
Abstract
Purpose
A case of tuberculosis is reported in which there was extensive unilateral destruction of the bones of the craniovertebral junction. A lateral facetal subluxation of the relatively well-preserved contralateral atlantoaxial joint was identified. The patient was treated with unilateral fixation of the subluxated joint using a lateral mass plate and screw method of fixation. The pathogenesis of facetal subluxation and the rationale of the treatment adopted are discussed.
Case report
A 63-year-old male patient had systemic tuberculosis and had been on drug treatment for 5 months. For about 1 month, he had experienced severe neck pain and progressive quadriparesis. Investigations revealed extensive unilateral destruction of the lateral masses of atlas and axis and occipital condyle. MRI showed altered cord signal at the level of the craniovertebral junction. CT scan showed contralateral lateral subluxation of the facet of atlas over the facet of axis. Unilateral fixation and distraction of the lateral mass of atlas and axis, external orthosis and antituberculous drug treatment resulted in rapid and sustained neurological recovery.
Conclusion
Contralateral atlantoaxial facetal subluxation can be a result of osteoligamentous incompetence in cases of tuberculosis where there is unilateral facetal destruction. A coronal CT scan view can be diagnostic in such cases. Atlantoaxial lateral mass fixation can be a rational form of surgical treatment in such cases.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Osteoligamentous destruction and deformities leading to a range of clinical presenting symptoms have been recorded in cases with tuberculosis involving the craniovertebral junction [1, 9–13]. Our analysis and review of the literature on the subject suggest that infective lesions in general and tuberculosis in particular involving the craniovertebral junction usually start unilaterally from the cancellous part of the lateral mass of the atlas or axis [7]. The disease then progresses to involve the atlantoaxial joint by destructive necrosis and inflammation. The extent and nature of involvement of the joints are determining factors for the need for any kind of surgery for stabilization of the region. Due to the intact normal presence of the contralateral atlantoaxial joint in the early stages of the disease, and absence of demonstrable instability, surgery for fixation is generally not advocated, and reliance is laid on external cervical immobilization and anti-tuberculous drug treatment. We report the management of a case in which the patient had extensive tuberculous unilateral involvement of the facets of atlas and axis and occipital condyle of craniovertebral junction that resulted in lateral dislocation of the facet of atlas over the facet of axis on the contralateral side. Lateral atlantoaxial facetal subluxation has been described in cases with rheumatoid arthritis [2], but has not been previously noted in patients with craniovertebral junction tuberculosis.
Case report
A 63-year-old male, not a known diabetic and not immunocompromised, had multiple large and matted cervical lymph nodes for about 5 months. The infection resulted in multiple sinuses that drained pus over the skin of the neck. Investigations confirmed that the lesions were tuberculous in nature, and, accordingly, drugs were started. Following the drug treatment, some of the sinuses healed and the cervical lymphadenitis resolved. Although the patient had experienced pain in the neck for several months, he and the physicians related it to cervical lymph node infection. Accordingly, the craniovertebral junction was not radiologically assessed, and no external orthosis was applied; he was not subjected to a bed-rest protocol. Under the circumstances, it was unclear if the anti-tuberculous drug treatment had failed or if non-restraint of the region resulted in worsening of craniovertebral junction disease. For about 1 month, the pain in the neck was exacerbated, and he had progressive weakness of all four limbs. The weakness was more pronounced on the right side. He also had moderate torticollis towards the normal (left) side. In the period of 10 days, his condition worsened to the extent that he was bed-ridden and could not perform useful activity with any of his limbs. He had to be fed and clothed. For urinary retention, he had to be catheterized. He needed an enema for stool evacuation.
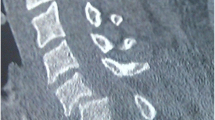
Investigations revealed extensive destruction of the facets of atlas and axis and occipital condyle on the right side (Fig. 1). Additionally, there was destruction of a part of the anterior and posterior arch of atlas and odontoid process of the axis. Adjoining the region of bone destruction, there was granulomatous soft tissue swelling. MRI showed altered cord signal intensity at the level of the craniovertebral junction; however, no evidence of direct neural compression by bone or soft tissue was evident (Fig. 1d). There was ‘fixed’ atlantoaxial dislocation, and the dynamic flexion-extension plain radiology did not show any clear evidence of abnormal mobility in the region and of the odontoid process in relationship with the anterior arch of the atlas. A CT scan showed evidence of lateral dislocation of the left-side facet of atlas over the facet of axis (Fig. 1a–c). The atlantoaxial joint space had collapsed. On this side, the occipitoatlantal joints and the sub-axial joints were preserved. The investigations and measurements by classically described parameters showed that the patient had mild basilar impression (Fig. 1a). It was concluded that the lateral dislocation of the facet of atlas over the facet of axis was a result of incompetence of the ligamentous assembly, and more importantly the alar and transverse ligaments due to destruction of the atlas facet on the contralateral side. Considering the rapid progression of the neurological worsening, surgery for stabilization of the region was contemplated. The surgical steps used were as discussed in our papers on the subject [3–6]. The left-sided atlantoaxial joint was exposed. The articular cartilage was denuded, and bone graft pieces harvested from the iliac crest were stuffed into the joint space. Additionally, a titanium spacer measuring 3 mm in height, 11 mm in length and 8 mm in width was impacted in the joint space after its distraction. Lateral mass plate and screw fixation of the atlantoaxial joint was subsequently done [3, 4]. Bone graft pieces were also placed over the midline in the region of the arch of atlas, over the lamina and spinous process of the axis, after appropriately preparing the bed. The region of the lateral masses on the disease-affected side was not manipulated as the location and course of the vertebral artery were unclear due to the marked bone destruction. There was no evidence of purulent granulations on this side. Postoperatively, the patient was placed in a four poster cervical collar, and all movements related to the neck were restricted for a period of 3 months. Investigations done at a 6-month follow-up showed reduction of the lateral dislocation and of basilar impression. The plate and screw fixation and distraction of the atlantoaxial joint by the spacer and bone graft could be observed (Fig. 2). There was evidence of bone fusion and no clinical or radiological evidence of instability. Extensive osteo-ligamentous fibrosis on the diseased side probably further contributed to the stability of the region. Postoperative coronal images showed evidence of osteo-ligamentous healing (Fig. 2b).

a CT scan shows borderline basilar impression (when measured by Chamberlain’s line and Wackenheim’s clival line), ‘fixed’ atlantoaxial dislocation and evidence of destruction of the odontoid process. The tracing of the spinolaminar line to the foramen magnum shows marginal anterior displacement of the posterior arch of the atlas. b Sagittal view of the scan showing destruction of the lateral mass of the atlas and axis. c Coronal view of the CT scan shows lateral dislocation of the facet of atlas over the facet of axis. On the diseased side occipito-atlantoaxial erosion is evident. d T2-weighted MRI shows evidence of cord changes at the level of the foramen magnum

a Postoperative CT scan shows reduction of atlantoaxial dislocation and of basilar impression. b Coronal image shows spacer within the distracted atlantoaxial joint. Screws can be seen within the facets of atlas and axis. Evidence of osteoligamentous healing is observed on the diseased side. c Lateral X-ray shows unilateral fixation of atlantoaxial joint with plate and screws and spacer
The patient improved remarkably in his clinical symptoms immediately following surgery. He was additionally placed on a second line of anti-tuberculous drugs for a total period of 18 months. At a follow-up after 33 months, he walked independently and could carry out his routine household activities unaided. There was no neck or spinal tilt.
Discussion
Advancements in the computer-based radiological investigations have improved the understanding of tuberculosis of the craniovertebral junction. Our analysis and review of the literature suggest that tuberculous infection more frequently starts unilaterally by involving the cancellous part of the facet of atlas [7]. Less frequently, the cancellous portion of the facet of axis and of the odontoid process is the site of the beginning of disease. The joint involvement is a result of extension of the inflammatory reaction. The incompetence of the joint and osseous and the adjoining ligamentous destruction in such a situation have been known to result in subluxation of the atlanto-axial facets. However, due to the presence of a normal atlantoaxial joint on the contralateral side, the region is not alarmingly unstable, and the patient generally presents with symptoms of pain and torticollis. Neurological deficits are notably delayed and less pronounced despite the aggressive destruction by the disease. Due to the presence of a relatively stable craniovertebral region, despite the unilateral facetal destruction and the effectiveness of the modern anti-tuberculous drugs, surgery for fixation is not universally recommended in such cases [8].
In the presented case, the patient developed tuberculous affection of the craniovertebral region when he was already on anti-tuberculous drugs. As he was not on any physical neck restraint, it is unclear if the drug treatment failed or not. He had rapid progression of neurological worsening, despite the fact that no definite abnormal mobility was observed on dynamic radiological imaging of the craniovertebral junction. The exact mode of involvement of the cord is unclear. However, it appeared from the radiological assessment that the lateral dislocation of the contralateral facet of atlas over the facet of axis and collapse of the atlantoaxial joint space height and reduced height of the spine in the region probably resulted in kinking of the cord. Abnormal mobility (especially rotational) between the atlas and axis causing recurrent cord trauma can be the possible cause of neurological worsening. Although granulation tissue and abscess can also result in cord compression in cases with tuberculous infection, such a feature was not clearly evident on imaging.
In the presence of destruction of the facets of atlas and axis on one side, it appeared that the alar and transverse ligaments became unilaterally incompetent. The shift of balance on the contralateral side and the obliquity of the inclination of the facet of atlas in the atlantoaxial joint probably resulted in its lateral subluxation over the facet of axis. During surgery, the region appeared moderately unstable. Our patient recovered remarkably following surgery that involved distraction of the facets of atlas and axis, restoration of the height of the atlantoaxial spine and their fixation. The improvement in the patient’s condition may also be related to neck immobilization with an internal fixation and external arthrosis in addition to anti-tuberculous drugs. Although fixation was done only on one side, the lateral mass C1-2 plate and screw fixation procedure, jamming the joint movements and distraction of the facets provided a stable fixation and ground for bone fusion [3–6]. However, the need for inclusion of the occipital bone in the fixation procedure remains questionable. This is particularly so in light of the fact that the occipital condyle and occipito-atlantal lateral joints appeared involved by the destructive disease process.
We conclude from our experience in the presented case that lateral subluxation of the atlas over axis secondary to osteoligamentous incompetence can be a defined and treatable pathological entity.
References
Behari S, Nayak S, Bhargava V, Banerji D, Chabbra D, Jain V (2003) Craniocervical tuberculosis: protocol of surgical management. Neurosurgery 52:72–81
Burry H, Tweed J, Robinson R, Howes R (1978) Lateral subluxation of the atlanto-axial joint in rheumatoid arthritis. Ann Rheum Dis 37:525–528
Goel A, Desai K, Muzumdar D (2002) Atlantoaxial fixation using plate and screw method: a report of 160 treated patients. Neurosurgery 51:1351–1357
Goel A, Laheri VK (1994) Plate and screw fixation for atlanto-axial dislocation. (Technical report). Acta Neurochir (Wien) 129:47–53
Goel A (2004) Treatment of basilar invagination by atlantoaxial joint distraction and direct lateral mass fixation. J Neurosurg Spine 1(3):281–286
Goel A (2007) Atlantoaxial joint jamming as a treatment for atlantoaxial dislocation: a preliminary report. Technical note. J Neurosurg Spine 7(1):90–94
Goel A, Shah A (2009) Treatment of Craniovertebral junction tuberculosis. In: Goel A (ed) Surgery of the craniovertebral junction. Principles and practice. Thieme Publications, Germany In press)
Gupta S, Mohindra S, Sharma B, Gupta R, Chhabra R, Mukherjee K, Tewari M, Pathak A, Khandelwal N, Narain S, Khosla V (2006) Tuberculosis of the craniovertebral junction: is surgery necessary? Neurosurgery 58:1144–1149
Kanaan IU, Ellis M, Safi T, Al Kawi MZ, Coates R (1999) Craniocervical junction tuberculosis: a rare but dangerous disease. Surg Neurol 51:21–26
Lee DK, Cho K, Im S, Hong S (2007) Craniovertebral junction tuberculosis with atlantoaxial dislocation: a case report and review of literature. J Korean Neurosurg 42:406–409
Shukla D, Mongia S, Devi I, Chandramouli BA, Das BS (2005) Management of craniovertebral junction tuberculosis. Surg Neurol 63:101–106
Sinha S, Singh A, Gupta V, Singh D, Takayasu M, Yoshida J (2003) Surgical management and outcome of tuberculous atlantoaxial dislocation: a 15-year experience. Neurosurgery 52:331–339
Teegala R, Kumar P, Kale S, Sharma B (2008) Craniovertebral junction tuberculosis: a new comprehensive therapeutic strategy. Neurosurgery 63:946–955
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Goel, A., Shah, A. Lateral atlantoaxial facetal dislocation in craniovertebral region tuberculosis: report of a case and analysis of an alternative treatment. Acta Neurochir 152, 709–712 (2010). https://doi.org/10.1007/s00701-009-0467-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-009-0467-2