
Abstract
The use of robotics in neurosurgery and, particularly, in stereotactic neurosurgery, is becoming more and more adopted because of the great advantages that it offers. Robotic manipulators easily allow to achieve great precision, reliability, and rapidity in the positioning of surgical instruments or devices in the brain. The aim of this work was to experimentally verify a fully automatic “no hands” surgical procedure. The integration of neuroimaging to data for planning the surgery, followed by application of new specific surgical tools, permitted the realization of a fully automated robotic implantation of leads in brain targets. An anthropomorphic commercial manipulator was utilized. In a preliminary phase, a software to plan surgery was developed, and the surgical tools were tested first during a simulation and then on a skull mock-up. In such a way, several tools were developed and tested, and the basis for an innovative surgical procedure arose. The final experimentation was carried out on anesthetized “large white” pigs. The determination of stereotactic parameters for the correct planning to reach the intended target was performed with the same technique currently employed in human stereotactic neurosurgery, and the robotic system revealed to be reliable and precise in reaching the target. The results of this work strengthen the possibility that a neurosurgeon may be substituted by a machine, and may represent the beginning of a new approach in the current clinical practice. Moreover, this possibility may have a great impact not only on stereotactic functional procedures but also on the entire domain of neurosurgery.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Stereotactic procedures in neurosurgery began more than 90 years ago when the pioneers of Stereotaxis (Gildemberg and Tasker 1996) made the first stereotactic apparatus to guide the surgical tools (instrumentation) to the planned targets without direct human visual control. Since the initial use of these stereotactic systems, different types of devices and tools have been used (Gildemberg and Tasker 1996; Mazzone 2001). More recently, the integration of stereotaxis with neuroimaging (CT scan and MRI) improved the surgical possibilities, allowing doctors to reach deeper targets, as in human brain-stem stimulation (Gildemberg and Tasker 1996; Mazzone et al. 2008, 2011, 2013, 2016; Mazzone and Scarnati 2009; Benabid et al. 1987a, b; Galloway and Maciunas 1990). The main fields of application of Deep Brain Stimulation (DBS) are pain syndromes, epilepsy, and, from 1987, movement disorders (Benabid et al. 1987a, b, 2005). This last application of Central Nervous System (CNS) stimulation applies to a large amount of diseases, and the use of DBS has increased the knowledge of disease mechanisms. Intraoperative recordings (Benazzouz et al. 2002; Fedele et al. 2001; Stefani et al. 2005) add a great source of information and may enhance surgical precision and advance stereotactic surgery, allowing the application in the near future of new implantable nanotechnologies, such as microarrays. With respect to classic stereotactic surgery and tools, the technical evolution of applied stimulating devices may require a different surgical approach and a wider diffusion of robotic technologies (Mazzone et al. 2008; Mazzone and Scarnati 2009; Joskowicz et al. 2006; De Lorenzo et al. 2011), especially if we consider multiple-target implantations and brain-stem procedures. The growth of neuroimaging accuracy together with neuronavigational possibilities and the development, flexibility, and speed of manipulator robots represented a revolutionary link to execute automatic surgical procedures, such as reaching a target in the brain. Moreover, the robot manipulator can perform many functions other than being a simple substitute of the frame-based or frameless stereotactic devices. In this paper, we explored the possibility for a robotic surgical performance without the participation of the surgeon’s hands by means of specific constructed actuators.
Past experiences of robotic neurosurgery
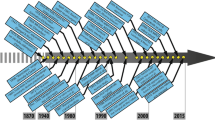
There are several examples of robotic systems adopted or specifically developed for neurosurgery (McBeth et al. 2004; Sam Eljamel 2008; Karas and Baig 2008; Sekhar et al. 2011). The use of robots in neurosurgery started in the 1980s when a PUMA 200 industrial manipulator was first used to allow a surgeon to guide a custom-made probe (Kwoh et al. 1985, 1988). Another important experiment was performed in Lausanne with the specifically developed MINERVA robot (Flury et al. 1992; Burckhardt et al. 1995). In 1987, in France, a group under Prof. Benabid started the development of the robot that is now marketed as NeuroMate® (by Renishaw plc) (Benabid et al. 1987b, 1998). Other examples include the Evolution 1 (Zimmermann et al. 2002), the MRI compatible robot (Masamune et al. 1995), the RoboSim Neurosurgery Simulator (Radstzky and Radolph 2001), and the NeuroArm (Louw et al. 2004). Other alternatives to robots for automating neurosurgery have been proposed in (Modrák et al. 2002). Commercially developed robotic systems for neurosurgery include the Pathfinder by Prosurgics, UK, the ROSA™ (MedTech, France) (Lefranc and Le Gars 2012), and the already mentioned Neuromate by Renishaw. From the use of the first robot in surgery, the Puma, to the more recent NeuroArm, more than 20 years have passed with great results. While the Puma was an industrial robot used in assembly, the NeuroArm was designed specifically for neurosurgical operations; both the performance and the production costs of the two robotic systems are not comparable. The cost of the NeuroArm project, composed of two robotic arms in titanium and the needed workstations, reaches about $30 million, against the few thousand needed for an industrial manipulator. Moreover, Puma was not yet a commercial robotic system as NeuroMate is. This last is a neuroimage-guided system able to automatically position a tool to reach a given target. However, the accuracy of the NeuroMate robotic system is not superior to that of conventional stereotactic biopsies, which is below 1 mm. The in vitro application accuracy result for NeuroMate is 1.95 ± 0.44 mm for frameless registration, but it goes down to 0.86 ± 0.32 mm in a frame-based configuration (Li et al. 2002). Moreover, although these robotic systems can perform specific well-defined tasks, there is currently no system that can perform a whole neurosurgical procedure. Considering the continuous evolution of anthropomorphic manipulators, it seems right to wonder how far a modern industrial manipulator can be used in surgery, trying to emulate the precision of the results obtained from the most sophisticated and expensive surgical robotic workstation.
The objective of this work was then to evaluate the ability, reliability, and precision of an industrial robot in reaching a given target, but also in the application of a new Skull Applied Stereotactic Frame (SASF) and in the autonomous insertion of leads for DBS in the planned target. The robots actually in use are based on a different method of spatial neuroradiological identification of targets and trajectories. They realize a static initialization of the stereotactic procedure, followed by the hand action of the surgeon. Our experience with respect to these traditional robotic approaches is based on “no hands” control of the entire surgical sequence. The implantation of surgical deep electrodes was made by the robot arm, splitting up the times of surgery and utilizing different actuators to apply miniaturized stereotactic devices. Without hand control or links between the surgeon and the robot arm, we realized both the general phases of surgery, which were skin incision, haemostasis control, and the drilling of skull holes, followed by robotic application to the skull of different stereotactic tools and guides, and the final phase of lead introduction. The main target of this approach was the automatic control of all steps of the surgical procedure: the link with the surgeon is only the system user interface. The second one, obviously, was to verify the precision and safety of this robotic surgical procedure, with respect to the actual traditional robotics standards.
The present paper is divided into four main parts. “Introduction” deals with some background experience developed by the construction of an innovative stereotactic device and the consequent design and building of new tools. “Method and tools” describes the new robotized procedure with the initial validation of the robotic capabilities, the laboratory trials, and, then, the in vivo surgery. Finally, “From classical to robotized procedure” shows the results, and a section of discussion and conclusions closes the paper.
Method and tools
Stereotactic devices
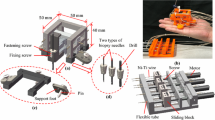
In 1997, a stereotactic device called 3P Maranello was built in cooperation with an Italian company (CLS Titanium, Forli’, Italy) (Mazzone 2001). The 3P Maranello has a double autocarrying emiarch with the ability to check two or more final targets simultaneously and with different independent tracks, able to target different structures during the advancing of probes to the final destination. As shown in Fig. 1a, the device permits fixing the target position by translations along the three axes and the approach direction by the two rotations: emiarch angle (green row in Fig. 1a) and cursor angle (red row in Fig. 1a). This device was constructed to have the possibility of multiple simultaneous recordings, as neurochemical (microdyalisis) or electrophysiological, from several anatomical sites and may allow the insertion into the brain of two or more permanent leads. The system was further developed in 2003 using a robotic advancing system with infrared remote control and five different independent parallel tracks, with steps of advancing from 1 µ to 1 mm (Fig. 1b) (Mazzone et al. 2011; Benabid et al. 1987a, b). In 2006, a new “low profile and size” SASF was made, which permitted the abolition of the emiarchs, but maintained the skills of the previous system. The first applications of SASF are realized by the classic emiarch system. This is able, by means of the frame-based approach, to make the same holistic conceptions of a “classic” stereotactic frame (Fig. 1c). The operative robotized version was conceived to avoid the need to apply this device through the emiarch, as it was done before. The patient may undergo the surgical procedure with only this small frame and, consequently, with a great sensation of freedom. Recordings are also revolutionized, giving the possibility to make them in a standing position or during the gait. The comparison between classic arch implantation and SASF has shown comparable targeting precision and clinical results.

a Maranello Stereotactic Apparatus, in 1998. b Robotic Advancing System arch mounted, from 2003. c Skull applied stereotactic frame (SASF). d Mechanical microdrive
New robotic tools actuators
To apply on the skull the devices described above, CLS Titanium (Forli, Italy) builts specific, newly designed robotic actuators to facilitate robotic actions. The instrumentation is realized in titanium, non-magnetic steel, and ergal. The connections within the robotic flange are studied to facilitate the change of instruments between the different phases of the surgical procedure. SASF is a small disc of 12 mm of diameter. As shown in Fig. 1c, there are six holes of 1.9-mm diameter in the surface and a central one with the same diameter, to submit several instruments through parallel tracks. The inferior surface presents a central screw (5-mm diameter and 5-mm height) to fix this frame to the skull. The central hole crosses this screw represents the planned direction to the target, and contains the system of the automatic setting of the electrode. The multiple tracks are required to realize spatial neurophysiological definitions of target boundaries. The advancement of the stylet can be done using a mechanical microdrive (Fig. 1d) or robotic miniaturized one (Fig. 1b). The system, even if applied to the skull only with the central screw, is very firm; the other cannulas add a great stability to the system. The frame must be applied to a horizontal skull surface to realize an optimal alignment to increase the accuracy of the planned trajectories. A specific tool actuated by an electric drill was built to horizontally smooth the skull curved surface. Tool carrier to Apply Frame on the skull (TAF) is a double concentric cylindrical system, able to slide over, with a spring inside to impose a given axial force on the SASF. It allows the fixing of the SASF screw in the skull using the robot and a mechanical drill without adopting a force sensor (Fig. 1d). This tool also allows easy detachment when the frame screw is completely fixed.
From classical to robotized procedure
From the expertise gained in more than 650 stereotactic procedures (of which 450 were for DBS to treat movement disorders), it was clear that manual stereotactic surgery has several drawbacks, especially, because it requires a long time for each step. Moreover, the precision of this method is strongly related with the manual capability and experience of the surgeon. The probability of making errors is also high, since the stereotactic head is manually controlled. The available robotic systems for neurosurgery, previously described in the introduction, partially solve these problems. In fact, in most cases, these also require the manual intervention of the surgeon, giving only guidance for the tool. The main goals of our research were then to improve the precision in the positioning of the tools, to greatly increase the speed of the operations, to allow accurate planning and monitoring of the sequence of the different steps, and to fully automate the neurosurgical procedure. The final aim is then an automatic “no hands” surgical procedure, with the purpose to implant leads into the brain. From a philosophical point of view, with this procedure, the surgeon’s skills are transferred from manual dexterity to planning capabilities.
Experimental procedure
The experimental procedure was performed along the time into three fundamental phases:
-
Validation of the robotic capabilities.
-
Laboratory simulation of the surgical procedure.
-
In vivo experimentations.
The following subsections describe these three steps in detail.
Validation of the robotic capabilities
In this phase, the validation of the robotic capability and reliability to reach a target inside a phantom in a very simple stereotactic surgical condition (Fig. 2) was performed.

Simulation of the robotic surgical procedure in comparison with the classical stereotactic device
Evaluation of robot/patient configuration
The purpose of this activity was to individuate the robot-patient positioning to guarantee higher manipulation capability and accuracy. In particular, the optimization was performed among the different configurations that a manipulator can assume to reach a given target.
Various working simulation layouts have been created to evaluate the several aspects of the problem. To allow stronger feedback from the surgeon, the robot positioning was virtually superimposed on a classical stereotactic head, as can be seen in Fig. 2. In this way, it was easier to understand how the manipulator was acting to replace the classical procedure.
The study concerned the following points:
-
evaluation of positioning error according to the angles of approach to the target;
-
evaluation of positioning error according to the length of the lead;
-
evaluation of positioning error according to the target position;
-
manipulability analysis.
Software simulations have been carried out, considering some configurations of the lead assembly on the robot.
The manipulability analysis has been carried out using the scalar index, defined by Yoshikawa (1995), that gives an indication of how far the robot is from singularities and thus able to move and exert forces uniformly in all directions. It can be expressed by the following equation:
where J is the Jacobian matrix in world coordinates.
Figure 3 reports some of the results obtained. In particular, as shown in Fig. 3a and b, the manipulability index has been evaluated during the insertion of the lead, i.e., along a straight path, varying the approach angles along the Coronal plane (cursor angle fixed to 0) and the Sagittal plane (emiarch angle fixed to 0), respectively.

Manipulability index relating the configuration along a straight path varying the approach angles along the Coronal plane (a) and the Sagittal plane (b)
Evaluation of positioning accuracy
Since the kinematic model cannot consider the mechanical and assembling tolerances, further investigation on positioning accuracy has been carried out on the real robot used in the experimentation.
The precise positioning of the end effector of a robot should be an important parameter to characterize its performance. However, in the technical specifications of commercial industrial robots, it is very rare to find information that indicates their absolute precision. As a partial justification of the manufacturers, it must be considered that the traditional applications of robotics are based essentially on the repeatability of the movements. In fact, the robots are mostly required to perform repetitive tasks on the paths defined in the joint space by sequences of points, planned in advance by the operator. For this reason, the manufacturers’ specifications usually indicate the repeatability of positioning of the end effector, or the center of the flange that holds the tool. The robot used for our experimentation has a repeatability of 0.03 mm, as shown in Table 1. With a reach of 850 mm, this compact, space-saving 6-axis robot combines high speed and accuracy with a long range. The intrinsic characteristics of the robot make it suitable to perform delicate operations, such as neurosurgery, resulting in the need for a thorough study to exploit the potential of the precision of the system. The main limitation to overcome is the intrinsic positioning accuracy that characterizes all industrial robots. As a consequence, a calibration process is fundamental to the procedure to adjust the kinematics model parameters and improve the robot’s precision. The objective of this analysis was then the characterization of the positioning error of the robot. In particular, the proposed experimental procedure permits the elaboration of the position of the robot using a method based on the Camera Calibration Toolbox for MATLAB (Bouguet 2006). As shown in Fig. 4, a high-resolution camera watching the grid below has been mounted on the robot’s wrist. The extrinsic parameter calculated from the grid images during the robot movement permits an estimation of the relative movement of the robot. Figure 5 shows the angle error during the programmed movement of the robot reported in Fig. 4. In particular, several consecutive five-degree step rotations have been performed varying the Emiarch and Cursor angles with respect to a fixed point on the grid below. The rotations concern the Sagittal and Coronal planes, respectively. The results show that the error is always below 0.1°, at least for the range concerning the stereotactic surgery. Finally, considering the results of this phase, it has been possible to define and optimize the plant setup in terms of robot-patient positioning, as shown in Fig. 6.

Experimental setup for the characterization of the positioning error of the robot: rotation performed from the robot along the Coronal (a) and Sagittal (b) planes

Error on the Cursor (a) and Emiarch (b) angles

Plant overview: from simulation to experimental setup
In vivo animal experimentation
The animal experimentation was performed first on five heads of dead pigs and in the next phase on five anesthetized head of live large white pigs. The experiments were done in the Biothecnological Center—AORN Cardarelli, Naples, Italy, with the permission and approval of the local ethical committee. The animal experimentation was conducted on Large White Pigs, intubed and anesthetized, with the application of three carbon pins fixed in the occipital and, bilaterally, in the malar region, of a former Leksell frame modified for stereotactic surgery in the pigs (Leksel 1950). As shown in Fig. 7, a Plexiglas box was positioned on the frame allowing two fundamental functions:

a, b Handmade Plexiglas coordinates box for Leksell frame planning. c The animal experimental conditions
-
Base coordinate system calibration procedure.
-
Frame coordinate determination by CT scan.
The base coordinate system is used as the reference system to define the position of the animal head. During this phase, which requires a few minutes, a Cartesian coordinate system is assigned using the base calibration procedure of the robot, which also returns a quality index of the procedure. Then, a translation is applied on the resulting coordinate system to set it to the center of the Leksell frame. Consequently, when interpolating the motion path, the robot controller calculates under normal circumstances (tool mounted on the robot flange) the current position in relation to the animal head coordinate system. The Plexiglas coordinates box was also useful to make coordinate determinations by MRI and Angio-CT scan and/or Ventriculography without artefacts. Trajectory planning was carried out primarily considering safety and targeting precision issues for the surgery (Joshi et al. 2008). In more detail, a software tool (“Medico CAD”—Maranello Stereotactic System, CLS Titanium, Forlì, Italy) was used to virtually include, within the frame, all the sensible structures that have to be accurately avoided from colliding with the electrode trajectory (Mazzone 2001; Mazzone and Scarnati 2009; Mazzone et al. 2008, 2011, 2013, 2016). This is the case, for example, of the brain blood vessels, which are the major cause of failure in this kind of surgical operation. Blood-vessel reconstruction is obtained from the Angio-CT scan images under the form of point clouds organized in slices. These clouds are automatically transformed, using a virtual prototyping methodology, in virtual surfaces and virtual objects in a 3D environment. Additional tolerances are also considered for safety reasons and to compensate for possible rendering errors. These are subsequently virtually included within the skull area surrounded by the stereotactic frame and aligned with the reference frame, the same one used for the stereotactic targeting. More details are reported in (Mazzone et al. 2008; Mazzone and Scarnati 2009). This virtual system was already experimentally used in human patient operations, to select the safest one among different planning possibilities and to help avoid a number of very dangerous situations. In our robotic implementation, the 3D overall view constitutes the operative area for the robot where, besides the target point, these forbidden areas are duly reported for a safety trajectory planning procedure. An X-ray intraoperative control was made to check the progression of the lead into the pig brain. In all cases, the MRI and CT scan are performed before and after the surgical procedure. After the control of stereotactic space inside the frame, the neuroimaging and planning data are processed to assist the surgeon in the exact computation of target coordinates and the trajectories of leads.
Once the surgeon makes the cut and places the retractor (Fig. 8a), the next phases of the surgical operation are all executed by the robot.

Experimental surgical procedure
The experimental surgical procedure consists of the following main robotic operations:
-
Realization of former hole (1.8 mm) (Fig. 8b).
-
Make a 5-mm hole for SASF and horizontalization of the skull (Fig. 8c).
-
Application by TAF of a miniaturized stereotactic frame (SASF) (Fig. 8d).
-
Insertion of the rigid stylet into the central track of the SASF (Fig. 8e).
-
Insertion of the electrode (Fig. 8f).
Once these operations are executed, the surgeon again takes control, verifies the setting of the electrode to the skull, and sutures the skin.
The drill (type electrical Midas Rex Medtronic Minneapolis, USA) was applied to the robotic wrist and used together with specific tools and synchronized with the robotic movements (Fig. 8a through d). The change of tools is not automatic, but in the next phases of experimentation and in human applications. The adoption of an automatic tool-changing system is planned.
Results
Reliability of the procedure and safety of employed tools
The neuroradiological examinations did not reveal brain damage related to the surgical procedure; no hemorrhagic event or brain edema or other abnormalities were found in post-operative controls (MR or CT scan) into the brain of the pigs. In the two cases, the brains of the pigs were carefully removed after the procedure and sectioned along frontal sections of 5 mm; the macroscopic examination did not reveal any evident damage into cerebral tissue or hemorrhagic complication in the site of targeting or along the trajectories.
Time of surgical procedures
The central (skin to skin) times of surgical procedures were monitored and compared with our experience in standard unilateral human surgeries (Mazzone et al. 2011, 2013, 2016). The mean values are consistently reduced on average from 75 ± 16.5 min in the classic human surgery (taken from the last five human unilateral procedures) to 38 ± 12.8 min, for a single lead implantation in robotic procedure. The planning phases are not considered for quantifying the temporal data.
Validation of precision and reliability of the procedure
The experimental results related to errors of positioning of the leads with respect to the planned coordinates, both in the five isolated pig heads and the five “in vivo” animals, are shown in Table 2a, b. In all sessions with the conventional neuroimaging controls (CT scan, MRI, Rx), the fully automated procedure demonstrated a low positioning error rate (0.1 cm ± 0.014). Some differences between isolated heads and “in vivo” were found, due to different experimental settings and, above all, to different biological conditions. In particular, the “in vivo” fifth trial showed a higher error in reaching a target positioned at the coordinates [X = 0.990 cm, Y = 0.790 cm, Z = 0.000 cm], where the two Emiarch and Cursor approach angles were 18° and −8°, respectively (Fig. 9).

Selected image of the post-operative CT scan in which the tip of electrode has been highlighted (a) and verification of target in coronal and sagittal projection of CT scan (a, b) regarding the fifth trial. Colours legend in c—Trial 5 in red the error expressed in cm in Cartesian coordinates between the planned target (green) and the really reached point (blue)
Discussion
The results of our experimental trial represent a significant step towards the possibility of a radical change, in rational basis, of the application of robotics in stereotactic neurosurgery. The conceptual aim of our experience was to realize a “fully” automated robotic procedure, utilizing new mechanical tools applied automatically by the robotic arm, without any loss of precision or increase of risk in the insertion of the leads into the brain, with respect to classical surgery. Moreover, in this paper, the target should be considered only as a landing point, to compare the planned and the experimentally executed coordinates. This study did not consider any analysis on the action of DBS or on the efficacy, from a therapeutic point of view, for a specific brain target; but was performed to introduce a new approach in robotic neurosurgery, i.e., towards a fully automated robotic procedure. Nevertheless, this approach, showing comparable errors with respect to classic or with manually assisted robotic methods, represents an undoubted progress. The time duration of the surgical procedure is consistently reduced with respect to a manual approach. Moreover, due to the miniaturization of the devices that renders unnecessary the cumbersome and heavy traditional stereotactic systems, the comfort for the patients in a future human application may be increased. On the other hand, this approach is in line with the development of the more recent frameless neurosurgery. It is also conceivable that neurosurgical procedures will be simplified and the amount of the staff personnel will be greatly reduced. Furthermore, fewer people with high knowledge on the standards and skills on the procedures are required, thus allowing greater spread of therapy. The first little hole (1.8 mm) in stereotactic position (Fig. 8a) is the former step of the robotic procedure. The pilot of the next screw is fundamental to maintain the exact stereotactic positioning and to avoid problems in the SASF installation. To get a robotic stable fixation of the frame without any significant displacement of this tool, the diameter of holes performed must be progressively increased (Fig. 8b). As shown in the pictures, the stereotactic alignment was excellent in all the experiments, and the SASF did not exhibit any problems in its application to the skull. Before the application of the SASF, the horizontalization of the theca was performed by an end mill in relation to the possible variations of the trajectory from time to time programmed (Fig. 8c). This phase is planned to assure a correct and solid stereotactic positioning of the SASF (hardly reachable with the right accuracy on a curved theca) (Fig. 8d). In the initial stages of the trial (on the heads of dead pigs), two different issues due to the “elasticity” of the leads (model 3389 Medtronic, USA) were studied and solved: wrong positioning of leads with respect to the target and impossibility of easily inserting the lead into the SASF. The first issue was solved by preceding the descent of the lead from a rigid stylet of the same diameter that traces a way devoid of tissular resistance (Fig. 8e). The application of a rigid stylet was easy, and no reduction of precision was obtained in reaching the planned target with it. In this way, a coaxial carrier cannula causing a larger diameter of the track, potentially harmful for the brain parenchyma, can be avoided. It should be observed that the lead employed in the experimentation (Medtronic 3389, Neurological Division, Minneapolis USA) is a typical lead for human applications and probably is not ideal, due to its length, diameter, and flexibility, for the animal experimental robotic surgery. This second issue was solved by equipping the robotic hand of two cylinders to lock the lead with a double function: it was long enough to limit deflection of the head of the lead and was grooved to avoid slipping during the descent of the lead. The lead has a high elasticity, which causes some oscillations. This problem was overcome by reducing the free part of the lead out of the robotic hand and setting back the electrode body, thus avoiding its retreat. Moreover, the material of the lead coating demonstrates a very high resistance to progression into the brain tissue, which is a viscoelastic system, and during the crossing of the dural surface. This is due to the friction that its silicone coating could generate during the advancement of the lead (Fig. 8f). The planning of this phase requires great attention, in particular for the choice of the insertion velocity of the electrode. The differences in the time durations of surgery with respect to the human ones are consistent with the fully automated procedure. We have considered even the differences in body size between the two situations. However, we must also consider the problems encountered in the experimental set. A clear difference was found in the isolated heads with respect to the “in vivo” experimental conditions: in the former, the progression of the leads was easier due to the lower viscosity of the different tissues and to the absence of vessels pulsatility. Moreover, these last two factors also explain the difference in the coordinates value errors of lead positioning (Table 2a, b). Special attention was dedicated to the automatic anchoring system to prevent dislocation of the lead from the target at the time of removal of the robotic arm. The fastening system operates automatically and simultaneously with the removal of the SASF, without further action of the robotic arm. Finally, the experiments on “in vivo” animals were conducted without any specific feedback from a specific sensor system to control the progression, exactness, and safety in the different steps of procedure. In addition, the automatic change of tools was not utilized; the different tools were changed by physicians at the beginning of each new operative step. However, in the human application, we plan to develop further sensing and control systems and the automatic change of the tools.
Conclusion
This paper presented an experimental robotic stereotactic procedure “no hands” aimed to realize a lead implantation into a brain target. The experience progressed from some preliminary laboratory trials and then to five “in vivo” anesthetized pigs. The laboratory and experimental animal surgery reached all planned targets, demonstrating that it was possible to avoid the intervention of the surgeon’s hands, and a complete fully automated surgical robotic procedure was made. The obtained results showed good precision in positioning the electrode, and the time required was strongly reduced with respect to a common manual or the traditional robotic procedure, according to data in the literature (Bekelis et al. 2012; Lollis and Roberts 2008). The developed robotic system introduces several innovative points with respect to the actual neurosurgery. The realization of a fully automated robotic procedure requires, in addition to the spatial and temporal decomposition of the surgical sequences, specific actuators, and suitably constructed for each surgical sequence: the hardware parts mentioned above, could be in the future automatically changed and supported by a suitable control system in the implementation of their tasks. In this way, potentially difficulties, traditionally solved by the surgeon, if unexpected biological or technological events occur, could be automatically solved. Moreover, it must be considered that the robot adopted in this animal experimental procedure was an industrial one, not certified for surgical operations in humans. The next step will be the adoption of a robotic certified manipulator and the development of a full “no hands” procedure in humans. Nowadays, transferring surgical actions from man to machine is still a painful experience for the surgeons and, in addition, the process requires an expansion of skills and knowledge towards other scientific fields, apparently far from the current medical science. This is perfectly in accordance with the famous statement of Harvey Cushing who, more than a century ago, predicted:
“I would like to see the day, when somebody would be appointed surgeon somewhere who had no hands, for the operative part is the least part of the work………” American surgeon, Letter to Henry Christian (November 20, 1911)
References
Bekelis K, Radwan TA, Desai A, Roberts DW (2012) Frameless robotically targeted stereotactic brain biopsy: feasibility, diagnostic yield, and safety. J Neurosurg 116(5):1002–1006
Benabid AL, Pollak P, Louveau A, Henry S, de Rougemont J (1987a) Combined (thalamotomy and stimulation) stereotactic surgery of the VIM thalamic nucleus for bilateral Parkinson disease. Appl. Neurophysiol 50:334–346
Benabid AL, Cinquin P, Lavalle S, Le Bas JF, Demongeot J, de Rougemont J (1987b) Computer-driven robot for stereotactic surgery connected to CT scan and magnetic resonance imaging: technological design and preliminary results. Appl Neurophysiol 50:153–154
Benabid AL, Hoffmann D, Ashraf A, Koadse A, Esteve F, La Bas JK (1998) Robotics in neurosurgery; current status and future aspects. Chirurgie 123:25–31
Benabid AL, Wallace B, Mitrofanis J, Xia R, Piallat B, Chabardes S, Berger F (2005) A putative generalized model of the effects and mechanism of action of high frequency electrical stimulation of the central nervous system. Acta Neurol Belg 105:149–157
Benazzouz A, Breit S, Koudsie A, Pollak P, Krack P, Benabid AL (2002) Intraoperative microrecordings of the subthalamic nucleus in Parkinson’s disease. Mov Disord 17(Suppl 3):S145–S149
Bouguet JY (2006) Camera Calibration Toolbox for Matlab. Available: http://www.vision.caltech.edu/bouguetj/calib_doc/index.html
Burckhardt CW, Fluty P, Glauser D (1995) Stereotactic Brain Surgery Integrated MINERVA system meets demanding robotic requirements. IEEE Eng Med Biol 14(3):314–317
De Lorenzo D, De Momi E, Dyagilev I, Manganelli R, Formaglio A, Prattichizzo D, Shoham M, Ferrigno G (2011) Force feedback in a piezoelectric linear actuator for neurosurgery. Int J Med Robot Comput Assist Surg 7:268–275
Fedele E, Mazzone P, Stefani A, Bassi A, Ansaldo MA, Raiteri M, Altibrandi MG, Pierantozzi M, Giacomini P, Bernardi G, Stanzione P (2001) Microdialysis in Parkinsonian patient basal ganglia: acute apomorphine-induced clinical and electrophysiological effects not paralleled by changes in the release of neuroactive amino acids. Exp Neurol 167:356–365
Flury P, Lopez P, Glauser D, Villotte N, Burckhardt CW, (1992) MINERVA, a robot dedicated to neurosurgery operations. In: Proceedings of the 23rd ISIR, Barcelona, 6–9 Oct., pp 729–733
Galloway RL, Maciunas RJ (1990) Stereotactic neurosurgery. Crit Rev Biomed Eng 18(3):181–205
Gildemberg PL, Tasker RR (1996) Textbook of stereotactic and functional neurosurgery, Part 1, Stereotactic Principles/1, Section 1, 2, 3, pp 5–256
Joshi A, Scheinost D, Vives KP, Spencer DD, Staib LH, Papademetris X (2008) Novel interaction Techniques for neurosurgical planning and stereotactic navigation. IEEE Trans Vis Comput Graph 14(6):1587–1594
Joskowicz L, Shamir R, Freiman M, Shoham M, Zehavi E, Umansky F, Shoshan Y (2006) Image-guided system with miniature robot for precise positioning and targeting in keyhole neurosurgery. Comput Aided Surg 11(4):181–193
Karas CS, Baig MN (2008) Robotic Neurosurgery. In: Medical Robotics, edited by Vanja Bozovic, ISBN 978-3-902613-18-9, I-Tech Education and Publishing, Vienna, Austria, p 526
Kwoh YS, Reed IS, Chen JY, Shao HM, Truong TK, Jonckheere E (1985) A new computerized tomographic-aided robotic stereotaxis system. Robot Age 7(6):17–22
Kwoh YS, Hou J, Jonckheere EA, Hayati S (1988) A robot with improved absolute positioning accuracy for CT guided stereotactic brain surgery. IEEE Trans Biomed Eng 35:153–160
Lefranc M, Le Gars D (2012) Robotic implantation of deep brain stimulation leads, assisted by intra-operative, flat-panel CT. Acta Neurochir (Wien) 154(11):2069–2074
Leksel L (1950) Stereotactic apparatus for intracranial surgery. Acta Chir Scand 99:229–233
Li QH, Zamorano L, Pandya A, Perez R, Gong J, Diaz F (2002) The application accuracy of the NeuroMate robot—a quantitative comparison with frameless infrared and frame based surgical localization systems. Comput Aided Surg 7(2):90–98
Lollis SS, Roberts DW (2008) Robotic catheter ventriculostomy: feasibility, efficacy, and implications. J Neurosurg 108(2):269–274
Louw DF, Fielding T, McBeth PB, Gregoris D, Newhook P, Sutherland GR (2004) Surgical robotics: a review and neurosurgical prototype development. Neurosurgery 54:525–534
Masamune K, Kobayashi E, Masutani Y (1995) Development of an MRI compatible needle insertion manipulator for stereotactic neurosurgery. J Image Guid Surg 1:242–248
Mazzone P (2001) Il sistema stereotassico 3P Maranello. Eur Medicophys 3:318–319
Mazzone P, Scarnati E (2009) Deep brain stimulation of the medial thalamus for movement disorders: the role of centromedianparafascicular complex. In: Krames ES, Peckham PH, Rezai AR (eds) Neuromodulation. Academic Press, New York, pp 599–615
Mazzone P, Della Marca G, Sposato S, Di Lazzaro V, Scarnati E (2008) Tridimensional modelling of midbrain and pontine structures: a proposed approach to the stereotactic targeting of nucleus pedunculopontine tegmenti. Neurotarget 3:8–20
Mazzone P, Sposato S, Insola A, Scarnati E (2011) The deep brain stimulation of the peduncolopontine tegmental nucleus: towards a new stereotactic neurosurgery. J Neural Transm. 118(10):1431–1451
Mazzone P, Sposato S, Insola A, Scarnati E (2013) The clinical effects of deep brain stimulation of the pedunculopontine tegmental nucleus in movement disorders may not be related to the anatomical target, leads location, and setup of electrical stimulation. Neurosurgery 73:894–906
Mazzone P, Vilelha Filho O, Viselli F, Insola A, Sposato S, Vitale F, Scarnati E (2016) Our first decade of experience in deep brain stimulation of the brainstem: elucidating the mechanism of action of stimulation of the ventrolateral pontine tegmentum. J Neural Transm. doi:10.1007/s00702-016-1518-5
McBeth PB, Louw DF, Rizun PR, Sutherland GR (2004) Robotics in neurosurgery. Am J Surg 188(Suppl to October 2004):68S–75S
Modrák V, Paško J, Pavlenko S (2002) Alternative solution for a robotic stereotactic system. J Intell Robot Syst 35:193–202
Radstzky A, Radolph M (2001) Simulating tumor removal in neurosurgery. Int J Med Inf 64:461–472
Sam Eljamel M (2008) Robotic applications in neurosurgery. In: Medical Robotics, edited by Vanja Bozovic, ISBN 978-3-902613-18-9, I-Tech Education and Publishing, Vienna, Austria, p 526
Sekhar LN, Ramanathan D, Rosen J, Kim LJ, Friedman D, Glozman D, Moe K, Lendvay T, Hannaford B (2011) Robotics in Neurosurgery. In: Rosen J, Hannaford B, Satava RM (eds) Surgical robotics systems applications and visions. Springer, New York, USA
Stefani A, Fedele E, Galati S, Pepicelli O, Frasca S, Pierantozzi M, Peppe A, Brusa L, Orlacchio A, Hainsworth AH, Gattoni G, Stanzione P, Bernardi G, Raiteri M, Mazzone P (2005) Subthalamic stimulation activates internal pallidus: evidence from cGMP microdialysis in PD patients. Ann Neurol 57:448–452
Yoshikawa T (1995) Manipulability of robotic mechanisms. Int J Robot Res 4(2):3–9
Zimmermann M, Krishnan R, Raabe A, Seifert V (2002) Robot-assisted navigated neuroendoscopy. Neurosurgery 51:1446–1451
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflicts of interest.
Rights and permissions
About this article

Cite this article
Mazzone, P., Arena, P., Cantelli, L. et al. Experimental new automatic tools for robotic stereotactic neurosurgery: towards “no hands” procedure of leads implantation into a brain target. J Neural Transm 123, 737–750 (2016). https://doi.org/10.1007/s00702-016-1575-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00702-016-1575-9