
Abstract
Background
Infratentorial supracerebellar approach via microscope still has some limitations in resection of pineal region tumors.
Methods
The authors describe a purely endoscopic infratentorial supracerebellar approach for resection of pineal region tumors with matched air-driven arm and navigation. The lateral oblique position is adopted. The same bimanual microsurgical techniques are utilized in this endoscopic approach with panoramic view and satisfying comfort.
Conclusions
Purely endoscopic resection of pineal region tumors using infratentorial supracerebellar approach is feasible. It may be considered as an alternative approach for certain pineal region tumors.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Relevant surgical anatomy
The pivotal neurostructures involved in the pineal region consist of the posterior wall of the third ventricle rostrally and cerebellar vermis caudally; the splenium of the corpus callosum dorsally; the corpora quadrigemina ventrally; and the pulvinar and the tentorial incisura bilaterally. The quadrigeminal cistern, corresponding to pineal region, communicates with the posterior pericallosal cistern superiorly, the ambient cisterns laterally, the velum interpositum anteriorly and superior cerebellar cistern posteriorly.
The pineal region contains the site of convergence of the internal cerebral veins, basal veins of Rosenthal, and multiple other tributaries of the galenic complex. Among the galenic tributaries, the precentral cerebellar vein originating on the superior cerebellar peduncles and terminates with the superior vermian vein in the great vein is of paramount importance.
The arterial structures of the pineal region are the medial posterior choroidal arteries, arising from the proximal part of the posterior cerebral artery; they frequently turn forward beside the pineal body in the quadrigeminal cistern and reach the velum interpositum.
Mostly, pineal region tumors are located in the midportion of the third ventricle and posteriorly to compress the anterior portion of the cerebellum; they are seldom beyond the undersurface of the velum interpositum, even though they attach to it at times. The tumor blood feeding comes mainly from the posterior medial and lateral choroidal arteries, with anastomoses to the pericallosal arteries and quadrigeminal arteries. Vein of Galen, internal cerebral veins, Rosenthal vein, and precentral cerebellar vein are involved in the site of the tumor.
Description of the technique
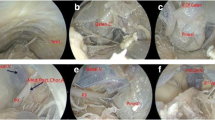
For the infratentorial supracerebellar approach, after intubation anesthesia, the patient’s head was fixed with a three-pin Mayfield holder. The patient was positioned lateral oblique with the upper body elevated 15 degrees, to benefit venous drainage. The neck was slightly flexed to enhance the surgeon’s comfort when approaching the tumor [3]. The antiseptic preparation was completed routinely. The size of the bone flap was approximately 4 × 3 cm, which crossed over the transverse sinus and contained the torcular region. The dura was opened in and turned over to the margin of the transverse sinus (Fig. 1). After fixing the dura with suturing, an endoscope (4-mm diameter, 18-cm length, 0-degree lenses; Karl Storz GmbH & Co., Tuttlingen, Germany) held in a matched, air-driven arm was introduced above the surgeon’s hands. The monitor was put in front of the surgeon. The surgical procedure was performed using the same microsurgical technique but illuminated by endoscope, which enabled a panoramic scenario and sharp details of the operative field along the midline trajectory. To open the quadrigeminal region, some bridging veins between the superior surface of the cerebellum and the tentorium were gradually sacrificed without any adverse consequence. We do not systematically coagulate and divide the vermian veins. Thereafter, the supracerebellar infratentorial corridor was gained without using a brain retractor. Next, the thickened and opaque arachnoid membrane over the quadrigeminal cistern was opened using microdissection techniques, thus uncovering the precentral cerebellar vein, which was sacrificed with impunity to further expose the tumor in the pineal region. Followed by intracapsular debulking, the superior and lateral margins of the tumor were dissected from the surrounding velum interpositum, pulvinar, walls of the third ventricle, and medial posterior choroidal artery. Accordingly, the tumor was totally extirpated in a piecemeal fashion. The posterior wall of the third ventricle was opened, so that the contained vital neurostructures were observed. The endoscope was used to further detect any residual portions, which were bound to be resected off, and verify total tumor removal. Equally important, the intraoperative clot near the aqueduct of Sylvius was removed, thus reducing the probability of postoperative hydrocephalus. After hemostasis was achieved, the dura was sutured in a watertight manner and the bone flap was repositioned (Video 1). If the patient presents with hydrocephalus, endoscopic third ventriculostomy (ETV) can be performed 1 week before tumor removal.

a Layout in the operating room. b The patient position and the skin incision. c The bone flap, TS transverse sinus, SS sagittal sinus. d The dura incision
The procedure of a purely endoscopic infratentorial supracerebellar approach of resecting a pineal region tumor (MPG 51456 kb)
Indications
Tumors with both cystic and solid consistency located within the quadrigeminal cistern (which is not beyond the splenium of the corpus callosum and the Galenic complex superiorly, the quadrigeminal plate inferiorly and the pulvinar bilaterally) can be removed via this endoscopic infratentorial–supracerebellar approach [1, 2, 5–7]. The tumors with soft and moderate texture but without artery encasement may be eligible for the technique. The tumors with massive calcification or rich blood supply are not good candidates.
Limitations
Limitations of the infratentorial supracerebellar approach have been profoundly discussed as the limitation of available surgical field and inconvenience in the case of confronting a very steep tentorium [4]. Despite offering a panoramic view and clear details, the current endoscope has its inherent shortcoming of two-dimensional images and blind region in proximity of the lens body. The main cause of transferring to microscope is the unclear vision hindered from bleeding and unskilled manipulations. Hence, the learning curve of endoscopy is imperative.
How to prevent complications
Efforts should be constantly made to avoid complications as follows: (1) the transverse sinus can be free of injury due to the proper bone opening; (2) adequate cerebellar relaxation, allowed by gravity, mannitol, slightly hyperventilation, cerebrospinal fluid releasing and sacrifice of few superior bridging veins other than retraction, is essential; (3) the veins in the path to the tumor must be protected as much as possible to prevent draining obstruction and consequent edema; (4) no resistance from the proximate side is permitted when advancing the endoscope.
Specific perioperative considerations
The perioperative considerations were the same as routine surgical treatment of pineal tumors.
Specific information to give to the patient about surgery and potential risks
Surgical excision plays an irreplaceable role in the therapeutic modalities of certain pineal region tumors [7]. An endoscope is an alternative surgical instrument with inherent advantages from different lighting principle with flashlight effect. Specific complications of the endoscope itself could be avoided owing to our extensive experience from endoscopic skull base surgery. However, the clinical outcome may not be improved affirmatively and the operative complications may not be avoided absolutely.
Key points
-
1.
The lateral oblique position facilitates the surgeon’s manipulation and the layout of the endoscope and navigation. The chief surgeon’s comfortable experience may be promptly improved.
-
2.
The incision and bone flap are the same or slightly smaller than an operation with a microscope.
-
3.
An air-driven arm plays a crucial role in endoscopic surgery. An air-driven arm ensures steady fixation of the endoscope, thus eliminating manual handling and freeing the chief surgeon’s bimanual operation.
-
4.
The navigation confirms the initial direction towards to quadrigeminal cistern and the tumor, thus eliminating unintended injury.
-
5.
The endoscope actually shortens the working distance and offers better comfort to the surgeon compared with a microscope because the chief surgeon may stand closer to the surgical field.
-
6.
Panoramic and extended views afforded by an endoscope promote safe surgical dissection and resection. The same bimanual microsurgical techniques are used in this endoscopic approach.
-
7.
When advancing the endoscope, prevent both the tip and body of the endoscope from injuring adjacent neurovascular structures, with no sparing effort.
-
8.
The flashlight effect enabled by an endoscope may reduce the retraction of the cerebellum after crossing the culmen.
-
9.
Proprioception with moving of the endoscope may offset the disadvantage of two-dimensional vision.
-
10.
The learning curve of using an endoscope is imperative.
References
Broggi M, Darbar A, Teo C (2010) The value of endoscopy in the total resection of pineocytomas. Neurosurgery 67:s159–s165
Gore PA, Gonzalez LF, Rekate HL, Nakaji P (2008) Endoscopic supracerebellar infratentorial approach for pineal cyst resection: technical case report. Neurosurgery 62:108–109, Discussion 109
Gu Y, Zhang XB, Yu Y (2013) Endoscope-assisted microsurgical resection for pineal region tumors: preliminary experience. J Pediatr Oncol 1:17–22
Hart MG, Santarius T, Kirollos RW (2013) How I do it—pineal surgery: supracerebellar infratentorial versus occipital transtentorial. Acta Neurochir 155:463–467
Sood S, Hoeprich M, Ham SD (2011) Pure endoscopic removal of pineal region tumors. Childs Nerv Syst 27:1489–1492
Thaher F, Kurucz P, Fuellbier L, Bittl M, Hopf NJ (2014) Endoscopic surgery for tumors of the pineal region via a paramedian infratentorial supracerebellar keyhole approach (PISKA). Neurosurg Rev 37:677–684
Tseng KY, Ma HI, Liu WH, Tang CT (2012) Endoscopic supracerebellar infratentorial retropineal approach for tumor resection. World Neurosurg 77:391–399
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
This study protocol was approved by the Research Ethics board in our hospital. All patients signed a written informed consent form that they will be enrolled in this study.
Conflict of interest
None.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Gu, Y., Hu, F. & Zhang, X. Purely endoscopic resection of pineal region tumors using infratentorial supracerebellar approach: How I do it. Acta Neurochir 158, 2155–2158 (2016). https://doi.org/10.1007/s00701-016-2895-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-016-2895-0