
Abstract
Adenocarcinoma is the predominant histological type of carcinoma of the gallbladder, accounting for more than 80% of all gallbladder carcinomas. In contrast, carcinosarcoma of the gallbladder is an extremely atypical subset of gallbladder malignancies. It is characterized by the presence of both epithelial and mesenchymal components. Currently, fewer than 100 cases have been reported in the English literature. Therefore, knowledge and experience regarding this disease are limited. Recently, we experienced two cases of gallbladder carcinosarcoma, which were diagnosed as gallbladder carcinoma based on the preoperative clinical and radiological examinations. Cholecystectomies were performed in both cases, and the malignant tumor cells included carcinomatous and sarcomatous components histologically. The final pathological diagnoses were carcinosarcoma of the gallbladder. We herein report these two cases of gallbladder carcinosarcoma and review the previous pertinent literature.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Carcinosarcoma of the gallbladder is a rare tumor, accounting for <1% of gallbladder carcinomas. It is characterized by tumor cells with both malignant epithelial and mesenchymal components. Carcinosarcoma arises most commonly in the gynecological or otorhinolaryngological regions, including the uterus, thyroid, esophagus, and upper respiratory tract [1, 2]. Carcinosarcoma of the gallbladder is a very aggressive malignancy, which spreads by the direct invasion of adjacent organs, hematogenously, and by lymph node metastasis. It is usually discovered at an advanced stage and has a propensity to invade the surrounding organs and vessels. Fewer than 100 cases of gallbladder carcinosarcoma have been reported in the English literature. We herein present two cases of carcinosarcoma of the gallbladder treated by surgical resection.
Case presentation
Case 1
A 72-year-old female presented with intermittent postprandial abdominal discomfort that began 6 days before admission. Abdominal ultrasonography showed a solid mass originating from the fundus of the gallbladder that filled most of the gallbladder lumen; gallstones were also present. Abdominal computed tomography (CT) revealed a solid mass in the gallbladder (Fig. 1a), and magnetic resonance imaging (MRI) showed irregular wall thickening with enhancement of the fundus of the gallbladder (Fig. 2a). The laboratory data revealed that the liver and renal function were within the normal limits, and the serum levels of tumor markers [carcinoembryonic antigen (CEA) and carbohydrate antigen 19-9 (CA 19-9)] were normal. The initial diagnosis was gallbladder cancer, and elective surgery was performed.

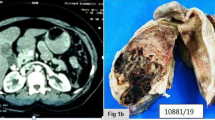
The abdominal computed tomography (CT) findings. a Abdominal CT revealed a solid mass in the gallbladder (Case 1). b Abdominal CT showed a 1.5 cm enhanced mass in the gallbladder (Case 2)

The abdominal magnetic resonance imaging (MRI) findings. a, b MRI showed irregular wall thickening with enhancement of the fundus of the gallbladder (Case 1). MRI revealed 1.5 cm (c) and 1.8 cm (d) polypoid masses originating from the fundus of the gallbladder (Case 2)
During the surgery, a frozen biopsy of the gallbladder mass revealed that it was a malignant mesenchymal tumor. A radical cholecystectomy was performed with a wedge resection of the liver (gallbladder bed), combined with a hepatoduodenal ligament lymphadenectomy.
The macroscopic examination of the specimen showed a 6.5 × 4.5 × 4.5 cm tumor with a polypoid structure, which originated from the fundus of the gallbladder and filled the entire gallbladder lumen. The tumor was a solid mass with hemorrhagic and necrotic foci (Fig. 3a). Microscopically, the tumor was composed of both: epithelial (Fig. 4a) and mesenchymal (Fig. 4b) components. The mesenchymal components showed widespread crossing bundles, and the epithelial components formed glandular tissues in focal areas (Fig. 4b). The degree of necrosis and hemorrhage comprised <50% of the specimen. An immunohistochemical examination showed positive staining for cytokeratin (CK), CK20, CK7 (Fig. 4c), CEA, and E-cadherin in the epithelial components, and vimentin and osteocalcin in the mesenchymal components, and focal staining for S-100 and actin. S-100 staining was positive in the chondroid differentiated sarcomatous components (Fig. 4d). Ki67 and p53 staining were positive in both the carcinomatous components and sarcomatous components. Staining for smooth muscle actin (SMA), myoglobin, and desmin was negative. No lymph node metastasis was observed. The final diagnosis was well to moderately differentiated adenocarcinoma and chondroid differentiated sarcoma (carcinosarcoma of the gallbladder). The patient was discharged on the 13th postoperative day.

The gross findings of carcinosarcoma of the gallbladder. a The gross examination revealed a 6.5 × 4.5 × 4.5 cm tumor with a polypoid structure, arising from the fundus of the gallbladder and filling the entire bladder lumen. The tumor was solid, hemorrhagic, and necrotic in appearance (Case 1). b The gallbladder was filled with a necrotic polypoid mass and the tumor in the gallbladder had spread to the liver (Case 2)

The microscopic and immunohistochemical findings of Case 1. Histologically, the tumor contains two distinct components: a well to moderately differentiated adenocarcinoma (a) and chondroid differentiated sarcomatous tissue (b) (H&E stain, ×100). Immunohistochemistry showed CK7 staining mainly in the carcinomatous components (c) (×100) and the chondroid differentiated sarcomatous portions were positive for S-100 (d) (×200)
Three months later, a follow-up abdominal CT revealed a 1.3 cm nodular enhancing mass lesion in the liver. She was given six cycles of chemotherapy with 5-FU and cisplatin, but the tumor progressed with direct invasion of the colonic loop, stomach, and liver. The patient has been followed semiannually with routine imaging and laboratory studies.
Case 2
An 81-year-old male visited our hospital complaining of epigastric discomfort. An abdominal CT scan revealed a 1.5 cm mass in the gallbladder (Fig. 1b), and the cholangiogram MRI revealed 1.5 and 1.8 cm polypoid masses originating from the fundus of the gallbladder with a l cm enlarged lymph node in the pericholecystic area (Fig. 2b). The laboratory data revealed that the patient’s liver and renal function were within normal limits, and the CEA and CA 19-9 levels were normal. The initial diagnosis was gallbladder cancer.
A cholecystectomy with liver segmentectomy (S4a, 5) and lymph node dissection were performed. The gallbladder was filled with a necrotic polypoid mass, and the gallbladder tumor had spread to the liver directly (Fig. 3b). Histologically, the tumor contained two distinct components: a moderately differentiated tubular adenocarcinoma (Fig. 5a) and undifferentiated sarcomatoid tissue (Fig. 5b). The sarcomatous component was located mainly in the part of the tumor that had spread to the liver. No anaplastic spindle cells or other differentiated elements were observed. The degree of necrosis and hemorrhage comprised <50% of the specimen. CK and CEA staining were positive in most of the adenocarcinomatous components (Fig. 5c). The sarcomatous portions were positive for vimentin (Fig. 5d) and CD34, and focally positive for epithelial membrane antigen (EMA). Ki67 and p53 staining were positive in both the carcinomatous and sarcomatous components, while stronger staining was noted in the sarcomatous components than in the carcinomatous components. Microscopic and immunohistochemical staining did not help to determine the subtype of the sarcoma, because the degree of differentiation was poor.

The microscopic and immunohistochemical findings of Case 2. Histologically, the tumor contained two distinct components: a moderately differentiated tubular adenocarcinoma (a) and undifferentiated sarcomatous tissue (b) (H&E stain, ×100). Immunohistochemistry showed cytokeratin (CK) staining mainly in the adenocarcinomatous components (c) and the sarcomatous portions were positive for vimentin (d) (×200)
Based on these results, the tumor was diagnosed as moderately differentiated adenocarcinoma and undifferentiated sarcoma (carcinosarcoma of the gallbladder). The patient had an uneventful postoperative course. However, he was readmitted with a recurrence involving peritoneal dissemination with tumor cells detected in ascites; he died 4 months after the initial surgery.
Discussion
Carcinosarcoma is characterized by malignancy with both epithelial and mesenchymal components within the same tissue. In many case reports, several names have been used for this entity, including sarcomatoid carcinoma and spindle cell carcinoma [3–5]. Some pathologists also include this entity in the category of undifferentiated carcinoma of the gallbladder without further subclassification. The epithelial (carcinomatous) component usually consists of adenocarcinoma, although an element of squamous cell carcinoma is also occasionally observed. The mesenchymal (sarcomatous) component typically consists of undifferentiated spindle or satellite cells, and is occasionally accompanied by various proportions of heterogenous elements, including chondrosarcoma, osteosarcoma, and rhabdomyosarcoma [6].
To our knowledge, since carcinosarcoma of the gallbladder was first described in 1907 by Landsteiner [7], fewer than 100 cases have been reported in the English literature. In 2008, Zhang et al. [5] reviewed 68 cases of gallbladder carcinosarcoma (mean patient age: 68.8 years; range 45–91 years). The female-to-male ratio was 3.25:1 and 66.7% of the patients had gallstones.
Although recent studies have suggested some causative factors, such as multistep genetic alterations, the precise mechanism of gallbladder carcinogenesis remains unknown [8].
The symptoms and signs of gallbladder carcinosarcoma are non-specific. Representative clinical symptoms include right upper abdominal pain and masses, loss of appetite, weight loss, general fatigue, jaundice, and vomiting. At laparotomy, most patients have locally advanced disease involving the gallbladder bed or distant metastasis [4].
The preoperative diagnosis of this tumor is usually gallbladder cancer, as in our cases. The final diagnosis requires the presence and intermingling of both the carcinomatous and sarcomatous components histologically. An immunohistochemical examination should show that the epithelial (carcinomatous) component is positive for cytokeratin, while the mesenchymal (sarcomatous) component is positive for vimentin [3, 9–12]. Table 1 summarizes the immunohistochemical features of gallbladder carcinosarcoma reported in the literature.
Due to the paucity of cases, there is no staging system for carcinosarcoma, nor has any consensus been established on the management of gallbladder carcinosarcoma. The usual treatment of choice is surgery and no successful treatment has so far been reported with radiotherapy or chemotherapy [9].
However, even with aggressive surgical resection, the prognosis of gallbladder carcinosarcoma is generally poor. Most cases present with locally advanced disease. Liver metastasis and peritoneal dissemination are common in these cases. The adrenal glands, pancreas, diaphragm, and lower thoracic vertebrae are other reported metastatic sites. The regional, retroperitoneal, and para-aortic lymph nodes may be involved. Even when a curable resection is performed, many patients die shortly after the operation because of recurrence or metastasis. The mean survival after diagnosis is usually only a few months [6, 13]. One of our patients (Case 2) died 4 months after surgery. According to Okabayashi et al. [13], the 3-year survival rate after surgical resection of carcinosarcoma of the gallbladder is 31.1%.
The current knowledge of, and predictions regarding gallbladder carcinosarcoma are based on a limited number of case reports. The precise mechanisms of gallbladder carcinogenesis remain unknown. We herein presented two cases of gallbladder carcinosarcoma that were successfully treated by surgical resection.
References
Jonson AL, Bliss RL, Truskinovsky A, Judson P, Argenta P, Carson L, et al. Clinical features and outcomes of uterine and ovarian carcinosarcoma. Gynecol Oncol. 2006;100:561–4.
Batsakis JG, Suarez P. Sarcomatoid carcinomas of the upper aerodigestive tracts. Adv Anat Pathol. 2000;7:282–93.
Takahashi Y, Fukushima J, Fukusato T, Shiga J. Sarcomatoid carcinoma with components of small cell carcinoma and undifferentiated carcinoma of the gallbladder. Pathol Int. 2004;54:866–71.
Landsteiner K. Plattenepithenelkarzinon und sarkom der gallen-blasse in einem falle von gallenblasse. Ztschr Klin Med. 1907:427–33.
Zhang L, Chen Z, Fukuma M, Lee LY, Wu M. Prognostic significance of race and tumor size in carcinosarcoma of gallbladder: a meta-analysis of 68 cases. Int J Clin Exp Pathol. 2008;1:75–83.
Kuroki T, Tajima Y, Matsuo K, Kanematsu T. Genetic alterations in gallbladder carcinoma. Surg Today. 2005;35:101–5.
Huguet KL, Hughes CB, Hewitt WR. Gallbladder carcinosarcoma: a case report and literature review. J Gastrointest Surg. 2005;9:818–21.
Hotta T, Tanimura H, Yokoyama S, Ura K, Yamaue H. So-called carcinosarcoma of the gallbladder; spindle cell carcinoma of the gallbladder: report of a case. Surg Today. 2002;32:462–7.
Sodergren MH, Silva MA, Read-Jones SL, Hubscher SG, Mirza DF. Carcinosarcoma of the biliary tract: two case reports and a review of the literature. Eur J Gastroenterol Hepatol. 2005;17:683–5.
Agarwal T, Jain M, Goel A, Visayaragavan P, Gupta RK. Carcinosarcoma of the gallbladder. Indian J Pathol Microbiol. 2009;52:244–5.
Shimada K, Iwase K, Aono T, Nakai S, Takeda S, Fujii M, et al. Carcinosarcoma of the gallbladder producing alpha-fetoprotein and manifesting as leukocytosis with elevated serum granulocyte colony-stimulating factor: report of a case. Surg Today. 2009;39:241–6.
Uzun MA, Koksal N, Gunerhan Y, Celik A, Gunes P. Carcinosarcoma of the gallbladder: report of a case. Surg Today. 2009;39:168–71.
Okabayashi T, Sun ZL, Montgomery RA, Hanazaki K. Surgical outcome of carcinosarcoma of the gall bladder: a review. World J Gastroenterol. 2009;15:4877–82.
Conflict of interest
None of authors have a conflict of interest or any financial support.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kim, HH., Hur, YH., Jeong, EH. et al. Carcinosarcoma of the gallbladder: report of two cases. Surg Today 42, 670–675 (2012). https://doi.org/10.1007/s00595-012-0160-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00595-012-0160-6