
Abstract
Purpose
Removal of tuberculum sella (TS) meningiomas is traditionally performed through transcranial approaches. Wide use of the endoscope in transphenoidal pituitary surgery is recently accessible through the tuberculum sellae with an endoscope-assisted or purely endoscopic technique. Extended endoscopic approach is an important and alternative route for meningiomas, which are located on the midline originating from the tuberculum sella. However, cerebrospinal fluid (CSF) leakage is an important problem in extended endoscopic approaches. In this report, we discuss surgical limitations and nuances of endoscopic transphenoidal approach from a retrospective analysis of nine patients with TS meningiomas.
Methods
Endoscopic transphenoidal approach was performed for seven women and two men (mean age, 51.1 years; age range, 32–78 years) with TS meningiomas between July 2007 and March 2010 in the Department of Neurosurgery, Kocaeli, Turkey.
Results
Total removal was achieved in six of nine patients. An improvement of the preoperative visual deficits was observed in six of the nine patients. Multilayer closure was performed for reconstruction, and lumbar external drainage was used for all patients for 3–5 days. CSF leakage was not seen in any of the patients after the operation and removal of the drainage.
Conclusion
Endoscopic extended transphenoidal approach is still not a standardized procedure for TS meningiomas, but it may be considered as an alternative procedure in selected cases.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Tuberculum sellae meningiomas (TSM) are conventionally removed through different surgical transcranial approaches including bifrontal or unifrontal and pterional or frontolateral approaches with the use of the microscopic techniques. Tuberculum sellae meningiomas account for about 3% of all intracranial meningiomas. Surrounding important neurovascular structures is one of the difficulties in the surgical treatment of these tumors [1, 10].
Removal of extrasellar lesions via transphenoidal approach is being used increasingly. “Extended transsphenoidal route,” which is a modification of the standard transsphenoidal exposure whichever sublabial, supraorbital keyhole or endonasal, microscopic, or endoscopic is being used for anterior cranial base located tumors that were previously operated on solely via transcranial approaches [3, 4, 8, 10, 11, 15, 17, 26, 27].
The extensive use of the endoscope in transphenoidal pituitary surgery has recently offered to the extension of the approach through the tuberculum sellae with purely endoscopic technique [2, 7–9, 16, 31].
In endoscopic approaches, higher rates of CSF leakage for tuberculum sellae meningiomas were reported [16]. In this report, we discussed endoscopic transphenoidal approach from a retrospective analysis of nine patients with TS meningiomas, who had been treated at the Department of Neurosurgery in Kocaeli University.
Methods
Three hundred thirty-four endoscopic transphenoidal approaches were performed since September 1997 in Kocaeli University, Department of Neurosurgery, Turkey, and between July 2007 and March 2010, seven women and two men (mean age, 51.1 years; age range, 32–78 years) underwent an extended endoscopic transphenoidal approach for the treatment of TS meningiomas (Table 1). None of the patients had undergone previous surgery or radiation therapy. None had experienced pituitary dysfunction.
All patients underwent preoperative and postoperative formal visual field and visual acuity evaluations.
Symptoms
All patients complained visual blurriness and had variable degrees of visual field and/or visual acuity defects. Two patients showed right temporal hemianopia for a duration of 9 and 6 months. Two patients reported total visual loss in her right eye for a duration of 15 and 20 months and left temporal hemianopia for 5 and 13 months, and one patient reported bitemporal hemianopia for 4 months. Bilateral total visual loss was seen in one patient for 1 year and left total visual loss was seen in one patient for 2 months. Five of nine patients had variable visual acuity defect (Table 1).
Radiologic evaluation
Preoperative neuroradiological evaluation included sellar pre- and post-contrast (gadolinium diethylenetriamine penta-acetic acid) magnetic resonance imaging (MRI) scans and paranasal sinus CT scans to define the relationships between the sphenoid, the sella, and the other bone structures that were involved. The tumor size was calculated according to de Divitiis et al. classification based on Yaşargil’s criteria on the preoperative MRI scans [10] (Grade I—less than 20 mm, Grade II—20 to 40 mm, and Grade III—more than 40 mm. The series include two lesions considered as Grade I, six lesions considered Grade II, and one patient considered as Grade III).
An early (within 24 h) postoperative neuroradiologic evaluation with MRI scan was performed and next MRI scan was scheduled 3 months later after surgery. In the third postoperative month, endoscopic evaluation of the patient was performed.
Surgical approach
Patient is placed supine fixed by Mayfield and turned slightly on a horizontal plane toward the surgeon and the head extended slightly on the sagittal plane. Before the procedure adrenaline applied paddies were inserted through the both nostrils. The procedure was performed using a rigid endoscope (Karl Storz, Tuttlingen, Germany) and additional tools like a highspeed microdrill with different size hand pieces, modified curets and aspirators, ultrasonic aspirator, micro-Doppler probe, and navigation system (Medtronic Neuronavigation, Stealth Station Trion) for the last four cases.
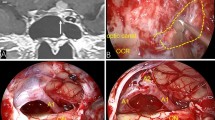
After viewing choana and sphenoethmoid recess, middle turbinate was resected and its mucoperichondrium was prepared thus it could be used for the closure. Middle turbinate of the other nasion was lateralized for binostril approach. Anterior sphenoidotomy was performed removing posterior nasal septum, rostrum, and perpendicular lamina by microdrill. Clivus, sellar floor, opticocarotid recess, and planum sphenoidale were visualized (Fig. 1). Tuberculum sella was opened by microdrill and ronguer superiorly setting the area between optic tuberans as a borderline inferiorly. Dura is coagulated and incised vertically.

Forty-nine-year-old female with Grade II tuberculum sellae meningioma (PN: 4). Intraoperative view of posterior sphenoid sinus wall after removal of anterior sphenoid wall. PS planum sphenoidale, TS tuberculum sellae, SF sphenoid wall, OP optic protuberance, CL clivus
Superior extracapsular dissection was performed after internal debulking of the tumor for Grade I lesions and Grade II lesions with dimensions below 3 cm (Fig. 2). Tumor was removed totally dissecting from frontal basis, arterial complex, and optic chiasm. In Grade II lesions with dimensions above 3 cm, following dural incision, internal debulking was performed, and sharp and blunt dissection were used for the dissection of the lesion from optic nerve and optic chiasm, arterial complex, pituitary stalk, and diaphragma with four-hand technique, and total removal of the tumor was achieved (Fig. 3). In cases with tumor extension into the optic canal, the bone and dura covering the optic canal in the superolateral part of the sphenoid sinus has been opened to expose the optic nerve in the optic canal.

Intraoperative view of superior extracapsular dissection and internal debulking of the tumor. T tumor

Intraoperative view of the case with Grade II tuberculum sellae meningioma; 59-year-old female (PN: 6). a Tumor compressing right optic nerve inferiorly. b After removal of the tumor. ON optic nerve, A1 and A2 anterior cerebral arteries, CA carotid artery. Single asterisk indicates left Heubner artery. Double asterisks indicate anterior comm. artery. Sagittal and coronal c,e preoperative and d,f postoperative MRI of the case; single asterisk indicates view of metyl metacrylate on MRI
In two cases with the tumor above 3 cm dimension and lateral extension, midline located part of the tumor was removed by internal debulking and capsular dissection. Anterior Comm–A1–A2 complex and perforating artery dissection was performed. However, firm tumor, which extended laterally and encased carotid artery–A1 complex could not be removed (Fig. 4).

a Intraoperative view of tumor removal by CUSA (Ultrasonic aspirator) and aspirator coronal b preoperative and c postoperative MRI of the case with Grade II tuberculum sellae meningioma; 59-year-old male (PN: 9). T tumor, RA1 right anterior cerebral artery (A1), LA1 and LA2 left anterior cerebral artery (A1, A2), As aspirator. Single asterisk indicates artery of Heubner. CUSA shows ultrasonic aspirator. Right arrowhead indicates right carotid artery ınvasion
In one case with Grade III lesion, even extracapsular dissection was attempted following internal debulking of the firm tumor and reaching to interpedincular cistern, we could not achieve total removal due to excessive adhesion of the tumor. In this case, we continued internal decompression by the time the tumor capsule became thinner and ended the operation (Fig. 5). After removal of meningioma surrounding structures were visualized and bleeding was controlled using surgicels. Also, these case examples are demonstrated by illustrated drawings (Fig. 6).

Axial and sagittal a,b preoperative and b,d postoperative MRI of the case with Grade III tuberculum sellae meningioma; 50-year-old female (PN: 5)

Illustrated drawing of tuberculum sella meningioma extension. TbS tuberculum sella, ON optic nerve, ICA ınternal carotid artery, M1 MCA M1, H artery of Heubner, AcoA anterior comm. artery, A1 and A2 anterior cerebral arteries. Dotted lines A indicates lateral vascular encasement, B indicates midline location, and C indicates optic nerve ınvasion
Reconstruction for all cases, autogenic fat inserted to residual cavity then duragen was applied in one case and in all cases autogenic fascia lata was laid inlay overflowing dural edges. Methyl methacrylate, which was prepared during the operation, was fixed on the defect.
Following defect closure, mucopericondrium of middle turbinate was laid onlay, fibrin glue was applied and 12F balloon inflated over the reconstructed area (Fig. 7). In all patients, lumbar drainage was performed intraoperative and removed on the postoperative fifth day for the first five patients and on the postoperative third day for the last four patients.

Multilayer closure for tuberculum sellae lesions. Duragen was inserted, and autogenic fascia lata was laid inlay overflowing dural edges. Metyl metacrylate was fixed on the defect. M metyl metacrylate
Results
In our clinical series, follow-up period varied from 3 months to 33 months (mean: 18 months; Table 1). Total removal was achieved in six of nine patients. Subtotal removal was performed for the patient with Grade III meningioma and the other two patients with Grade II lesions. An improvement of the preoperative visual deficits was observed in six of nine patients. No transient or permanent visual worsening was observed in any patients. Length of postoperative hospital stay varied from 6 to 8 days. CSF leakage was not seen in any of the patients. Permanent diabetes insipidus was seen in one patient.
Discussion
Different microsurgical surgical transcranial approaches and mostly pterional transsylvian route have been performed for the treatment of TSMs, and the results of techniques showed improvement gradually in morbidity and mortality rates [9].
Initial indications for transphenoidal technique only included the treatment of intrasellar lesions; however, it is now extended for supra and parasellar lesions [9, 11–14, 18–20, 23, 24].
Extended transphenoidal techniques including sublabial, transrhinoseptal, and direct endonasal variations via microsurgery, endoscopic endonasal, and endoscope-assisted microsurgery are presently being used [5, 6, 18, 20, 27, 28].
This technique has still challenges even though there is a possibility for performing endoscopic extended transphenoidal approach for tuberculum sellae meningioma.
These challenges can be classified according to the association between the lesions and the related neurovascular structures, endoscopic instrumentation management and control within the subarachnoid spaces, defect closure, and CSF leakage [9].
One of the criticisms of endoscopic extended approach for these lesions is the dissection trajectory located anterior to the neurovascular structures so blind accessing to the surgical area and increased risk of vascular injury. Especially, in cases with Grade III meningiomas and in Grade II meningiomas above 3 cm with vascular encasement and cisternal and lateral encasement, removal of the tumor through endoscopic transphenoidal route is difficult. But subtotal removal can be achieved in these cases. Sometimes inferior approach for Grade III lesions is more confident when compared with transcranial approaches due to similarity of selected operative route with tumor growing way. In these cases, one of the most important points is the nature of the tumor.
In the other Grade II and I cases, optic chiasm, anterior communicating artery complex dissection was performed, and the tumor was totally removed. Further extracapsular dissection may be possible with gaining experience in these cases.
Vascular and neural encasement evaluated preoperatively and nature of the tumor in Grade II and III cases are the most important factors affecting the efficiency of surgical procedure. Especially, removal of firm tumors is harder. General principles of microsurgical techniques should be also implemented for endoscopic approach. Endoneurosurgical dissection, which is defined by Kassam et al., can be achieved like in traditional transcranial dissection as the number of cases increase [20, 21]. Using ultrasonic aspirator at the beginning of tumor debulking gives a convenient dissection and allows the capsula to be mobilized. Meticulous endoneurosurgical technique should be used for the removal of the tumor from the usually preserved arachnoidal planes between the tumor and vascular structures.
Meningiomas originating from the tuberculum sellae commonly extend into the optic canal. Visual loss in an affected eye is the initial and most common symptom.
Especially lesions medially growing to the optic nerve can be better controlled by an inferior approach and extended endoscopic approach is a better way in controlling this route. de Divitiis et al. [10] defined the extension of the tumor inside the optic canal(s) as one of the contraindication for the transphenoidal approach. Wang et al. [31] defined the lateral limits to this exposure for tuberculum sella were the medial margins of the optic nerves as they entered the optic canal.
Inferior endoscopic approach may be a viable method accessing the inferomedial part of the optic nerve for the tumors located inferior to the optic nerve with optic canal invasion. In our experience, the endoscopic optic decompression was performed successfully in cases with pseudotumor cerebri and optic canal fractures due to trauma [25]. Also elevating the optic nerve on the affected side enables tumor removal on the posterior part of the nerve (Figs. 8 and 9).

Intraoperative view of meningioma extending into the optic nerve a before and b after opening the optic canal. Ultrasonic aspirator was used for posterior–inferior tumor removal by elevating the optic nerve (c,d). ON optic nerve, T tumor

Axial a preoperative and b postoperative MRI of the case with Grade I tuberculum sellae meningioma demonstrating the left optic nerve invasion; 32-year-old male (PN: 8)
One of the foremost drawbacks of this approach is to reconstruct the cranial base [22, 29, 30]. In the literature, CSF fistula was reported in the series of endoscopic approach for tuberculum sellae meningiomas. Six endoscopic transphenoidal approaches were reviewed for tuberculum sellae meningiomas. Jho et al. has published one case in 2001 and one case in 2004 followed by Laufer et al. with four cases in 2007, de Divitiis et al. with seven cases total in 2007 and 2008, Gardner and Kassam et al. with 13 cases in a series of anterior cranial base meningiomas in 2008, and Wang et al. with seven cases in 2009. In the last four of these series, common complication was CSF leakage. CSF fistula was reported by Laufer et al. 1/3 (33%), de Divitiis et al. 2/7 (28.5%), Gardner and Kassam et al. 8/13 (62%), and Wang et al. 1/7 (14.3%) in rates [6, 9, 10, 16, 18, 31].
Various techniques were used to reconstruct the cranial base such as “inlay” graft and vascularized fleb [22] or plugging with gelfoam or a graft of autologous abdominal fat that was held in place by a strut of the vomer [31].
Surgical approach itself in the nasal cavity should not destroy the normal nasal and paranasal anatomy unnecessarily. Tuberculum sellae is a superior region so there is no need to resect inferior part of posterior nasal septum such as vomer.
In our nine cases, reconstruction was performed with autogenic fascia lata inlay covering the dural edges. Methyl methacrylate was prepared on the same size with the defect intraoperative and fixed to prevent migration and stabilize the reconstructed area. Only in one case duragen was applied and autogenic lamellar bone was used. After applying fibrin glue, we inflated 12F balloon over the reconstructed area.
In our opinion, most important points in closing the defect are using autogenic fascia lata and to leave external lumbar drainage system fixed at the end of operation for at least 3 days. In our small number of cases, we did not see any CSF leakage after the operation and removal of lumbar drainage.
Most of the CSF leakages were treated applying lumbar drainage without the need of reoperation in our previous endoscopic approaches also in cases reported in the literature. We applied lumbar drainage in these nine cases intraoperative, initially for 5 days for the first five patients and 3 days for the last four cases. We did not see any CSF leakage after removal of the lumbar drainage. Improving reconstruction techniques may provide lumbar drainage duration to be decreased and to be omitted afterwards.
Via this approach, brain retraction is avoided, optic apparatus manipulation is minimized, and since direct visualization is possible, it is easy to overcome complete tumor removal with excision of the lesion dural attachment and involved bone, in other words, a Simpson Grade I removal [2]. In microscopic techniques, it is not possible to achieve Simpson Grade I removal every time.
To choose appropriate surgical technique, one must consider objectively the advantages and limitations of each technique and should take into account the surgical outcome, complication prevention, and own experience.
Conclusion
Limitations and nuances in extended endoscopic transphenoidal route for tuberculum sellae, meningioma can be brought under four groups.
-
1.
Tuberculum sellae meningiomas with dimensions above 3 cm located on the midline with optic chiasm and/or arterial encasement can be excised totally by endoneurosurgical technical dissection.
-
2.
Especially, TSMs demonstrating optic canal invasion and which are difficult to remove by transcranial route can be excised easier by endoscopic technique.
-
3.
Total removal of Grade III TSMs and Grade II tumors with lateral vascular encasement via endoscopic transphenoidal route is difficult.
-
4.
Nowadays, most important criticism of these approaches is CSF leakage. This complication may be overcome by applying inlay fascia lata, bone substitute, and onlay mucosa following external lumbar drainage for 3–5 days.
Although endoscopic extended transphenoidal approach for TS meningioma is still not a standardized procedure, it may be considered as a feasible alternative procedure in selected cases.
References
Arai H, Sato K, Okuda MM, Hishii M, Nakanishi H, Ishii H (2000) Transcranial transsphenoidal approach for tuberculum sellae meningiomas. Acta Neurochir (Wien) 142:751–757
Cappabianca P, Cavallo LM, Esposito F, De Divitiis O, Messina A, De Divitiis E (2008) Extended endoscopic endonasal approach to the midline skull base: the evolving role of transsphenoidal surgery.Adv Tech Stand Neurosurg 33:151–99, Review
Ceylan S, Koc K, Anik I (2009) Extended endoscopic approaches for midline skull-base lesions. Neurosurg Rev 32(3):309–19
Ceylan S, Koc K, Anik I (2010) Endoscopic endonasal transsphenoidal approach for pituitary adenomas invading the cavernous sinus. J Neurosurg 112(1):99–107, Erratum in: 112(1):210
Cook SW, Smith Z, Kelly DF (2004) Endonasal transsphenoidal removal of tuberculum sellae meningiomas: technical note. Neurosurgery 55:239–246
Couldwell WT, Weiss MH, Rabb C, Liu JK, Apfelbaum RI, Fukushima T (2004) Variations on the standard transsphenoidal approach to the sellar region, with emphasis on the extended approaches and parasellar approaches: surgical experience in 105 cases. Neurosurgery 55:539–550
de Divitiis E, Cappabianca P (2004) Endoscopic pituitary surgery: anatomy and surgery of the transsphenoidal approach to the sellar region. Endo-Press, Tuttlingen
de Divitiis E, Cavallo LM, Cappabianca P, Esposito F (2007) Extended endoscopic endonasal transsphenoidal approach for the removal of suprasellar tumors: Part 2. Neurosurgery 60(1):46–58
de Divitiis E, Cavallo LM, Esposito F, Stella L, Messina A (2008) Extended endoscopic transsphenoidal approach for tuberculum sellae meningiomas. Neurosurgery 62(6 Suppl 3):1192–1201
de Divitiis E, Esposito F, Cappabianca P, Cavallo LM, de Divitiis O (2008) Tuberculum sellae meningiomas: high route or low route? A series of 51 consecutive cases. Neurosurgery 62(3):556–563
Dusick JR, Esposito F, Kelly DF, Cohan P, DeSalles A, Becker DP, Martin NA (2005) The extended direct endonasal transsphenoidal approach for nonadenomatous suprasellar tumors. J Neurosurg 102:832–841
Dusick JR, Esposito F, Mattozo CA, Chaloner C, McArthur DL, Kelly DF (2006) Endonasal transsphenoidal surgery: the patient’s perspective-survey results from 259 patients. Surg Neurol 65:332–342
Fahlbusch R, Honegger J, Paulus W, Huk W, Buchfelder M (1999) Surgical treatment of craniopharyngioma: experience with 168 patients. J Neurosurg 90:237–250
Frank G, Pasquini E, Doglietto F, Mazzatenta D, Sciarretta V, Farneti G, Calbucci F (2006) The endoscopic extended transsphenoidal approach for craniopharyngiomas. Neurosurgery 59(1 Suppl 1):ONS75–ONS83
Frank G, Pasquini E, Mazzatenta D (2001) Extended transsphenoidal approach. J Neurosurg 95(5):917–918
Gardner PA, Kassam AB, Thomas A, Snyderman CH, Carrau RL, Mintz AH, Prevedello DM (2008) Endoscopic endonasal resection of anterior cranial base meningiomas. Neurosurgery 63(1):36–52
Goel A, Muzumdar D, Desai KI (2002) Tuberculum sellae meningioma: a report on management on the basis of a surgical experience with 70 patients. Neurosurgery 51:1358–1564
Jho HD, Ha HG (2004) Endoscopic endonasal skull base surgery: Part 1—The midline anterior fossa skull base. Minim Invasive Neurosurg 47:1–8
Kaptain GJ, Vincent DA, Sheehan JP, Laws ER Jr (2001) Transsphenoidal approaches for the extracapsular resection of midline suprasellar and anterior cranial base lesions. Neurosurgery 49:94–101
Kassam AB, Snyderman CH, Mintz A, Gardner P, Carrau RL (2005) Expanded endonasal approach: the rostrocaudal axis. Part I. Crista galli to the sella turcica. Neurosurg Focus 19(1):E3
Kassam AB, Snyderman CH, Mintz A, Gardner P, Carrau RL (2005) Expanded endonasal approach: the rostrocaudal axis. Part II. Posterior clinoids to the foramen magnum. Neurosurg Focus 19(1):E4
Kassam AB, Thomas A, Carrau RL, Snyderman CH, Vescan A, Prevedello D, Mintz A, Gardner P (2008) Endoscopic reconstruction of the cranial base using a pedicled nasoseptal flap. Neurosurgery 63(1 Suppl 1):ONS44–ONS52, discussion ONS52-3
Kim J, Choe I, Bak K, Kim C, Kim N, Jang Y (2000) Transsphenoidal supradiaphragmatic intradural approach: technical note. Minim Invasive Neurosurg 43:33–37
Kitano M, Taneda M (2001) Extended transsphenoidal approach with submucosal posterior ethmoidectomy for parasellar tumors. Technical note. J Neurosurg 94:999–1004
Koc K, Anik I, Altintas O, Ceylan S (2008) Endoscopic optic nerve decompression for idiopathic intracranial hypertension in two cases: case report. Minim Invasive Neurosurg 51(2):72–75
Koc K, Anik I, Ozdamar D, Cabuk B, Keskin G, Ceylan S (2006) The learning curve in endoscopic pituitary surgery and our experience. Neurosurg Rev 29(4):298–305, Erratum in (2007) Neurosurg Rev 30(1):96
Kouri JG, Chen MY, Watson JC, Oldfield EH (2000) Resection of suprasellar tumors by using a modified transsphenoidal approach. Report of four cases. J Neurosurg 92:1028–1035
Laufer I, Anand VK, Schwartz TH (2007) Endoscopic, endonasal extended transsphenoidal, transplanum transtuberculum approach for resection of suprasellar lesions. J Neurosurg 106:400–406
Oliver CL, Hackman TG, Carrau RL, Snyderman CH, Kassam AB, Prevedello DM, Gardner P (2008) Palatal flap modifications allow pedicled reconstruction of the skull base. Laryngoscope 118(12):2102–2106
Snyderman CH, Kassam AB, Carrau R, Mintz A (2007) Endoscopic reconstruction of cranial base defects following endonasal skull base surgery. Skull Base 17(1):73–78
Wang Q, Lu XJ, Li B, Ji WY, Chen KL (2009) Extended endoscopic endonasal transsphenoidal removal of tuberculum sellae meningiomas: a preliminary report. J Clin Neurosci 16(7):889–893
Acknowledgment
We thank to Assoc. Prof. Volkan Etus for the illustrated drawing.
Conflicts of ınterest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ceylan, S., Koc, K. & Anık, I. Extended endoscopic transphenoidal approach for tuberculum sellae meningiomas. Acta Neurochir 153, 1–9 (2011). https://doi.org/10.1007/s00701-010-0788-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-010-0788-1