
Abstract
Background
Trigeminal neuralgia (TN) is primarily diagnosed by symptoms and patient history. Magnetic resonance (MR) imaging can be helpful in visualizing the neurovascular compression of the trigeminal nerve in TN patients, but the current parameters used as diagnostic markers for TN are less than optimal. The aim of this study is to assess whether the angle between the trigeminal nerve and the pons (the trigeminal-pontine angle) on the affected side of patients with idiopathic TN differs from that of the unaffected side and that found in controls without TN.
Methods
A case-control study of 30 clinically diagnosed idiopathic TN patients aged 30 to 79 years and 30 age- and sex-matched controls was conducted. We compared the trigeminal-pontine angle and trigeminal nerve atrophy via fast-imaging employing steady-state acquisition (FIESTA) MR imaging.
Results
A sharp trigeminal-pontine angle was observed in 25 patients (25/30) on the affected side. As such, the mean angle of the trigeminal nerve on the affected side (40.17) was significantly smaller than that on the unaffected side (48.91, p = 0.001) and that in the control group (52.02, p < 0.001).
Conclusions
A sharp trigeminal-pontine angle on the affected side was found in idiopathic TN patients by FIESTA imaging. This suggests that a sharp trigeminal-pontine angle increases the chance of neurovascular compression on the medial side of the trigeminal nerve.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Trigeminal neuralgia (TN) is characterized by recurrent episodes of brief, sudden, stabbing pain that is usually unilateral and is distributed through one or more branches of the fifth cranial nerve [17]. Although trigeminal neuralgia is diagnosed by symptoms and patient history, magnetic resonance (MR) imaging, especially fast-imaging employing steady-state acquisition (FIESTA) imaging and constructive interference steady state (CISS) imaging, are useful in visualizing the neurovascular compression between the trigeminal nerve and the surrounding blood vessels [15]. It is known that atrophy of the trigeminal nerve, a small cerebellopontine angle (CPA) cistern, a small pontomesencephalic cistern, and the length of the cisternal segment of the trigeminal nerve are diagnostic markers for TN [13, 21, 23]. However, nerve atrophy on MR imaging is hard to delineate, and the volume of the CPA cistern is difficult to measure.
Although dolichoectatic vessels or large offending vessels have occasionally been found in patients with TN [4], and Gudmundsson et al. reported on the angle between the longest diameter of the cross-section and the long axis of the body [6], a sharp angle between the trigeminal nerve and the pons has not been recognized as a clinically meaningful parameter. This angle difference is thought to be one of the structural features that contribute to Caucasians having a higher prevalence of TN than Asians, and is due to Caucasians having a scaphocephalic skull morphology [11, 12, 26]. The focus of the novel work presented here is to demonstrate the clinical utility of measuring the angle between the trigeminal nerve and the pons (trigeminal-pontine angle).
It is thought that a sharp angle may increase the chance of neurovascular compression on the medial side of the trigeminal nerve. Thus, we hypothesized that a sharp trigeminal-pontine angle may be a useful additional diagnostic factor for idiopathic TN. We also examined atrophy of the trigeminal nerve by dividing the segment and confirmed previous reported parameters. To test our hypothesis, patients with idiopathic TN and a control group underwent FIESTA imaging.
Materials and methods
Patients
Between February 2006 and January 2010, 30 patients with TN who were treated at our center were included in this study. Patients diagnosed with secondary trigeminal neuralgia or tic convulsif and those who had bilateral symptoms were excluded from the study. The patient population included 24 women and six men and had a mean age of 60.7 years (range 30–79 years). Sixteen patients had right-sided TN, and 14 patients had TN on the left side. All but five patients in this study complained of V2 or V3 branch pain, and the average symptom duration at diagnosis was 75 months. The mean score of the patients on the Barrow Neurological Institute (BNI) pain scale was 3.7, and two patients complained of sensory changes. The clinical manifestations of TN found in the patients in this study are summarized in Table 1. Sixteen patients underwent microvascular decompression, three patients were treated by glycerol injection, two patients underwent radiofrequency ablation, one patient underwent Novalis stereotactic radiosurgery (BrainLAB, Heimstetten, Germany), and nine patients were treated conservatively with medication.
The patients were matched for age and sex with patients with hemifacial spasm, who served as the control group, and both groups were evaluated by FIESTA MR imaging (Table 2).
Imaging procedures
Patients were evaluated by MR imaging at the time of diagnosis. Examinations were performed with a clinical 3.0-T whole-body MR system (SIGNA excite HDXT 3.0 T; GE Healthcare) with an eight-channel head coil. Initially, multiplane localizations were performed to ensure the scan range. Imaging with the Fast Imaging Employing Steady State Acquisition protocol (TR/TE, 6.5/2.3; FOV, 160-mm flip angle, 60; matrix, 448 × 256; axial thickness, 1.0 mm; bandwidth, 62.5) was subsequently performed.
All images were transferred to a post-processing workstation (Advantage Workstation, ADW 4.3, GE Medical Systems). Multiplanar reconstruction was utilized on the workstation to evaluate the various cerebellopontine angle structures. Images were reconstructed in the sagittal, coronal, and axial planes. The reformatted images were magnified to facilitate the measurement of the diameter and cross-sectional area of the target.
Imaging analysis
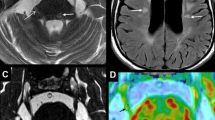
Two observers who were blinded to which side of a patient’s face was symptomatic independently measured diagnostic parameters. For each parameter in the patients we used the average of the two observers’ measurements, whereas for the controls we used the average of both sides of the face. The angle between the medial margin of the trigeminal nerve and the anterior surface of the pons at the root exit zone (REZ) was measured in the axial view with the Marosis m-view program (Infinitt Co., Seoul, Korea) (Fig. 1). Additionally, we measured the cross-sectional area of the CPA cistern between the anterolateral surface of the pons and cerebellum and the posterior surface of the petrous bone. Atrophy of the trigeminal nerve was measured by separating the axial cisternal segment at the level of the REZ, the axial cisternal and ganglional segments at the level of the REZ, and the coronal cross-sectional area at the ambient cistern. The short-axis length of the trigeminal nerve was measured in the middle portion of the cisternal segment of the nerve at the level of the REZ. The length of the cisternal segment of the trigeminal nerve was measured as the length from the REZ to the narrow aperture of Meckel’s cave, and the cross-sectional area of Meckel’s cave was measured as the space between the cerebellar tentorium (laterally), the lateral wall of the cavernous sinus (medially), and the margin of the petrous bone (posteriorly). Parameters were measured in both patients and the control group (Fig. 2).

Delineation of both angles between the trigeminal nerve and the pons

Imaging parameters. Cross-sectional area of the cisternal segment of the trigeminal nerve (a), cross-sectional area of the cisternal and ganglional segment of the trigeminal nerve (b), cross-sectional area of trigeminal nerve in coronal view (c), short-axis length of the trigeminal nerve (d), cross-sectional area of the CPA cistern (e), length of the cisternal segment of the trigeminal nerve (f), cross-sectional area of Meckel’s cave (g)
Statistical analysis
The trigeminal-pontine angle and the atrophy of the trigeminal nerve were compared in the affected side of TN patients versus the unaffected side and controls by the t test for dependent samples. All analyses were performed with SPSS Version 15.0 for Windows (SPSS Inc., Chicago, IL, USA). A probability value of p = 0.05 or less was accepted as indicating statistical significance.
Results
Nerve-vessel conflict was present on MR imaging on the symptomatic side in 24 out of 30 patients, whereas six patients presented with no definite offending vessel on MRI. In three of these six patients, a nerve-vessel conflict was identified during the operation. Due to this difference in MR imaging findings among the patients, in addition to comparing the symptomatic side of the patients (affected side) with the patients’ unaffected side and controls, we also stratified the patients into a definite offending vessel group (definite offenders) and an indefinite offending vessel group (indefinite offenders) and compared these two groups in terms of various parameters. Table 3 show comparisons of various parameters between the affected side of patients with trigeminal neuralgia with the non-affected side and the control group.
Sharp trigeminal-pontine angle in TN patients
There were statistically significant differences in the trigeminal-pontine angle in the affected side compared to the unaffected side and the control group (p = 0.001 and p < 0.001, respectively). The mean angle was 40.17 (range 22.8–68.98) on the affected side, 51.39 (range 25.80–70.74) on the unaffected side, and 52.02 (range 37.35–68.44) in the control group. A relatively sharp angle was present on the affected side in 25 patients (83.33%) and on the unaffected side in five patients. In the control group, there was not a significant difference in the trigeminal-pontine angle between the right and left sides.
Atrophy of the trigeminal nerve
The mean cross-sectional area of the cisternal segment of the trigeminal nerve was 22.73 mm2 (range 8.58–45.61 mm2) on the affected side and 25.83 mm2 (range 10.77–54.56 mm2) on the unaffected side. Thus, the mean cross-sectional area of the cisternal segment was significantly smaller (87.99%) on the affected side than the unaffected side (p = 0.005). In the control group, there was not a significant difference in the cross-sectional area of the cisternal segment between the right and left sides.
The mean cross-sectional area of the cisternal and ganglional segment of the trigeminal nerve was 37.07 mm2 (range 15.24–61.41 mm2) on the affected side and 41.28 mm2 (range 14.57–70.65 mm2) on the unaffected side, making the mean cross-sectional area of the cisternal and ganglional segment significantly smaller (89.80%) on the affected side than the unaffected side (p = 0.003). In the control group, there was no significant difference between the right side and the left side in the cross-sectional area of the cisternal and ganglional segment.
Nerve atrophy, as measured by the cross-sectional short-axis length of the trigeminal nerve, was observed in 25 patients (83.0 %) on the affected side. The mean cross-sectional length of the trigeminal nerve was 3.20 mm on the affected side and 3.47 mm on the unaffected side, but this difference was not significant.
The length of the cisternal segment of the trigeminal nerve and the cross-sectional area of the CPA cistern and Meckel’s cavity
The mean length of the cisternal segment of the trigeminal nerve on the affected side was 7.20 mm, whereas it was 8.10 mm on the unaffected side. Hence, the mean length of the cisternal segment was significantly shorter (88.89 %) on the affected side than the unaffected side (p = 0.001). In the control group, there was no significant difference in the length of the cisternal segment between the right and left sides.
The mean cross-sectional area of the CPA cistern was significantly smaller (86.62 %, p = 0.001) on the affected side (85.75 mm2, range 29.61–148.05 mm2) than the unaffected side (98.99 mm2, range 50.11–177.58 mm2). There was no significant difference in the cross-sectional area of the CPA cistern between the right and left sides of the control group.
The mean cross-sectional area of Meckel’s cave was 80.45 mm2 (range 32.12–141.01 mm2) on the affected side and 78.98 mm2 (range 25.06–136.23 mm2) on the unaffected side, and there was no significant difference between the affected and unaffected sides.
Comparison by MR imaging of the trigeminal-pontine angle between definite offenders and indefinite offenders
Among TN patients, 24 were classified as definite offenders and six were classified as indefinite offenders. There was no statistically significant difference in the trigeminal-pontine angle between these groups.
Discussion
MR imaging is useful in evaluating neurovascular conflict of the trigeminal nerve at the REZ and helpful as a preoperative tool when trigeminal neuralgia is diagnosed by symptoms and patient history [2, 10, 16, 27]. However, the trigeminal nerve is sometimes hard to distinguish from the surrounding blood vessels in T1-weighted and T2-weighted imaging. FIESTA imaging and CISS imaging, which provide higher spatial resolution, have been investigated as tools for the evaluation of cranial nerves and the surrounding structures [7, 20, 24, 28–30]. These imaging modalities provide better contrast between the parenchyma of the central nervous system and the cerebrospinal fluid by flow compensation. In addition, the delineation of fine anatomic structures in the cerebrospinal fluid can be achieved [7, 18, 24]. Chavez et al. were able to clearly image the trigeminal nerve complex (nerve root entry zone, trigeminal ganglion, nerve roots, and vascular structures), including visualization of the branches of the trigeminal nerve, inside Meckel’s cave in 14 of 15 patients while using FIESTA imaging for the targeting and planning of stereotactic radiotherapy [3]. In this study, we used FIESTA imaging to detect the trigeminal-pontine angle and trigeminal nerve atrophy.
Neurovascular contact between the trigeminal nerve and a blood vessel can also be found in individuals not affected by TN. Contact between a trigeminal nerve root and an artery in the prepontine cistern can be seen as anatomical variant [1, 22]. Based on surgical experience, Sindou et al. suggested a ribbon-shaped and angulated root was a possible anatomic factor [25]. Due to the unclear MR imaging findings associated with trigeminal neuralgia, there have been efforts to describe unique MR imaging findings in trigeminal neuralgia patients. Miller et al. reported that neurovascular compression is more severe and more proximal in TN patients compared to those asymptomatic [19].
Atrophy of the trigeminal nerve as the result of nerve-vessel conflict in trigeminal neuralgia patients has been revealed by MR imaging in several reports [5, 13, 14]. Nerve atrophy is thought to be a late consequence of chronic physical stress following demyelination [21]. Erbay et al. measured a single cross-sectional coronal area of the trigeminal nerve [5], and Park et al. measured the volume of the cisternal segment of trigeminal nerve [21]. Both of these studies showed statistically significant results.
Herweh et al. used DTI to assess the area known to be susceptible to bony artifacts and suggested that FA reduction is caused by tissue damage associated with demyelination [8]. However, the sample size was very small, and anisotropy is seldom involved in an MR imaging protocol [8]. Horinek et al. found no association between the clinical neurovascular conflict and the size of the posterior fossa and its substructures, including the pontomesencephalic cistern and Meckel’s cave [9]. Rasche et al. assumed that a smaller cistern may increase the chance for neurovascular conflict, and a prospective study demonstrated significant volumetric differences of the pontomesencephalic cistern in patients with unilateral TN [23]. A study by Park et al. measured the cross-sectional area of the CPA cistern and the length of the cisternal segment of the trigeminal nerve and suggested that the CPA cistern might be smaller on the affected side in TN patients [21]. Vergani at al. reported that MRI/MRA had a sensitivity of 96% and a specificity of 75% for detecting NVC in their study on the pre-operative role of MRI for TN [27]. They also found that there was no correlation between the pre-operative imaging and the clinical outcome. Leal et al. reported a similar result with a specificity of 100% and concluded that MRI is reliable in detecting and grading NVC [16]. In their anatomical study of the posterior fossae of patients with TN, Horinek et al. concluded that the only visible factor is the atrophy of the nerve [9]. In 2002, Sindou et al. reported that NVC was the principal finding in pre-op MRI and operative exploration but added that other anatomical findings may be present, including a sharp angulated root, atrophy of the nerve, and a thick arachnoid membrane [25]. Ongoing clinical research has led to preoperative imaging for TN becoming widely applicable in the clinical fields.
In this study, we found a sharper angle between the trigeminal nerve and the pons in TN patients compared to controls and demonstrated nerve atrophy with FIESTA imaging. These results lend further credence to our hypothesis that states a sharp trigeminal-pontine angle increases the chance of neurovascular conflict. Our results showed a significantly sharper trigeminal-pontine angle on the affected side in TN patients compared to the unaffected side and controls. This measurement can be relatively easily applied to clinical practice. Atrophy of the trigeminal nerve was calculated by dividing the nerve into cisternal and ganglional segments by a cross-sectional view, and significant differences were found for both measurements when the affected side was compared to the unaffected side and controls. There were some limitations to this study. First, the sample size was small. Although we showed there was no difference in the nerve-pontine angle between the definite offenders and the indefinite offenders, the value of this angle as a diagnostic supplementary marker will be overestimated due to the study included an insufficient number of indefinite offender patients. Further, we only checked a single cross-sectional area, and it is possible that the true volume of the trigeminal nerve was miscalculated despite the FIESTA sequence being evaluated at an axial thickness of 1 mm.
Conclusions
In summary, we have shown that a sharp trigeminal-pontine angle observed in 3D-FIESTA imaging could lead to TN by increasing the likelihood for neurovascular conflict. Additionally, nerve atrophy was shown in cross-sectional axial and coronal imaging by dividing the nerve into ganglional and cisternal segments. These features are thought to be potential supplementary markers for the diagnosis of trigeminal neuralgia.
References
Adamczyk M, Bulski T, Sowinska J, Furmanek A, Bekiesinska-Figatowska M (2007) Trigeminal nerve—artery contact in people without trigeminal neuralgia—MR study. Medical science monitor: international medical. J Exp Clin Res 13(Suppl 1):38–43
Akimoto H, Nagaoka T, Nariai T, Takada Y, Ohno K, Yoshino N (2002) Preoperative evaluation of neurovascular compression in patients with trigeminal neuralgia by use of three-dimensional reconstruction from two types of high-resolution magnetic resonance imaging. Neurosurgery 51:956–961, discussion 961–952
Chavez GD, De Salles AA, Solberg TD, Pedroso A, Espinoza D, Villablanca P (2005) Three-dimensional fast imaging employing steady-state acquisition magnetic resonance imaging for stereotactic radiosurgery of trigeminal neuralgia. Neurosurgery 56:E628, discussion E628
El-Ghandour NM (2010) Microvascular decompression in the treatment of trigeminal neuralgia caused by vertebrobasilar ectasia. Neurosurgery 67:330–337
Erbay SH, Bhadelia RA, O’Callaghan M, Gupta P, Riesenburger R, Krackov W, Polak JF (2006) Nerve atrophy in severe trigeminal neuralgia: noninvasive confirmation at MR imaging–initial experience. Radiology 238:689–692
Gudmundsson K, Rhoton AL Jr, Rushton JG (1971) Detailed anatomy of the intracranial portion of the trigeminal nerve. J Neurosurg 35:592–600
Hatipoglu HG, Durakoglugil T, Ciliz D, Yuksel E (2007) Comparison of FSE T2W and 3D FIESTA sequences in the evaluation of posterior fossa cranial nerves with MR cisternography. Diagn Interv Radiol 13:56–60
Herweh C, Kress B, Rasche D, Tronnier V, Troger J, Sartor K, Stippich C (2007) Loss of anisotropy in trigeminal neuralgia revealed by diffusion tensor imaging. Neurology 68:776–778
Horinek D, Brezova V, Nimsky C, Belsan T, Martinkovic L, Masopust V, Vrana J, Kozler P, Plas J, Krysl D, Varjassyova A, Ghaly Y, Benes V (2009) The MRI volumetry of the posterior fossa and its substructures in trigeminal neuralgia: a validated study. Acta Neurochir (Wien) 151:669–675
Hutchins LG, Harnsberger HR, Jacobs JM, Apfelbaum RI (1990) Trigeminal neuralgia (tic douloureux): MR imaging assessment. Radiology 175:837–841
Hyun SJ, Kong DS, Park K (2010) Microvascular decompression for treating hemifacial spasm: lessons learned from a prospective study of 1,174 operations. Neurosurg Rev 33:325–334, discussion 334
Kamiguchi H, Ohira T, Ochiai M, Kawase T (1997) Computed tomographic analysis of hemifacial spasm: narrowing of the posterior fossa as a possible facilitating factor for neurovascular compression. J Neurol Neurosurg Psychiatry 62:532–534
Kress B, Rasche D, Fiebach J, Tronnier V, Sartor K, Stippich C (2004) MR volumetry of the trigeminal nerve in patients with unilateral facial pain. RoFo: Fortschritte auf dem Gebiete der Rontgenstrahlen und der Nuklearmedizin 176:719–723
Kress B, Schindler M, Rasche D, Hahnel S, Tronnier V, Sartor K, Stippich C (2005) MRI volumetry for the preoperative diagnosis of trigeminal neuralgia. Eur Radiol 15:1344–1348
Leal PR, Froment JC, Sindou M (2010) MRI sequences for detection of neurovascular conflicts in patients with trigeminal neuralgia and predictive value for characterization of the conflict (particularly degree of vascular compression). Neuro-Chirurgie 56:43–49
Leal PR, Hermier M, Froment JC, Souza MA, Cristino-Filho G, Sindou M (2010) Preoperative demonstration of the neurovascular compression characteristics with special emphasis on the degree of compression, using high-resolution magnetic resonance imaging: a prospective study, with comparison to surgical findings, in 100 consecutive patients who underwent microvascular decompression for trigeminal neuralgia. Acta Neurochir (Wien) 152:817–825
Merskey H, Bogduk N (1994) Classification of chronic pain: descriptions of chronic pain syndromes and definitions of pain terms. IASP Press, Seatle, WA, 59–71
Mikami T, Minamida Y, Yamaki T, Koyanagi I, Nonaka T, Houkin K (2005) Cranial nerve assessment in posterior fossa tumors with fast imaging employing steady-state acquisition (FIESTA). Neurosurg Rev 28:261–266
Miller JP, Acar F, Hamilton BE, Burchiel KJ (2009) Radiographic evaluation of trigeminal neurovascular compression in patients with and without trigeminal neuralgia. J Neurosurg 110:627–632
Okumura Y, Suzuki M, Takemura A, Tsujii H, Kawahara K, Matsuura Y, Takada T (2005) Visualization of the lower cranial nerves by 3D-FIESTA. Nihon Hoshasen Gijutsu Gakkai zasshi 61:291–297
Park SH, Hwang SK, Lee SH, Park J, Hwang JH, Hamm IS (2009) Nerve atrophy and a small cerebellopontine angle cistern in patients with trigeminal neuralgia. J Neurosurg 110:633–637
Peker S, Dincer A, Necmettin Pamir M (2009) Vascular compression of the trigeminal nerve is a frequent finding in asymptomatic individuals: 3-T MR imaging of 200 trigeminal nerves using 3D CISS sequences. Acta Neurochir (Wien) 151:1081–1088
Rasche D, Kress B, Stippich C, Nennig E, Sartor K, Tronnier VM (2006) Volumetric measurement of the pontomesencephalic cistern in patients with trigeminal neuralgia and healthy controls. Neurosurgery 59:614–620, discussion 614–620
Sheth S, Branstetter BFT, Escott EJ (2009) Appearance of normal cranial nerves on steady-state free precession MR images. Radiographics: a review publication of the Radiological Society of North America, Inc. 29:1045–1055
Sindou M, Howeidy T, Acevedo G (2002) Anatomical observations during microvascular decompression for idiopathic trigeminal neuralgia (with correlations between topography of pain and site of the neurovascular conflict). Prospective study in a series of 579 patients. Acta Neurochir (Wien) 144:1–12, discussion 12–13
Tan EK, Chan LL (2004) Clinico-radiologic correlation in unilateral and bilateral hemifacial spasm. J Neurol Sci 222:59–64
Vergani F, Panaretos P, Penalosa A, English P, Nicholson C, Jenkins A (2011) Preoperative MRI/MRA for microvascular decompression in trigeminal neuralgia: consecutive series of 67 patients. Acta Neurochir(Wien) 153(12):2377–2381
Xie T, Zhang XB, Yun H, Hu F, Yu Y, Gu Y (2011) 3D-FIESTA MR images are useful in the evaluation of the endoscopic expanded endonasal approach for midline skull-base lesions. Acta Neurochir (Wien) 153:12–18
Yoshino N, Akimoto H, Yamada I, Nagaoka T, Tetsumura A, Kurabayashi T, Honda E, Nakamura S, Sasaki T (2003) Trigeminal neuralgia: evaluation of neuralgic manifestation and site of neurovascular compression with 3D CISS MR imaging and MR angiography. Radiology 228:539–545
Yousry I, Camelio S, Schmid UD, Horsfield MA, Wiesmann M, Bruckmann H, Yousry TA (2000) Visualization of cranial nerves I-XII: value of 3D CISS and T2-weighted FSE sequences. Eur Radiol 10:1061–1067
Acknowledgments
The authors would like to thank Hye Young Yu (R.N.), Ju-Mi Kim (R.N.), and Hyouk Sang Kwon (BS) for data acquisition.
Disclosure of Funding
None.
Financial Support and Industry Affiliations
None.
Conflict of Interest
None.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
ESM 1
(JPEG 9 kb)
Rights and permissions
About this article
Cite this article
Ha, S.M., Kim, S.H., Yoo, E.H. et al. Patients with idiopathic trigeminal neuralgia have a sharper-than-normal trigeminal-pontine angle and trigeminal nerve atrophy. Acta Neurochir 154, 1627–1633 (2012). https://doi.org/10.1007/s00701-012-1327-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-012-1327-z