
Abstract
Background
Evolving of a single centre by means of different transsphenoidal approaches during the survey of methodological advances in pituitary surgery is presented.
Materials and methods
Ninety-three consecutive patients with pituitary adenomas underwent transphenoidal pituitary operations at Gulhane Military Medical Academy from January 1996 to October 2007. Retrospective chart-based analysis of the surgical methods of transsphenoidal pituitary adenoma operations were done. Surgical methods were described. Outcomes and complications were presented. Attention is focused on the methodology of different surgical techniques of pituitary surgery.
Findings
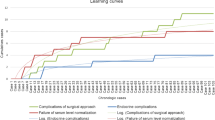
During the evaluation period, 12 Sublabial approaches (1996–1998), 13 transseptal transsphenoidal approaches (1999–2000), 15 endonasal transsphenoidal approaches (2000–2004), 25 endoscopy assisted endonasal approaches (2002–2006) and 28 pure endoscopic endonasal approaches (2006–2007) were performed.
Conclusions
Technologic advancements in endoscopy and gaining experience in pituitary surgery drives neurosurgeons toward less invasive approaches.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The surgical treatment of pituitary tumours has been improved by a number of recent technical advances. Pituitary tumours can now be visualized more accurately due to continued improvements in magnetic resonance imaging (MRI) techniques with gadolinium enhancement. Various techniques in the surgical treatment of pituitary adenomas have been described to date. Sir Victor Horsley performed the first surgical resection of pituitary adenoma in 1889 via a transcranial approach. Herman Schloffer performed the first successful transsphenoidal resection of a pituitary tumour via a transfacial approach [18]. Since the initial transsphenoidal approach performed in Austria by Schloffer, the transsphenoidal approach has become the preferred surgical approach to most pituitary tumours [15]. More recently, transitional steps are taking place among neurosurgeons from traditional microscopic transsphenoidal surgery to endoscopic endonasal pituitary surgery [2, 3, 9–11].
This short review is focused on evolving of transsphenoidal surgery in a single centre. We also aimed to present our experience during the survey of transition from sublabial approach to endoscopic pituitary surgery, problems and our solutions for different surgical techniques.
Methods and materials
Retrospective chart-based analysis of the surgical methods, indications and outcomes of pituitary adenoma patients were done. Transcranial operations for pituitary adenomas were excluded. Eighty one of operations were done by Professor Engin Gonul. Outcomes and complications of transsphenoidal operations were presented. Pituitary adenomas were classified by size on magnetic resonance imaging, computed tomography or intraoperative findings: tumour size of <1 cm was defined as micro-adenoma, 1 and <2 cm as macro-adenoma, and >2 cm as giant-adenoma. Invasiveness was evaluated as invasive to supradiaphragmatic space, invasive to cavernous sinus and invasive to sphenoid sinus on magnetic resonance imaging and intraoperative findings.
Results
Patient and follow-up characteristics
The study included 36 (38.7%) female and 57 (61.3%) male patients. The mean age was 38.5 ± 14.8 years (range, 19–81 year) and mean postoperative follow-up period of 28 ± 22 months (median = 24 months)
Documentation of surgical techniques:
Ninety-three consecutive patients with pituitary adenomas underwent transphenoidal pituitary operations at Gulhane Military Medical Academy from January 1996 to October 2007. In addition to the primary transsphenoidal operations, eleven transsphenoidal cerebrospinal fluid leak (CSF) repair operations were performed on these cases.
Transphenoidal pituitary operations were included sublabial transgingival, transseptal transsphenoidal, endonasal transsphenoidal, endoscopy assisted endonasal transsphenoidal and purely endoscopic endonasal transsphenoidal operations. The sublabial approach is directed under the lip and submucosally along the nasal septum to the sphenoid sinus. The transseptal approach avoids the oral cavity and is directed through a small incision along one side of the columella and submucosally along the septum. The endonasal approach is directed through one nostril, between the concha laterally and the nasal septum medially, and does not require an incision in the nose before reaching the anterior face of the sphenoid. The endoscopy assisted endonasal transsphenoidal approach was done through one nostril with the aid of microscope and endoscope. Nasal speculum was used to facilitate the operation in all approaches except pure endoscopic endonasal approaches.
During the evaluation period, 12 Sublabial approaches (1996–1998), 13 transseptal transsphenoidal approaches (1999–2000), 15 endonasal transsphenoidal approaches (2000–2004), 25 endoscopy assisted endonasal approaches (2002–2006) and 28 pure endoscopic endonasal approaches (2006–2007) were performed (Table 1). Our first endoscopic experience was in 2002. We have started to use the endoscopy to explore the operative field at first operations. After gaining experience with 25 patients we have decided to make pure endoscopic endonasal operations starting from 2006. In order to show the progression in experience in pituitary surgery, documentation of different surgical techniques which were performed at GATA is presented in Table 1.
Tumour characteristics:
Eighteen (19.3%) patients had microadenoma (<1 cm). 58 (62.3%) patients had macroadenoma (>1 cm). 22 (37.9%) out of 58 macroadenoma was giant macroadenoma (>2 cm). Sixty-four (68.8%) were invasive adenomas. Twenty-five (26.8%) adenomas were invasive to supradiaphragmatic space through diaphragma sella. Fifty-four (58%) adenomas were invasive into the cavernous sinus. Thirteen (13.9%) adenomas were invasive to the sphenoid floor.
Resection degree
Overall 43, 41 and nine out of 93 adenomas were resected gross totally (46.2%), subtotally (44%) or partially (9.6%), respectively (Table 2). All of the multihormone secreting adenomas were resected subtotally. All of the TSH secreting adenomas were resected gross totally.
Lessons learned from the different surgical techniques:
Sublabial transgingival approach (12 patients): The sublabial approach is directed under the lip and submucosally along the nasal septum to the sphenoid sinus. At the end of the operation the upper buccal mucosa were closed with absorbable sutures. Patient discomfort due to the limitation of oral intake and nutrition problems and additional problems of breathing due to the nasal airway blockage were noted in all patients after the operation. Postoperative numbness of the anterior teeth was documented in three out of 12 patients. Reconstruction of the sellar defect was done by the fascia and fat tissue which was harvested from right lateral femoral region. All of the patients were revealed discomfort after the operation on the right femoral region. In two patients CSF leak was observed and managed with lumbar continuous drainage. C arm fluoroscopy was used three to five times in every operation.
Transseptal transsphenoidal approach (13 patients): Patient discomfort due to the nasal airway blockage was noted in all patients after the operation. Septum perforation was documented in five patients. Septal mucosal tear was done in eight patients. Reconstruction of the sellar defect was done by the fascia and fat tissue which was harvested from right lateral femoral region. All of the patients were revealed discomfort after the operation on the right femoral region. In two patients CSF leak was observed and managed with lumbar continuous drainage. C arm fluoroscopy was used three to four times in every operation.
Endonasal transsphenoidal approach (15 patients): Patient discomfort was noted due to postoperative extensive packing and nasal airway blockage in all patients after the operation. We have not observed any septum perforation or septal mucosal tear. CSF leak which was treated with lumbar continuous drainage was seen in five patients. One of the patients with CSF leak was undergone a second operation for CSF leak repair. Reconstruction of the sellar defect was done by the fascia and fat tissue which was harvested from right lateral femoral region. All of the patients were revealed discomfort after the operation on the right femoral region. C arm fluoroscopy was used three to four times in every operation.
Endoscopy assisted endonasal transsphenoidal approach (25 patients): Patient discomfort was noted due to postoperative extensive packing and nasal airway blockage was noted in all patients after the operation. CSF leak was noted in five patients. Lumbar continuous drainage was done in all but two of them have undergone CSF leak repair operation for one time by transsphenoidal route. In 15 patients, operations were started with microscope and after the tumour removal the operation field was explored with endoscope. Surgeons were familiarized with endoscope with these eventual explorations. At the beginning of ten operations, surgeons were attempted to make the intranasal step of the operation with endoscope. Five of our first ten attempts, ear nose and throat (ENT) surgeon was helped us during nasal step of the operation. In our early endoscopic operations continuous mucosal bleeding was blocked our view, we lost extra half an hour or more to the control of mucosal bleeding. Septal mucosal tear was happened five of our ten attempts. We have not observed any septum perforation. Due to the bleeding and time loss in the operation we have inserted the speculum and approximated the microscope to the operation field. This was an extra time loss for the team and orientation loss of the neurosurgeon to the operation field. In two patients ENT surgeon removed the middle turbinate, which was blocking the presphenoidal area, in order to facilitate operation. In 8 patients, a hand-held nasal speculum was used to lateralize the middle turbinate at the beginning of endoscopic endonasal step. C arm fluoroscopy was used at two to three times in 15 patients whose operation was started with microscopy. Eight out of ten patients whose operation was started with endoscopic exploration C arm fluoroscopy was use only two times. In the rest two patients we have not used C arm fluoroscopy during the operation.
Purely endoscopic endonasal transsphenoidal approach (28 patients): First three operations were held with the aid of an ear nose and throat (ENT) surgeon. ENT surgeon has excised only in one patient the middle turbinate, which was blocking the operation field, in order to facilitate operation. In the early period of our experience with ten patients, reconstruction of sellar base was done with inlay dural substitute plus onlay fascia and fat tissue beneath them. In order to fix the fat tissue, fibrin glue (tisseel) was then applied and reconstruction was augmented with endonasal packing. Six of 10 patients (60%) in the early period underwent CSF leak repair operations following the tumour resection. Due to the high percentage of CSF leak we have changed our reconstruction technique. In 18 patients, after inlay and onlay fascia application, we have repositioned the middle turbinate after removing the relevant mucosa, as a pedicled flep to intensify the reconstruction. Then we have placed the fat tissue beneath, and fixed the reconstruction with fibrin glue (tisseel) application. CSF leak repair operations were dramatically declined to 11% (two out of 18). In the first 14 pure endoscopic endonasal operations, the balloon located at the tip of a Foley catheter was inflated inside the nose to support the sellar base reconstruction instead of nasal packing. Then we have quitted using any nasal packing after endoscopic endonasal operations. Patient discomfort due to nasal packing was eliminated after operations. In none of the pure endoscopic endonasal operations C arm flouroscopy was used (Fig. 1).

a, b, c, d Forty-year-old man, presented with bitemporal hemianopia. Diagnosis was non-functioning pituitary adenoma. a Preoperative T2 weighted coronal MRI image of pituitary adenoma. b T1 weighted coronal image after endoscopic endonasal operation. c Preoperative T1 weighted sagittal MRI image. d T1 weighted sagittal image after endoscopic endonasal operation
Discussion
In this article, we review the surgical techniques in a series of patients with pituitary adenoma and methodological differentiation in a single institute during last decade. The transsphenoidal route is the most widely used technique for pituitary adenoma surgery due to its rapidity, good tolerance, effectiveness and low complication rate. In our series we used sublabial transgingival, transseptal transsphenoidal, endonasal transsphenoidal, endoscopy assisted endonasal transsphenoidal and purely endoscopic endonasal approach for resecting pituitary adenomas.
Surgical procedures
The transsphenoidal approach is the procedure of choice for pituitary adenomas because it offers a lower morbidity and mortality [1, 4, 14]. In 1967, Hardy introduced the use of an operating microscope he developed and designed for transsphenoidal surgery, which transformed the face of this procedure [5, 7]. Hardy’s technique has undergone many refinements to become the fundamental surgical technique for the removal of pituitary tumours and other sellar lesions over the last 40 years [5, 13, 14]. Most experienced neurosurgeons have reported mortality rates between 0 and 1%, verifying that the procedure is reasonably safe and effective [1, 4, 14]. In our institution, we continued to perform operations as Hardy’s sublabial transseptal transsphenoidal approach to 1998. Then we have subsequently switched to the endonasal approach.
The transseptal approach has been done by a short incision adjacent to the columella, we usually preferred the left side, at the mucocutaneous junction. By using subperichondral dissection, the exposure is advanced submucosally along the anterior edge of the columella to the left side of the nasal septum. The submucosal dissection is directed, by using fluoroscopy, to the sphenoid face. Than the tips of the speculum blades advanced submucosally along the sphenoid face. We have used this method in 13 cases and abandoned due to the difficulties of submucosal dissection especially in the patients who has previous trauma to the nose. In the endonasal approach the view of the microscope is directed through one nostril between the nasal septum and nasal conchae to the sphenoid face below the ostia. No incision is needed in the anterior part of the nasal cavity. A hand-held nasal speculum, inserted under fluoroscopy into one nostril between the conchae and nasal septum, is opened to compress the conchae and septum sufficiently that the endonasal transsphenoidal speculum can be advanced through one nostril to the sphenoid face. Removal of the conchae is not required [16]. In the endoscopy assisted endonasal transsphenoidal approach we used the endoscope to inspect for residual tumour during the endonasal transsphenoidal operation that may be out of the surgeon’s view.
With better knowledge of microsurgical anatomy and modern microinstrumentation, and introduction of endoscope to the operation field, neurosurgeons have modified the microscopic transsphenoidal approach to endoscopic endonasal approach in order to gain better access to regions such as the cavernous sinus and the suprasellar cisterns.
Jho and Carrau have reported a series of 50 patients who underwent endoscopic endonasal transsphenoidal surgery with encouraging results [9]. Cappabianca et al., reported outcome analysis of 100 consecutive procedures performed by endoscopic endonasal transsphenoidal approach (2). Kabil et al reported a series of 300 patients who have undergone fully endoscopic transnasal pituitary adenoma resection in 2005 [10]. We have started to use endoscope to explore the operation field after and or together with microscope as a supplementary device in 2002.
One of the main advantages of this approach is excellent panoramic visualization of the sellar and suprasellar anatomy with increased illumination and magnification [8] (Fig. 2). In the endoscopic operation surgeon inserts endoscope parallel to the middle turbinate and finds the sphenoid ostia under direct vision than performs anterior sphenoidotomy without using fluoroscopy. Lacking of radiation in the operating room is an advantage of endoscopic endonasal operations. As reported in the results section, in all other approach types C arm fluoroscopy were used at least two times in an operation. Anatomic studies have demonstrated that the endoscope provides a volume of exposure superior to that of the operating microscope [17]. With pure endoscopic endonasal approach, extensive mucosal dissection is avoided and postoperative nasal packing is eliminated [3, 10].

a Endoscopic view of sella floor from the nose after opening of sphenoid sinus in an operation. b Endoscopic view of sellar dura from inside of sphenoid sinus after removal of sella floor
Major drawbacks of endoscopic operations include the lack of stereoscopic vision and learning curve for using this technique. In our operations endoscope was driven in a dynamic fashion. This is similar to the vision and orientation principle of pigeons. Three dimensional organization of the vestibuloocular reflex in pigeons are maintained with compensatory eye movements [6]. Pigeons are repetitively makes head movement back and forth to maintain the stereoscopic vision during walking. Lack of stereoscopic vision is get over with dynamic movement of endoscope during the operation.
In our series, at the beginning, involvement of an ENT surgeon to our surgical team facilitated the operations. Twenty-five endoscopy assisted endonasal operations were encouraged us to start the pure endoscopic operations. On the basis of experience gained with the use of endoscope in the operations, some modifications can be made but our small series together with the short follow-up do not allow us to draw definitive conclusions. Resection of middle turbinate at the beginning of the operations may facilitate the operations [12]. In our series we have preferred to preserve the middle turbinate after a few cases. The percentage of CSF leak after operations is also important. In early period of endoscopic surgery, due to the wide panoramic view of the sellar base, surgeon has a propensity to make wider sellar base resection. We think that incomplete reconstruction of wider sellar opening may contribute to the high percentage of CSF leak during early period of endoscopic experience.
Haemorrhage is another big problem for endoscopic operations. Repetitive irrigation with warm water is helpful to stop oozing from sinonasal mucosa during the operation. Systematic solution such as Clearvision of Storz is helpful to maintain the operation.
Preoperative prophylaxis with antibiotics (first generation ceftriaxon), infectious complications were very infrequent in our series. We have seen only one case with meningitis after transsphenoidal surgery due to rhinorrhea and successfully treated with antibiotherapy.
Conclusion
Technologic advancements in endoscopy and gaining experience in pituitary surgery drives neurosurgeons toward less invasive approaches.
References
Black PMcL, Zervas NT, Candia G (1987) Incidence and management of complications of transsphenoidal operation for pituitary adenomas. Neurosurgery 209:20–924
Cappabianca P, Cavallo LM, Colao A, Del Basso De Caro M, Esposito F, Cirillo S, Lombardi G, de Divitiis E (2002) Endoscopic endonasal transsphenoidal approach: outcome analysis of 100 consecutive procedures. Minim Invasive Neurosurg 45(4):193–200
Charalampaki P, Reisch R, Ayad A, Conrad J, Welschehold S, Perneczky A, Wuster C (2007) Endoscopic endonasal pituitary surgery: surgical and outcome analysis of 50 cases. J Clin Neurosci. 14(5):410–415
Ciric I, Ragin A, Baumgartner C, Pierce D (1997) Complications of transsphenoidal surgery: results of a national survey, review of the literature, and personal experience. Neurosurgery 40:225–237
Couldwell WT (2004) Transsphenoidal and transcranial surgery for pituitary adenomas. Journal of Neuro-Oncology 69:237–256
Dickman JD, Beyer M, Hess BJ (2000) Three-dimensional organization of vestibular related eye movements to rotational motion in pigeons. Vision Res. 40(20):2831–2844
Hardy J (1967) La chirugie de l’hypophyse par voie transsphenoidale. Union Med Can 96:702–712
Jho HD, Carrau RL, Ko Y, Daly MA (1997) Endoscopic pituitary surgery: an early experience. Surg Neurol 47:213–222
Jho HD, Carrau RL (1997) Endoscopic endonasal transsphenoidal surgery: experience with 50 patients. J Neurosurg 87(1):44–51
Kabil MS, Eby JB, Shahinian HK (2005) Fully endoscopic endonasal vs. transseptal transsphenoidal pituitary surgery. Minim Invasive Neurosurg 48(6):348–354
Kassam AB, Gardner P, Snyderman C, Mintz A, Carrau R (2005) Expanded endonasal approach: fully endoscopic, completely transnasal approach to the middle third of the clivus, petrous bone, middle cranial fossa, and infratemporal fossa. Neurosurg Focus 15(1):19
Koc K, Anik I, Ozdamar D, Cabuk B, Keskin G, Ceylan S (2006) The learning curve in endoscopic pituitary surgery and our experience. Neurosurg Rev 29:298–305
Laws ER Jr, Piepgras DG, Randall RV, Abboud CF (1979) Neurosurgical management of acromegaly. Results in 82 patients treated between 1972 and 1977. J Neurosurg 50:454–461
Laws ER Jr (1987) Pituitary surgery. Endocrinol Metab Clin N Am 16:647–665
Liu JK, Das K, Weiss MH, Laws ER Jr, Couldwell WT (2001) The history and evolution of transsphenoidal surgery. J Neurosurg 95(6):1083–1096
Rhoton AL (2002) The sellar region. Neurosurgery 51(Suppl 1):335–374
Spencer WR, Das K, Nwagwu C, Wenke E, Schaeffer SD, Moscatello A, Couldwell WT (1999) Approaches to the sellar and parasellar region: anatomic comparison of the microscope vs endoscope. Laryngoscope 109:791–794
Youssef AS, Agazzi S, van Loveren HR (2005) Transcranial surgery for pituitary adenomas. Neurosurgery 571(Suppl):168–175
Author information
Authors and Affiliations
Corresponding author
Additional information
Comment
This paper provides a longitudinal view of the progression in technique for surgery of pituitary lesions over the past decade or so. This period was marked by increasing enthusiasm for the trans-nasal endoscopic approach, and by the adoption of this technique by several forward-looking groups in many parts of the world.
Along with others, the investigators began with the traditional sub-labial microscopic approach which has served patients so well for many years after its re-introduction in the 1970’s. Along with others, they then moved to the direct endo-nasal microscopic approach which has been considered quicker and less “invasive”. The next step was the introduction of the endoscope in traditional endo-nasal exposures, using the nasal speculum or retractor. Finally, they adopted and report upon the “pure” endoscopic approach, without speculum. They also have generally abandoned the use of intraoperative fluoroscopy and neuronavigation. Although their experience is somewhat limited in numbers of patients, the progression is logical and the results are very good.
One of the alleged advantages of the pure endoscopic approach is that it is “minimally invasive”. Experience tells us that although the surgical trauma to the nasal structures may be less, this technique requires a more extensive sphenoidotomy in order to assure full mobility of the endoscope and lack of collision with other instruments. In this respect it is actually more invasive, particularly when the turbinate is resected, a procedure which we find unnecessary in most cases.
There is debate about the use of intraoperative imaging and navigation. In training programs, these adjuncts may be valuable in the education of residents and fellows. There is also debate about whether all young neurosurgeons should follow this type of progressive approach or whether they should simply begin with the endoscopic methods that have proven to be so effective.
Edward Laws and John A Jane Jr
Rights and permissions
About this article
Cite this article
Duz, B., Harman, F., Secer, H.I. et al. Transsphenoidal approaches to the pituitary: a progression in experience in a single centre. Acta Neurochir (Wien) 150, 1133–1139 (2008). https://doi.org/10.1007/s00701-008-0135-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-008-0135-y