
Abstract
Objective
The suboccipital lateral or retrosigmoid approach is the main neurosurgical approach to the cerebellopontine angle (CPA). It is mainly used in the treatment of CPA tumors and vascular decompression of cranial nerves. A prospective study using navigation registered with anatomical landmarks in order to identify the transverse and sigmoid sinuses junction (TSSJ) was carried out in a series of 30 retrosigmoid craniotomies. The goal of this study was to determine the accuracy of this navigation technique and to establish the relationship between the location of the asterion and the TSSJ.
Methods
From March through November 2008, 30 patients underwent a retrosigmoid craniotomy for removal of CPA tumors or for surgical treatment of neurovascular syndromes. Magnetic resonance imaging (MRI) T1 sequences with gadolinium (FSPGR with FatSst, 1.5 T GE® Signa) and frameless navigation (Vector vision®, Brainlab®) were used for surgical planning. Registration was performed using six anatomical landmarks. The position of the TSSJ indicated by navigation was the landmark to guide the craniotomy. The location of the asterion was compared with the position of the TSSJ. After craniotomy, the real TSSJ position was compared with the virtual position, as demonstrated by navigation.
Results
There were 19 cases of vestibular schwannomas, 5 petroclival meningiomas, 3 trigeminal neuralgias, 1 angioblastoma, 1 epidermoid cyst and 1 hemifacial spasm. In all cases, navigation enabled the location of the TSSJ and the emissary vein, with an accuracy flaw below 2 mm. The asterion was located directly over the TSSJ in only seven cases. One patient had a laceration of the sigmoid sinus during the craniotomy.
Conclusions
Navigation using anatomical landmarks for registration is a reliable method in the localization of the TSSJ for retrosigmoid craniotomies and thereby avoiding unnecessary sinus exposure. In addition, the method proved to be fast and accurate. The asterion was found to be a less accurate landmark for the localization of the TSSJ using navigation.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The suboccipital lateral or retrosigmoid approach is the most used neurosurgical approach for treatment of neurovascular compression syndromes and removal of vestibular schwannomas and other CPA tumors. Surface landmarks may be helpful to identify the transverse sigmoid sinus junction (TSSJ), whose location is indispensable for a successful suboccipital lateral approach. The junction of the lambdoid, occipitomastoid and parietomastoid sutures is the surface landmark called the asterion, and it is reported to lie over the TSSJ. Nonetheless, in only 60% of the cases is this precise relationship found [3, 6, 16]. The variation of asterion location may lead to potential sinus laceration during burr hole placement and mastoid drilling.
Image-guided navigation systems are widely used for surgical planning and intraoperative orientation. Several approaches to the posterior-lateral portion of the skull base involve exposure of the transverse and sigmoid sinuses [2]. The use of computer tomography (CT) navigation as a guiding tool for craniotomies in this region is useful to correctly drill the burr hole and thus avoid dural sinus laceration and venous bleeding [7–9]. We report a prospective study of 30 retrosigmoid craniotomies in which surgical planning using MRI navigation registered with anatomical landmarks was used to identify the transverse and sigmoid sinuses. The accuracy of this navigation technique and the relationship between the position of the asterion and the TSSJ were studied.
Material and methods
From March through November 2008, 30 patients underwent retrosigmoid craniotomies for removal of CPA tumors and surgical treatment of neurovascular conflicts as follows: 19 (63.3%) cases of vestibular schwannomas, 5 (16.7%) petroclival meningiomas, 3 (10%) trigeminal neuralgias, 1 (3.3%) epidermoid cyst, 1 (3.3%) angioblastoma and 1 (3.3%) hemi-facial spasm. Twenty-one patients were female, and the mean age was 58.3 years, range 21–74 years. For surgical planning, MRI scans using T1-weighted FSPGR (fast spoiled gradient-recalled echo) with FatSat gadolinium-enhanced 1.5-T sequences (MRI, 1.5-T GE® Signa) were performed. The images were uploaded onto a Brainlab® workstation with PatXfer® 5.2 software. The registration points, the transverse and sigmoid sinuses and object creation were captured with Brainlab iPlan® Cranial 2.6 software. Six skin surface anatomical landmarks were used for the navigation registration: nasion, anterior nasal spine, medial and lateral angles of the ipsilateral eye, ipsilateral tragus and ipsilateral ear helix (Fig. 1). In the object creation, the transverse and sigmoid were highlighted from the torcullae down to the jugular bulb ipsilaterally to the surgical site using axial, coronal and sagittal images (Fig. 2). The three-dimensional reconstructed object and its projection on the head were represented in the visualization mode (Fig. 3). All surgeries were performed in supine position with the ipsilateral shoulder and hip slightly elevated to allow easy rotation of the neck to the opposite side. Mayfield clamps were used in all cases, with the head positioned in such a way that the temporal squama would remain parallel to the floor. Special care to avoid occlusion of jugular venous outflow was taken. Intra-operative monitoring of the cranial nerves (VII, VIII and IX, X, XI) and brainstem-evoked potentials were carried out in all cases. A linear skin incision was placed 2 inches posterior to the ipsilateral mastoid tip, 1/3 above and 2/3 below the external auditory canal.

Six anatomical landmarks were used for navigation registration (indicated by arrows)

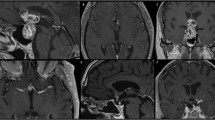
Object creation with right transverse and sigmoid sinuses

Three-dimensional reconstructed object (left) and its projection on the head (right). a Dural sinuses; b: TSSJ; c: skin incision
The navigation system used was the Brainlab® Vector Vision® Compact Image Guided Surgery System. The files were imported from the workstation to the navigator with a USB flash memory drive. The navigation system was registered with a pre-calibrated pointer using the six anatomical landmarks described above. After the skin incision and bone exposure, the virtual position of the TSSJ determined by the navigation was used as a landmark for the burr hole placement and craniotomy. The asterion position was compared with the virtual TSSJ position indicated by the navigation. When not coincidental, the distance between these two points (asterion and virtual TSSJ) was measured in millimeters using two coordinate axes (Fig. 4). The x axis was parallel and the y axis was perpendicular to the transverse sinus. The burr hole was placed about 1 cm medially and inferiorly from the virtual location of the TSSJ to avoid unnecessary sinus exposure. After craniotomy, the real position of the inferior margin of the TSSJ was identified and compared with the virtual location showed by the navigation (Fig. 5). The distance obtained (mm) between the position of the real TSSJ and the TSSJ position given by the navigation tool corresponded to the accuracy of the system. An accuracy within 2 mm or under was acceptable for a reliable navigation. In all cases, the same surgeon performed both the surgical planning and registration for the navigation tool.

Comparison between the asterion (a) and virtual TSSJ position indicated by navigation (b)

Comparison between virtual TSSJ location (left) and real TSSJ location (right) after craniotomy. TS: Transverse sinus; SS: sigmoid sinus
Results
An accurate localization of the real position of the TSSJ, as well as the mastoid emissary vein, was possible in all cases in this series. The comparison between the virtual and real position of the TSSJ had an accuracy flaw below 2 mm. The asterion was located directly over the TSSJ in 7 of the 30 cases. In our series, the asterion location varied from 13 mm medial to 15 mm inferior to the virtual position of the TSSJ (Table 1). In none of our cases was the asterion situated laterally or superiorly to the TSSJ. The average time spent with surgical planning on the workstation was 12 (range 8–20) min.
The location of the mastoid emissary vein was demonstrated by navigation in 24 cases. For instance, the emissary vein was absent in six cases, findings that were confirmed during surgery. Sigmoid sinus injury and emissary vein bleeding during craniotomy occurred in one case. The sigmoid sinus was repaired with polypropylene sutures, a muscle plug and biological glue. There were no other complications related to the retrosigmoid craniotomies in the present study. There were no cases of head shifting, reference star dislocation or registration loss during the procedures.
Discussion
The retrosigmoid craniotomy is the most used neurosurgical approach to gain acess to the cerebellopontine angle (CPA). It is usually performed to remove CPA tumors such as vestibular schwannomas, meningiomas, epidermoid cysts and others, and also in the treatment of neurovascular syndromes.
The retrosigmoid approach is limited by the position of the transverse (superiorly) and sigmoid sinuses (inferiorly). The correct burr hole placement for craniotomy has been extensively studied, being essential to avoid venous injury [1, 11, 17].
The asterion is located at the junction of the lambdoid, occipitomastoid and parietomastoid sutures and is commonly used as the main skull anatomical landmark for TSSJ localization. Day et al. [3] studied the asterion position in 100 dry human skulls and found its localization over the TSSJ in 61% of cases on the right side and 66% on the left side. Ribas et al. [16, 17] showed in a study of 50 dry human skulls that the asterion position over the TSJJ was accurate in 78% of cases; in 17% of the cases the asterion was below the TSSJ. Garabaghi et al. [8] demonstrated in 200 in vivo cases that the asterion was located over the TSSJ in 65% of cases on the right side and 75% of cases on the left side. In the present study, we found the asterion to lie directly over the TSJJ in only 23.3% of cases and directly over any point of the inferior margin of the transverse sinus in 63.3% of cases. In the present series virtual and in vivo parameters were compared.
The superior nucal line can also be used as a parameter to identify the inferior border of the transverse sinus, and the posterior edge of the mastoid process correlates well with the posterior margin of the sigmoid sinus [1, 11]. Illumination of mastoid air cells is also described as a technique employed to locate the venous sinuses in the retrosigmoid approach [19].
Neuronavigation has become a standard tool in intracranial and spinal procedures [18]. It minimizes surgical trauma through a more accurate definition of the target area. Localization of the venous sinuses, TSSJ and emissary vein is of utmost importance in the retrosigmoid approach to avoid damage to the venous structures of the region. Gharabaghi et al. [8] reported a systematic clinical study focused on image-guided retrosigmoid approaches with CT venography, with a 4% incidence of venous injury and 8% air embolisms in the image-guided group compared with a 15% incidence of venous injury and 19% air embolisms in the non-image-guided group. Hamasaki et al. [9] described 30 cases of image-guided retrosigmoid craniotomy based on CT surgical planning in order to avoid venous injury. In our series, a single case (3.33%) of venous sinus injury occurred with no morbidity. Although both authors demonstrated the importance of navigation in the retrosigmoid approaches, their registration method and navigation accuracy were not clearly presented. In the present study, the virtual position of TSSJ, indicated by the MRI navigation, determined the burr hole placement.
CT scan imaging is superior to MRI to study bone structures, but the T1 FSPGR with FatSat MRI sequence was effective in demonstrating the intracranial venous sinuses, which was helpful for the surgical planning [10, 14]. In our service, the surgical planning with CT scan images is complemented with MRI images to obtain optimal definition of intra- and extracranial structures. In the workstation, the venous sinuses are highlighted, and anatomical landmarks are used for registration.
Three types of registration methods for navigation are described in the literature [4, 5, 12, 13, 15]: (1) anatomical landmarks: uses anatomical points such as the nasion, eyes angles and tragus, (2) fiducials (adhesive or skull implanted): requires an image scan before surgery and (3) surface matching: consists of a laser registration of the patient's face. The accuracy among these methods differs according to the reports in the literature. Skull-implanted fiducials seems to be the gold standard with an accuracy flaw below 2 mm [13]. This method is invasive and adds extra time and extra costs.
Wolfsberger et al. [20] compared two registration methods and found an accuracy flaw of 2.9 mm with anatomical landmarks and 3.2 mm with adhesive fiducials. The nasion, the posterior wall of the external acoustic meatus, the medial and lateral eye angles were the anatomical landmarks used. Hill et al. [10] described 6 surgical cases using 6 to 12 anatomical landmarks for registration with CT, with a preference for points located close to the area of interest to avoid accuracy errors due to image distortion. Mascott et al. [13] described 30 surgical cases with CT navigation, comparing various registration methods. The bilateral tragus, bilateral medial eye angle and nasion were used as anatomical landmarks; the accuracy flaw was 5.4 mm. Adhesive fiducials had an accuracy flaw of 4.1 (with five adesive fiducials) and 3.9 (with ten adesive fiducials). Surfacing matching registration obtained an accuracy flaw of 4.4 to 4.9 mm. Skull implanted fiducials resulted in an accuracy flaw of 1.4 mm. With all registration methods an accuracy impairment was observed for deep structure localization. Pfisterer et al. [15] compared anatomical landmarks with adhesive fiducials and with surface matching registration in 30 surgical cases. He observed a similar efficacy with the three methods, with an accuracy flaw of about 3.5 mm. In our series, all 30 cases with anatomical landmarks registration had an accuracy flaw below 2.0 mm.
The option of anatomical landmark registration in our service is part of meticulous surgical planning before the operation, which, nonetheless, has not added extra surgery time. With adhesive fiducials, this delay is often unavoidable [15]. We perform surface matching registration in craniofacial or transnasal surgeries only. Anatomical landmarks registration is the fastest of the three methods and offers a simple and reliable navigation planning method in retrosigmoid craniotomy. This navigation planning method is operator-dependent, which significantly increases speed and safety in the retrosigmoid approach and decreases venous sinus injuries. An accuracy flaw below 2 mm in the identification of the TSSJ position demonstrated the reliability of MRI navigation registration using anatomical landmarks in all cases of our series. In our department, we also use intraoperative registration, with anatomical landmarks acquired after skull base and spine exposure for posterior fossa midline approaches.
Conclusion
MRI navigation using well-defined anatomical landmarks for registration as described in this paper is an easy, fast and safe method for the localization of TSSJ for retrosigmoid approaches. It also may improve the localization of craniotomy placement and may reduce injuries to the venous sinuses. Although useful for spatial orientation, the asterion is less accurate than navigation to localize the TSSJ.
References
Day JD, Fukushima T, Giannotta SL (1996) Innovations in surgical approach: lateral cranial base approaches. Clin Neurosurg 43:72–90
Day JD, Kellogg JX, Tschabitscher M, Fukushima T (1996) Surface and superficial surgical anatomy of the posterolateral cranial base: significance for surgical planning and approach. Neurosurgery 38:1079–1084
Day JD, Tschabitscher M (1998) Anatomic position of the asterion. Neurosurgery 42:198–199
Eggers G, Mühling J, Marmulla R (2006) Image-to-patient registration techniques in head surgery. Int J Oral Maxillofac Surg 35:1081–1095
Esquia-Medina G, Nguyen Y, Mazalaigue S, Vellin JF, Lombard B, Kalamarides M, Ferrary E, Sterkers O (2009) Use of anatomic or invasive markers in association with skin surface registration in image-guided surgery of the temporal bone. Acta Otolaryngol 19:1–6
Gharabaghi A, Rosahl SK, Feigl GC, Samii A, Liebig T, Heckl S, Mirzayan JM, Safavi-Abbasi S, Koerbel A, Löwenheim H, Nägele T, Shahidi R, Samii M, Tatagiba M (2008) Surgical planning for retrosigmoid craniotomies improved by 3D computed tomography venography. Eur J Surg Oncol 34:227–231
Gharabaghi A, Rosahl SK, Feigl GC, Liebig T, Mirzayan JM, Heckl S, Shahidi R, Tatagiba M, Samii M (2008) Image-guided lateral suboccipital approach: part 1-individualized landmarks for surgical planning. Neurosurgery 62:18–22 discussion 22–23
Gharabaghi A, Rosahl SK, Feigl GC, Safavi-Abbasi S, Mirzayan JM, Heckl S, Shahidi R, Tatagiba M, Samii M (2008) Image-guided lateral suboccipital approach: part 2-impact on complication rates and operation times. Neurosurgery 62:24–29 discussion 29
Hamasaki T, Morioka M, Nakamura H, Yano S, Hirai T, Kuratsu J (2009) A 3-dimensional computed tomographic procedure for planning retrosigmoid craniotomy. Neurosurgery 64:241–245 discussion 245–246
Hill DLG, Hawkes DJ, Crossman JE, Gleeson MJ, Cox TCS, Bracey EECML, Strong AJ, Graves P (1991) Registration of MR and CT images for skull base surgery using point-like anatomical features. Br J Radiol 64:1030–1035
Lang J Jr, Samii A (1991) Retrosigmoid approach to the posterior cranial fossa: an anatomical study. Acta Neurochir (Wien) 111:147–153
Marmulla R, Mühling J, Wirtz CR, Hassfeld S (2004) High-resolution laser surface scanning for patient registration in cranial computer-assisted surgery. Minim Invasive Neurosurg 47:72–78
Mascott CR, Sol JC, Bousquet P, Lagarrigue J, Lazorthes Y, Lauwers-Cances V (2006) Quantification of true in vivo (application) accuracy in cranial image-guided surgery: influence of mode of patient registration. Neurosurgery 59:146–156
Pérez AJ, Hernández LC, Ornia M, García Y (2006) The noninvasive study of cerebral veins and dural sinuses: comparison of two MR angiography techniques. Radiologia 48:87–98
Pfisterer WK, Papadopoulos S, Drumm DA, Smith K, Preul MC (2008) Fiducial versus nonfiducial neuronavigation registration assessment and considerations of accuracy. Neurosurgery 62:201–207 discussion 207–208
Ribas GC (1991) Study of the topographic relationship between the lambdoid, occipitomastoid and parietomastoid sutures and the transverse and sigmoid sinuses in trepanations in this areas. Dissertation, University of São Paulo, Brazil
Ribas GC, Rhoton AL Jr, Cruz OR, Peace D (2005) Suboccipital burr holes and craniectomies. Neurosurg Focus. PMID: 16122209
Roberts DW, Strohbehn JW, Hatch JF, Murray W, Kettenberger H (1986) A frameless stereotaxic integration of computerized tomographic imaging and the operating microscope. J Neurosurg 65:545–549
Tanaka Y, Kobayashi S, Unoki T, Nagashima H, Iwashita T (1995) Illumination of mastoid air cell for suboccipital craniotomy: technical note. Neurosurgery 36:1049–1051
Wolfsberger S, Rössler K, Regatschnig R, Ungersböck K (2002) Anatomical landmarks for image registration in frameless stereotactic neuronavigation. Neurosurg Rev 25:68–72
Disclosure
The authors do not have any further financial interest in the subject or materials under discussion.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
da Silva, E.B., Leal, A.G., Milano, J.B. et al. Image-guided surgical planning using anatomical landmarks in the retrosigmoid approach. Acta Neurochir 152, 905–910 (2010). https://doi.org/10.1007/s00701-009-0553-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-009-0553-5