
Abstract
Background
Watertight dural closure is a crucial step in preventing postoperative cerebrospinal fluid (CSF) leak and subsequent infection in posterior fossa surgery. The aim of this study is to assess an alternative use of collagen matrix double grafting in microvascular decompression (MVD).
Methods
Dural closure using double collagen matrix grafts was retrospectively compared with autologous fascial grafting in 120 patients who underwent MVD. Double collagen matrix grafting technique, a combination use of inlay and onlay grafting (DuraGen®, Integra Lifesciences, Plainsboro, NJ, USA, $700–800 for an MVD craniotomy size), was applied in 60 patients (the collagen matrix group). In the remaining 60 patients, an autologous fascial graft was sutured in a watertight fashion to the dural defect (the fascia group). Postoperative wound complications, such as CSF leak and infection, were retrospectively compared between the two groups.
Results
CSF leaks were observed in 3 patients (5.0%) in the fascia group and in 2 patients (3.3%) in the collagen matrix group. All cases of CSF leakage presented with pseudomeningoceles except one patient who developed an incisional CSF leak. A repair surgery for CSF leak was required in this one patient in the fascia group. Subcutaneous abscesses were noted in 2 patients (3.3%) in the fascia group. There was no patient who developed a subcutaneous abscess in the collagen matrix group. One patient in each group developed aseptic meningitis. Statistical analyses revealed that the collagen matrix group showed non-inferior outcomes to the fascia group in CSF leaks and infectious complications.
Conclusions
Double grafting technique with a combination of inlay and onlay collagen sheets is a safe and secure alternative for watertight dural closure despite a cost limitation.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The most frequent complication in posterior fossa surgery is postoperative cerebrospinal fluid (CSF) leakage presented as pseudomeningocele, incisional CSF leak, CSF rhinorrhea, subsequent subcutaneous abscess, and meningitis [9, 14,15,16, 18, 20, 23]. Some of those patients may require additional surgical interventions; therefore, watertight dural reconstruction is a crucial step in preventing CSF leaks and relevant infections [8, 17]. Microvascular decompression (MVD) can be performed through a small craniotomy. It is not always feasible to suture the dural edges in a watertight fashion in such a small craniotomy due to shrinkage of the dura mater [16, 22]. A fascial flap harvested from the suboccipital muscles is widely used as a patch graft for watertight duraplasty in MVD. Collagen matrix dural grafting has been available for more than a decade,but dural repair with single layer grafting in posterior fossa surgery has not been popularized due to cost increase and relatively high CSF leak rate [9, 12,13,14,15]. We developed a double grafting method of inlay and onlay collagen sheets for dural closure in MVD and evaluated the potential alternative use instead of the conventional method of harvesting an autologous fascial flap.
Material and method
Patient cohort
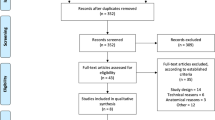
The objectives are 120 patients who underwent MVD in our institutes from June 2018 to June 2020 with more than a 6-month follow-up period (Fig. 1). Two different methods of dural reconstruction were compared. Collagen matrix grafts (DuraGen®, Integra Lifesciences, Plainsboro, NJ, USA) were used in 60 patients (the collagen matrix group), and autologous fascial flaps were grafted in the remaining 60 patients (the fascia group). Twenty-four patients with combination use of a fascial flap and a collagen matrix graft were excluded in this study.

Participant flow diagram. MVD microvascular decompression
Operative technique
Patients were operated through the retrosigmoid approach in the lateral position. For the collagen matrix closure, we use “inlay and onlay” double grafting technique (Fig. 2). A larger size of a collagen sheet (approximately 1.5 times larger in diameter than the craniotomy size) was inserted intradurally (inlay placement) to have sufficient contact with the inner surface of the dura mater. The inlay graft was fixed to the dural edge with a running 4–0 braided nylon suture and fibrin glue to prevent migration. Then, the onlay collagen graft was placed extradurally to cover all areas of the exposed outer dura mater. For the fascia closure, a sufficient size of a thin fascial flap was harvested from the surface of the suboccipital muscles before making the muscle split and the craniotomy. The harvested fascia was kept in a moist gauze until use for the dural closure. The fascial flap was sutured in a watertight fashion with 4–0 braided nylon sutures. In both methods, no CSF leakage was confirmed with the Valsalva maneuver after completion of the dural reconstruction. In case a CSF leak was found, several sutures were added to ensure watertight closure. An artificial bone cement, calcium phosphate paste (BIOPEX-R®, HOYA Technosurgical, Tokyo, Japan), was then applied for cranioplasty in most patients except 8 patients who underwent re-exploration. No drainage tube was placed in all patients. Postoperative care, including a period of bed rest, the method of wound dressing, and the selection of antibiotics, was as per our standard protocols, which did not differ between the two groups.

Double grafting technique using inlay and onlay collagen sheets. a The retrosigmoid approach on the left in microvascular decompression for trigeminal neuralgia. A dural defect near the transverse-sigmoid junction is shown. The craniectomy size is approximately 3 cm in diameter. The transverse and sigmoid sinuses are illustrated in blue. The mastoid air cells are opened during a craniotomy and sealed with bone wax. b A larger collagen matrix graft (4.5 cm in diameter) than the craniectomy size is prepared for inlay use. The center of the inlay graft is marked with pyoctanin (purple). c The inlay graft is placed intradurally in the middle of the dural defect with reference to the center marker (purple). The yellow dashed circle illustrates the larger size of the inlay graft inserted intradurally. The inlay graft is lifted with forceps (black arrowhead) to attach the inner surface of the dura and fibrin glue is applied for fixation (white arrowhead). d The intradural space is filled with a sufficient amount of artificial cerebrospinal fluid (CSF) through a small gap (black arrowhead). e The inlay graft is bulging with water pressure and attached to the inner surface of the dura mater. f The dural edge is sutured to the inlay graft to ensure fixation (black arrowheads). This picture shows bulging of the inlay graft during Valsalva maneuver over 30 mmHg. CSF leakage is hardly seen at this step. g An onlay graft of the same size with the craniectomy is placed onto the outer dural surface for secure watertight closure. h Dural reconstruction is completed and reconfirmed watertight with repeated Valsalva maneuvers
Assessment of outcomes
Computed tomography (CT) was taken on postoperative day one in all patients. The maximum diameter of craniotomy was measured with axial images. Fluid density in the mastoid air cells is inspected and classified into four degrees (0: no fluid density, 1: fluid density limits posterior to the mastoid antrum, 2: fluid density entering the mastoid antrum, 3: fluid density reaching the tympanic cavity) (Fig. 3). Observation of the operative wound was monitored during the inpatient hospital stay and at the follow-up examination in our clinic. Patient information, surgical and radiological findings, and the incidence of wound complications, such as pseudomeningocele, incisional CSF leak, CSF rhinorrhea, subcutaneous abscess, and meningitis, were assessed between the collagen matrix group and the fascia group. In describing demographic characteristics, p values across dura closure categories were obtained by linear regression for continuous variables and by a χ2 test or the Mantel–Haenszel test for categorical variables. Each statistical test was set to be significant at p < 0.05 (2-sided p value). SAS software (version 9.4; SAS Institute, Inc., Cary, North Carolina) was used for all statistical analyses.

Postoperative radiological findings. a An axial slice of computed tomography on postoperative day 1 shows water density in the mastoid air cells over the sigmoid sinus (grade 1, white arrowhead). The water density may include saline used during the craniotomy. An artificial bone is used for cranioplasty. The yellow arrows indicate the size of the craniotomy. b Magnetic resonance imaging on postoperative day 11 demonstrates no increase of water in the mastoid air cells (white arrowhead), indicating no cerebrospinal fluid leakage occurs. The inlay collagen graft (black arrowheads) is securely attached to the inner surface of the dura mater with larger coverage size than the craniotomy (yellow arrows). The onlay graft is difficult to be recognized as it is compressed between the artificial bone and the dural surface
Results
Patient characteristics and radiological findings
Patient characteristics, radiological findings, CSF leakage, and infectious complications of each group are summarized in Table 1. The patient characteristics were not significantly different in both groups. The mean diameter of craniotomy was 21.2 mm in total. Mastoid air cells were opened in more than half of the cases of each group (57% in the fascia group, 53% in the collagen matrix group). Fluid density observed in the mastoid air cells postoperative day one showed mostly grade 0 to grade 1. Artificial bone cement was used in most cases (93%). Statistical analyses showed no significant difference in radiological findings of the two groups.
Operative results and follow-up outcomes
The follow-up period was not significantly different between the two groups (median 12 months). All complications were noticed within 3 months postoperatively, and no occurrence was noted thereafter. Overall CSF leaks were observed in 5 patients (4.2%) in total (5.0% in the fascia group, 3.3% in the collagen matrix group). Most of them (4 patients) were presented as pseudomeningoceles. No CSF rhinorrhea was found in this series. All CSF leaks were treated conservatively with repeated punctures or continuous lumbar drainage except one patient who required a repair surgery in the fascia group. There was no significant difference in CSF leaks between the two groups in the statistical analyses.
Infectious complications were found in 4 patients (3.4%) in total (5.1% in the fascia group, 1.7% in the collagen matrix group). Subcutaneous abscesses were found in 2 patients (3.3%) only in the fascia group. These two patients required debridement with the removal of the bone cement. No subcutaneous abscess was observed in the collagen matrix group. Aseptic meningitis was observed in one patient in each group. The collagen matrix group showed non-inferiority to the fascia group in infectious complications.
Discussion
Posterior fossa surgery is associated with a higher risk of CSF leak than supratentorial surgery. The incidence is reported between 0.3 and 33.3% in the literature (Table2) [2,3,4,5,6, 9,10,11,12, 15, 16, 18,19,20,21]. A CSF leak remains a potentially devastating complication of a retrosigmoid craniotomy that should be avoided. Primary dural closure is frequently not feasible due to shrinkage of the dura mater by desiccation and bipolar coagulation [5, 10]. An autologous graft, such as a fascial flap harvested on-site, is a practical solution in achieving watertight dural reconstruction to prevent CSF leak in posterior fossa surgery [3, 4, 11, 16, 20]. This method is well established in MVD, and it is therefore widely used at many institutions including our institute [3, 4, 11, 23]. Conventional fascial grafting at our institute demonstrated 5.0% of CSF leaks, which is a relatively low rate of complication when compared with previous reports; therefore, it is difficult to demonstrate significant differences in the statistical analyses due to a small number of complications (3.3%) in the collagen matrix double grafting even though the collagen matrix double grafting improved the rate of CSF leakage in this study. This simple method can be an effective alternative to conventional fascial grafting.
The disadvantage of collagen matrix grafting is its additional cost ($700–800 for an MVD craniotomy size) than conventional on-site autologous fascial grafting. Although the application may be limited due to the cost, it is valuable to have an alternative surgical technique. Harvesting a sufficient size of the fascia may have the potential risk of wound infection by creating a dead space, postoperative headache by damaging the lesser occipital nerve, and local atrophy of the subcutaneous and muscle layer [1, 7]. Double grafting is a useful technique for those with subcutaneous or muscle layers that are thin, such as re-do cases, elderly patients, patients who need to avoid infection risks such as diabetic patients, and those who care about cosmetic appearance. In this study, the double grafting collagen matrix demonstrated a decreased rate of wound infection. The fascial defect over the suboccipital muscles may cause donor site morbidity against infection and paucity of local tissue in repeat surgery or debridement [9]. We speculate that a double collagen matrix grafting is benefited from keeping the suboccipital fasciomuscular layers intact without harvesting the fascial layer.
All previous reports of the use of a collagen matrix graft were single layer use as a patch for a dural defect [9, 12, 14, 15], but there is no report of double grafting in the literature. Kshettry et al. reported the results of dural reconstruction by a single use of onlay graft in 84 cases of posterior fossa surgery [9]. They found relatively higher risks of complications: CSF leak in 11.9%, wound infection in 4.8%, aseptic meningitis in 7.1%, and pseudomeningocele in 10.7%. The present study regarding a small craniotomy for MVD surgery demonstrates that double layer grafting can provide a favorable CSF leak and infection rates as compared with previous studies of a single layer collagen matrix graft. The inlay graft may play a pivotal role in preventing CSF leaks because the inlay graft can have a larger area of contact with the dura mater rather than the onlay graft (Fig. 3). Narotam et al. reported histological evaluation of implanted collagen grafts in the long-term perspective [13]. There was no inflammatory reaction or cell infiltration found in the underlying brain section, suggesting the inlay collagen matrix may not be harmful to brain tissue. It is necessary to accumulate cases and do further research to ensure its safety in the long-term.
Limitations of the present study include those that are inherent to studies of retrospective design with the small number of patients and complications. Another limitation is the relatively short follow-up period of the patients. Although the complication rates in the current series were acceptable as compared with those in previous studies, a longer period of observation and accumulation of the number of cases are needed to confirm our conclusions.
Conclusion
A combination use of inlay and onlay collagen matrix grafts is comparable to a sole use of a fascial flap in terms of CSF leaks and infections. Although the application is restricted due to the cost, our double grafting method can be a safe and effective alternative to a fascial flap for dural reconstruction in some limited conditions.
References
Aihara N, Yamada H, Takahashi M, Inagaki A, Murakami S, Mase M (2017) Postoperative headache after undergoing acoustic neuroma surgery via the retrosigmoid approach. Neurol Med Chir (Tokyo) 57:634–640
Altaf I, Vohra AH, Shams S (2016) Management of cerebrospinal fluid leak following posterior cranial fossa surgery. Pak J Med Sci 32:1439–1443
Barker FG 2nd, Jannetta PJ, Bissonette DJ, Shields PT, Larkins MV, Jho HD (1995) Microvascular decompression for hemifacial spasm. J Neurosurg 82:201–210
Barker FG 2nd, Jannetta PJ, Bissonette DJ, Larkins MV, Jho HD (1996) The long-term outcome of microvascular decompression for trigeminal neuralgia. N Engl J Med 334:1077–1083
Bayazit YA, Celenk F, Duzlu M, Goksu N (2009) Management of cerebrospinal fluid leak following retrosigmoid posterior cranial fossa surgery. ORL J Otorhinolaryngol Relat Spec 71:329–333
Dubey A, Sung WS, Shaya M, Patwardhan R, Willis B, Smith D, Nanda A (2009) Complications of posterior cranial fossa surgery - an institutional experience of 500 patients. Surg Neurol 72:369–375
Ducic I, Felder JM 3rd, Endara M (2012) Postoperative headache following acoustic neuroma resection: occipital nerve injuries are associated with a treatable occipital neuralgia. Headache 52:1136–1145
Kinaci A, Algra A, Heuts S, O’Donnell D, van der Zwan A, van Doormaal T (2018) Effectiveness of dural sealants in prevention of cerebrospinal fluid leakage after craniotomy: a systematic review. World Neurosurg 118:368–376
Kshettry VR, Lobo B, Lim J, Sade B, Oya S, Lee JH (2016) Evaluation of non-watertight dural reconstruction with collagen matrix onlay graft in posterior fossa surgery. J Korean Neurosurg Soc 59:52–57
Lee YM, Ordaz A, Durcanova B, Viner JA, Theodosopoulos PV, Aghi MK, McDermott MW (2020) Cerebrospinal fluid leaks and pseudomeningocele after posterior fossa surgery: effect of an autospray dural sealant. Cureus 31:e8379
Linskey ME, Ratanatharathorn V, Peñagaricano J (2008) A prospective cohort study of microvascular decompression and gamma knife surgery in patients with trigeminal neuralgia. J Neurosurg 109:160–172
Litvack ZN, West GA, Delashaw JB, Burchiel KJ, Anderson VC (2009) Dural augmentation: part I-evaluation of collagen matrix allografts for dural defect after craniotomy. Neurosurgery 65:890–897
Narotam PK, van Dellen JR, Bhoola KD (1995) A clinicopathological study of collagen sponge as a dural graft in neurosurgery. J Neurosurg 82:406–412
Narotam PK, Reddy K, Fewer D, Qiao F, Nathoo N (2007) Collagen matrix duraplasty for cranial and spinal surgery: a clinical and imaging study. J Neurosurg 106:45–51
Narotam PK, Qiao F, Nathoo N (2009) Collagen matrix duraplasty for posterior fossa surgery: evaluation of surgical technique in 52 adult patients. J Neurosurg 111:380–386
Park JS, Kong DS, Lee JA, Park K (2007) Intraoperative management to prevent cerebrospinal fluid leakage after microvascular decompression: dural closure with a “plugging muscle” method. Neurosurg Rev 30:139–142
Sade B, Oya S, Lee JH (2010) Non-watertight dural reconstruction in meningioma surgery: results in 439 consecutive patients and a review of the literature. Clinical article J Neurosurg 114:714–718
Samii M, Günther T, Iaconetta G, Muehling M, Vorkapic P, Samii A (2002) Microvascular decompression to treat hemifacial spasm: long-term results for a consecutive series of 143 patients. Neurosurgery 50:712–719
Steinbok P, Singhal A, Mills J, Cochrane DD, Price AV (2007) Cerebrospinal fluid (CSF) leak and pseudomeningocele formation after posterior fossa tumor resection in children: a retrospective analysis. Childs Nerv Syst 23:171–174
Stoker MA, Forbes JA, Hanif R, Cooper C, Nian H, Konrad PE, Neimat JS (2012) Decreased rate of CSF leakage associated with complete reconstruction of suboccipital cranial defects. J Neurol Surg B Skull Base 73:281–286
Than KD, Baird CJ, Olivi A (2008) Polyethylene glycol hydrogel dural sealant may reduce incisional cerebrospinal fluid leak after posterior fossa surgery. Neurosurgery 63:ONS182–6; discussion ONS186–7
Venable GT, Roberts ML, Lee RP, Michael LM 2nd (2018) Primary dural closure for retrosigmoid approaches. J Neurol Surg B Skull Bas 79:330–334
Zhao Y, Chen L, Zhang J, You N, Liu Y, Yao A, Zhao K, Zhang J, Xu B (2020) Duraplasty with cervical fascia autograft to reduce postoperative complications of posterior fossa tumor surgery with suboccipital midline approach. World Neurosurg 134:e1115–e1120
Acknowledgements
We thank Ms. Lori Radcliffe for assistance with English language editing.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Conflict of interest
All authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Functional Neurosurgery - Pain
Rights and permissions
About this article

Cite this article
Inoue, T., Shitara, S., Shima, A. et al. Double collagen matrix grafting for dural closure in microvascular decompression: an alternative use of autologous fascial grafting. Acta Neurochir 163, 2395–2401 (2021). https://doi.org/10.1007/s00701-021-04856-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-021-04856-6