
Abstract
Purpose
Cervical spondylodiscitis is a quite rare finding regarding the number and the common location of spinal abscesses in the lumbar region. While in thoracic and lumbar discitis, single-step surgery with neural decompression, disc space evacuation, and subsequent fusion is well known, there is no such report in cervical discitis. Here the authors present their experience with ventral polyetherketone (PEEK) cage fusion in cervical spondylodiscitis in a single-step procedure.
Methods
Between January 2006 and November 2008, five patients (three men, two woman; ages 71, 77, 58, 66 and 66 years) suffering from cervical spondylodiscitis and epidural abscess underwent disc evacuation, myelon decompression and subsequent ventral fusion using an empty PEEK cage disc replacement in one single setting. All five patients presented with significant neurological symptoms like cervicobrachialgia, tetraparesis and disturbance of the urinary incontinence. In all five patients, disc evacuation, myelon decompression and cervical fusion using a PEEK cage disc replacement in a single-stage surgery were performed. All wounds were closed primarily. Postoperatively, all patients received a specific antibiotic therapy for at least 6 weeks.
Results
This treatment strategy was successful in all patients with respect to clinical signs, laboratory parameters and radiological findings. All patients improved neurologically. Follow-up revealed a stable osteosynthesis without signs of instability. One cage was explanted despite neurological improvement and normal infectious parameters at another surgical department. No complications were observed.
Conclusions
In all, abscess drainage and ventral fusion with PEEK-cage disc replacement in one single setting was proven to be a successful treatment option in cervical discitis and spinal epidural abscess.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Cervical ventral fusion using a cage implant in the disc space is quite common. Currently it represents probably the most frequent technique to obtain anterior cervical fusion. Many different kinds of cage material are in use [2, 4, 14, 19]. Decompression of the myelon and subsequent ventral fusion with the implantation of cages are regarded as a safe and effective procedure in patients suffering from cervical disc disease [1, 2, 4, 5, 14, 19]. While reports of successful cage implantation in spondylodiscitis exist for the thoracolumbar spine [6, 7, 13], reports on polyetherketone (PEEK)-cage implantation in the primary treatment of cervical spondylodiscitis are missing.
In cervical spondylodiscitis, it depends on the location of the abscess and, even more importantly, on the involvement of the disc space if a ventral discectomy has to be performed [8, 10–12, 17, 18]. Surprisingly with the widespread use of PEEK-cage implants, no data have been reported on ventral fusion using a PEEK cage after ventral discectomy for discitis in only one setting.
Here, the authors present their series of five cervical ventral fusions using a PEEK cage after evacuation of the disc space and drainage of epidural abscess in cervical spondylodiscitis as a single-stage surgery.
Materials and methods
Study design
For the past 5 years, ventral fusion using a PEEK cage disc spacer after ventral discectomy has been the established technique in the authors’ departments. Out of the data base of more than 300 ventral cervical fusions using a PEEK cage since March 2003, five patients underwent this procedure after evacuation of cervical spondylodiscitis and drainage of spinal epidural abscess in one setting. All cases were followed prospectively.
Surgical technique for ventral fusion
The standard surgical technique via an anterolateral approach and right-sided skin incision, which was described by Smith and Robinson [16], was applied. The disc of the pathological level was microsurgically evacuated with a high-speed drill and bone curettes. After resection of the disc, the posterior ligament was opened and the epidural abscess drained. After careful irrigation, PEEK cage implantation (Cornerstone, Medtronic) was performed. The PEEK cage is a hollow frame with retentive teeth on the top and bottom [2] which improve the fixation of the cage to the bone. The cages were not filled with bone or other material. Then a radiological control of cage position followed. In one case, an antibiotic chain was put in the wound. After insertion of a drain for wound secretion, the wound was closed primarily.
Results
Five patients underwent ventral discectomy, abscess drainage and decompression of the myelon for cervical spondylodiscitis and epidural abscess. In all cases, surgery was performed in an emergency setting because of significant neurological symptoms and infectious signs. After decompression, an empty PEEK cage was inserted into the disc space. The cages consisted of 12 mm width and 14 mm depth. No antibiotic irrigation was performed. The wound was closed primarily. All patients were put on intravenous antibiotic therapy. Microbiology revealed Staphylococcus aureus in all cases. All patients recovered rapidly and without complications. After discharge to a rehabilitation centre, one patient was transferred to another surgical department at 5 weeks after initial surgery. There it was felt that implantation of a foreign body (PEEK cage) was inadequate despite persistent improvement of neurological symptoms and normal infectious parameters. The cage was explanted and a bone graft inserted. All the other patients progressed uneventfully, without complications. Details of the five patients are given in Table 1. Figures 1 and 2 show the radiological course of two exemplary patients.

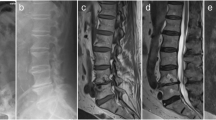
Case illustration 1: (a) T2-weighted and (b) T1-weighted sagittal MR images demonstrating C5/6 spondylodiscitis and epidural abscess formation compressing the cervical myelon. c T1-weighted axial MR image with gadolinium showing right lateral epidural abscess with myelon compression. d Postoperative sagittal X-ray image with PEEK cage in correct space. e Postoperative MR image 9 days after surgery with decompressed myelon, evacuated disc space, PEEK cage in correct position and residual epidural abscess (T1-weighted sagittal scan with gadolinium). f Postoperative MR image 9 months after surgery. There is no evidence of epidural abscess, optimal postoperative result (T1-weighted sagittal scan with gadolinium)

Case illustration 2: (a) T1-weighted sagittal MR image with gadolinium demonstrating spondylodiscitis at C6/7, epidural abscess from C5/6 to Th1/2 level, and retropharyngeal abscess formation. b T1-weighted gadolinium-enhanced axial MR image showing epidural abscess with myelon compression at C6/7 level. c, d Postoperative MR image with decompressed myelon, evacuated disc space, and implanted PEEK cage at C6/7 and C7/Th1 at 16 months after surgery (c T2-weighted sagittal image,d T1-weighted sagittal image)
Discussion
Ventral fusion of the cervical spine in patients with cervical disc disease using a PEEK cage is, nowadays, a very common operative technique. The PEEK cage provides a solid fusion and an increased cervical lordosis [4]. The complication rate is very low; and the functional and neurological outcomes are good [1, 4]. Spinal epidural abscess comprises 0.2–2 cases per 10,000 hospital admissions [12]. Most cases of spinal epidural abscess occur in patients aged 30–60 years, and the most common risk factors are diabetes mellitus, trauma, intravenous drug abuse and alcoholism [12]. Reports on PEEK cage implantation in active purulent cervical discitis are missing. The use of anterior implants and non-allogenic material in the presence of a severe infection presents a challenge for spine surgery. Various studies exist which report the surgical results in patients with pyogenic spinal infections with abscess drainage and debridement and delayed ventral fusion [7]. In the literature, most authors described an anterior surgery with fusion and cage implantation in active infections concerning the thoracolumbar spine [6, 7, 13]. Korovessis et al. [6] reported 14 patients with thoracolumbar spondylitis who were treated with anterior surgery with the insertion of a titanium mesh cage and a posterior instrumented fusion performed in one setting. They had only one anterior wound abscess and hence showed that the presence of titanium mesh cages had no negative influence on wound healing. Even the sagittal profile of the spinal column could be retained. Ruf et al. [13] investigated 88 cases with active vertebral osteomyelitis, and 13 cases had a cervical location. All had a ventral fusion using titanium mesh cages. All patients showed a solid bony fusion without any recurrence of infection, and they found a restored sagittal profile. Kuklo et al. [7] reviewed 21 patients with a pyogenic vertebral osteomyelitis, but they had no cervical location. All patients were treated with titanium mesh cages after debridement in only one setting; they received a resolution of infection in every case.
Ventral fusion using a PEEK cage in an active cervical spinal abscess after drainage and debridement has not been reported. However, several case reports and studies exist concerning treatment strategies in cervical spinal epidural abscesses. Boström et al. [3] found instrumentation with primary fixation not mandatory, but it should be discussed on an individual basis. Matsuda et al. [9] reported one case of an acute cervical epidural abscess where an anterior spinal decompression surgery was performed; the patient underwent reconstruction stabilization surgery 3 weeks after the first operation. To perform more than one operation seems to be a common treatment option in cases with cervical epidural abscess. The reason why it is not usual to do ventral instrumentation using a cage after abscess drainage and debridement in cervical spinal epidural abscess under the status of only one general anaesthesia seems to be obvious. It is not recommended to put a foreign material into an infected wound. Various authors favoured against the use of foreign material because of the glycocalyx formation on the non-allogenic material which could be the reason for a chronic infection [7]. However, in the present report, all five patients were treated successfully by emergency decompression, PEEK cage implantation and postoperative antibiotic treatment with complications. In all patients, the neurological symptoms improved; all parameters of infection decreased to normal. In every patient, a postoperative magnetic resonance imaging (MRI) showed a well decompressed myelon and a sufficient position of the PEEK cage with a restored sagittal profile. The present five patients did not receive any bone grafting at the authors’ department not even within the cages. The authors think that the use of small bone pieces rather increases the risk of an infection since this material is bradytroph and has a large surface area. However, no data on this subject are available. Thus, no conclusions can be drawn. Also, the bony fusion rate after this treatment strategy cannot be addressed accurately since all patients only received MR studies at the follow up appointments. All the authors can say is that there was a stable osteosynthesis on the MR images of all patients.
In all, it seems that a ventral fusion using a PEEK cage after spondylodiscitis and abscess drainage in only one surgery could represent a valuable treatment option. Although the conservative treatment of spinal discitis remains the therapy of first choice as soon as the decision for surgery mainly based on the neurological status is made, empty PEEK cage implantation is possible [15]. However, long-term specific antibiotic therapy appears to be mandatory. The report gains even more importance since the surgical revision by a foreign surgical team of one patient just because the PEEK cage implantation was considered to be inadequate treatment for cervical discitis shows that there is a vivid controversy on the optimal treatment of cervical discitis cases.
References
Assietti R, Beretta F, Arienta C (2002) Two-level anterior cervical discectomy and cage-assisted fusion without plates. Neurosurg Focus 12:E3
Bärlocher CB, Barth A, Krauss JK, Binggeli R, Seiler RW (2002) Comparative evaluation of microdiscectomy only, autograft fusion, polymehtylmethacrylate interposition, and threaded titanium cage fusion for treatment of single-level cervical disc disease: a prospective randomized study in 125 patients. Neurosurg Focus 12:E4
Boström A, Oertel M, Ryang Y, Rohde V, Bürgel U, Krings T, Korinth M (2008) Treatment strategies and outcome in patients with non-tuberculous spinal epidural abscess—a review of 46 cases. Minim Invasive Neurosurg 51:36–42
Cho DY, Liau WR, Lee WY, Liu JT, Chiu CL, Sheu PC (2002) Preliminary experience using a polyetherketone (PEEK) cage in the treatment of cervical disc disease. Neurosurgery 51:1343–1349
Kandziora F, Pflugmacher R, Schaefer J, Scholz M, Ludwig K, Schleicher P, Haas NP (2003) Biomechanical comparison of expandable cages for vertebral body replacement in the cervical spine. J Neurosurg Spine 99:91–97
Korovessis P, Petsinis G, Koureas G, Iliopoulos P, Zacharatos S (2006) Anterior surgery with insertion of titanium mesh cage and posterior instrumented fusion performed sequentially on the same day under one anesthesia for septic spondylitis of thoracolumbar spine: is the use of titanium mesh cages safe? Spine 31:1014–1019
Kuklo TR, Potter BK, Bell RS, Moquin RR, Rosner MK (2006) Single-stage treatment of spinal infection with titanium mesh cages. J Spinal Disord Tech 19:376–382
Liou LM, Shih PY (2007) Epidural abscess of the cervical spine with atypical manifestations: a report of two cases. Neurologist 13:215–218
Matsuda R, Nakase H, Park YS, Sakaki T (2005) A case of acute cervical epidural abscess. No To Shinkei 57:1089–1093
Murphy DR, Morris NJ (2006) Cervical epidural abscess in an afebrile patient: a case report. J Manipulative Physiol Ther 29:672–675
Nussbaum ES, Rigamonti D, Standiford H, Numaguchi Y, Wolf AL, Robinson WL (1992) Spinal epidural abscess: a report of 40 cases and review. Surg Neurol 38:225–231
Reihsaus E, Waldbaur H, Seeling W (2000) Spinal epidural abscess: a meta-analysis of 915 patients. Neurosurg Rev 23:175–204
Ruf M, Stoltze D, Merk HR, Ames M, Harms J (2007) Treatment of vertebral osteomyelits by radical debridement and stabilization using titanium mesh cage. Spine 32:E275–E280
Salame K, Ouaknine GER, Razon N, Rochkind S (2002) The use of carbon fiber cages in anterior cervical interbody fusion. Neurosurg Focus 12:E1
Schils F, Rilliet B, Payer M (2006) implantation of an empty carbon fiber cage or a tricortical illiac crest autograft after cervical discectomy for single-level disc herniation: a prospective comparative study. J Neurosurg Spine 4:292–299
Smith GW, Robinson RA (1958) The treatment of certain cervical spine disorders by anterior removal of the intervertebral disc and interbody fusion. J Bone Joint Surg Am 40A:607–623
Soehle M, Wallenfang T (2002) Spinal epidural abscesses: clinical manifestations, prognostic factors, and outcomes. Neurosurgery 51:79–85
Tang HJ, Lin HJ, Liu YC, Li CM (2002) Spinal epidural abscess-experience with 46 patients and evaluation of prognostic factors. J Infect 45:76–81
Zevgaridis D, Thomé C, Krauss JK (2002) Prospective controlled study of rectangular titanium cage fusion compared with iliac crest autograft fusion in anterior cervical discectomy. Neurosurg Focus 12:E2
Author information
Authors and Affiliations
Corresponding author
Additional information
Comment
This is a collection of four patients with cervical discitis who underwent fusion with a PEEK cage at the time of surgical debridement. Although the sample size is small, and the incidence of cervical discitis is uncommon but not rare, the paper raises an important discussion point.
The authors suggest that adding a cage to a single-stage procedure is safe and does not increase the risk of recurrent infection, which is known already for infections of the thoracic and lumbar spine. It is interesting that the authors did not put any bone graft in the cage. It is not clear whether use of bone graft increases infection rates.
David Choi
London, UK
Rights and permissions
About this article
Cite this article
Mondorf, Y., Gaab, M.R. & Oertel, J.M.K. PEEK cage cervical ventral fusion in spondylodiscitis. Acta Neurochir 151, 1537–1541 (2009). https://doi.org/10.1007/s00701-009-0486-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-009-0486-z