we believe that correction for multiple testing would cause us to underestimate our results.
The present study found that the CC genotype of ITIH4 SNP rs2239547 was significantly associated with a reduced risk of depressive symptoms during pregnancy, while the haplotype containing the rs2535629 G allele, the rs736408 C allele, the rs3821831 C allele, and the rs2239547 T allele was significantly related to an increased risk of depressive symptoms during pregnancy; however, the theoretical mechanism that can explain such genetic influence is unknown. Furthermore, a significant interaction was observed between SNP rs2239547 and the presence of children that affects the risk of depressive symptoms during pregnancy. Larger case–control studies and functional studies are needed to confirm the causal relationship between ITIH4 SNP rs2239547 and depressive symptoms during pregnancy. Research regarding interactions between ITIH4 SNP rs2239547 and environmental factors is also required.
References
Barrett JC, Fry B, Maller J, Daly MJ (2005) Haploview: analysis and visualization of LD and haplotype maps. Bioinformatics 21:263–265
Bost F, Diarra-Mehrpour M, Martin JP (1998) Inter-alpha-trypsin inhibitor proteoglycan family—a group of proteins binding and stabilizing the extracellular matrix. Eur J Biochem 252:339–346
Cross-Disorder Group of the Psychiatric Genomics Consortium (2013) Identification of risk loci with shared effects on five major psychiatric disorders: a genome-wide analysis. Lancet 381:1371–1379
Finseth PI, Sønderby IE, Djurovic S, Agartz I, Malt UF, Melle I, Morken G, Andreassen OA, Vaaler AE, Tesli M (2014) Association analysis between suicidal behaviour and candidate genes of bipolar disorder and schizophrenia. J Affect Disord 163:110–114
Gauderman WJ (2002) Sample size requirements for matched case–control studies of gene–environment interaction. Stat Med 21:35–50
He K, Wang Q, Chen J, Li T, Li Z, Li W, Wen Z, Qiang Y, Wang M, Shen J, Song Z, Ji J, Feng G, Qi S, Lin H, Shi Y, Cheng Z (2014) ITIH family genes confer risk to schizophrenia and major depressive disorder in the Han Chinese population. Prog Neuropsychopharmacol Biol Psychiatry 51:34–38
Kashyap RS, Nayak AR, Deshpande PS, Kabra D, Purohit HJ, Taori GM, Daginawala HF (2009) Inter-alpha-trypsin inhibitor heavy chain 4 is a novel marker of acute ischemic stroke. Clin Chim Acta 402:160–163
Kawasaki Y, Miyake Y, Tanaka K, Furukawa S, Arakawa M (2017) Smoking and secondhand smoke exposure and prevalence of depressive symptoms during pregnancy in Japan: baseline data from the Kyushu Okinawa Maternal and Child Health Study. Tob Induc Dis 15:34
Keller MC (2014) Gene × environment interaction studies have not properly controlled for potential confounders: the problem and the (simple) solution. Biol Psychiatry 75:18–24
Lee J, Joo EJ, Lim HJ, Park JM, Lee KY, Park A, Seok A, Lee H, Kang HG (2015) Proteomic analysis of serum from patients with major depressive disorder to compare their depressive and remission statuses. Psychiatry Investig 12:249–259
Ministry of Public Management Telecommunications (2002) 2000 Population Census of Japan, Vol. 3–2–40, Labour Force Status of Population, Industry (Major Groups) of Employed Persons, and Education, Fukuoka-ken. Statistics Bureau, Ministry of Public Management, Home Affairs, Posts and Telecommunications, Tokyo
Miyake Y, Tanaka K, Okubo H, Sasaki S, Arakawa M (2013) Fish and fat intake and prevalence of depressive symptoms during pregnancy in Japan: baseline data from the Kyushu Okinawa Maternal and Child Health Study. J Psychiatr Res 47:572–578
Psychiatric GWAS, Consortium Bipolar Disorder Working Group (2011) Large-scale genome-wide association analysis of bipolar disorder identifies a new susceptibility locus near ODZ4. Nat Genet 43:977–983
Radloff LS (1977) The CES-D scale: a self-report depression scale for research in the general population. Appl Psychol Meas 1:385–401
Salier JP, Rouet P, Raguenez G, Daveau M (1996) The inter-alpha-inhibitor family: from structure to regulation. Biochem J 315:1–9
Sasayama D, Hori H, Yamamoto N, Nakamura S, Teraishi T, Tatsumi M, Hattori K, Ota M, Higuchi T, Kunugi H (2014) ITIH3 polymorphism may confer susceptibility to psychiatric disorders by altering the expression levels of GLT8D1. J Psychiatr Res 50:79–83
Schizophrenia Psychiatric Genome-Wide Association Study (GWAS) Consortium (2011) Genome-wide association study identifies five new schizophrenia loci. Nat Genet 43:969–976
Shima S, Shikano T, Kitamura T, Asai M (1985) New self-rated scale for depression (in Japanese). Jpn J Clin Psychiatry 27:717–723
Wang Q, Su X, Jiang X, Dong X, Fan Y, Zhang J, Yu C, Gao W, Shi S, Jiang J, Jiang W, Wei T (2016) iTRAQ technology-based identification of human peripheral serum proteins associated with depression. Neuroscience 330:291–325
Yang MH, Yang YH, Lu CY, Jong SB, Chen LJ, Lin YF, Wu SJ, Chu PY, Chung TW, Tyan YC (2012) Activity-dependent neuroprotector homeobox protein: a candidate protein identified in serum as diagnostic biomarker for Alzheimer’s disease. J Proteom 75:3617–3629
Acknowledgements
This study was supported by JSPS KAKENHI Grant numbers 19590606JP, 20791654JP, 21590673JP, 22592355JP, 22119507JP, 24390158JP, 25463275JP, 25670305JP, 17K12011JP, and 17H04135JP and by Health and Labour Sciences Research Grants for Research on Allergic Disease and Immunology and Health Research on Children, Youth and Families from the Ministry of Health, Labour and Welfare, Japan. The authors would like to thank the Kyushu Branch of the Japan Allergy Foundation, the Fukuoka Association of Obstetricians and Gynecologists, the Okinawa Association of Obstetricians and Gynecologists, the Miyazaki Association of Obstetricians and Gynecologists, the Oita Association of Obstetricians and Gynecologists, the Kumamoto Association of Obstetricians and Gynecologists, the Nagasaki Association of Obstetricians and Gynecologists, the Kagoshima Association of Obstetricians and Gynecologists, the Saga Association of Obstetricians and Gynecologists, the Fukuoka Society of Obstetrics and Gynecology, the Okinawa Society of Obstetrics and Gynecology, the Fukuoka City Government, and the Fukuoka City Medical Association for their valuable support.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None of the authors reported conflicts of interest.
Rights and permissions
About this article

Cite this article
Miyake, Y., Tanaka, K. & Arakawa, M. ITIH3 and ITIH4 polymorphisms and depressive symptoms during pregnancy in Japan: the Kyushu Okinawa Maternal and Child Health Study. J Neural Transm 125, 1503–1509 (2018). https://doi.org/10.1007/s00702-018-1905-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00702-018-1905-1