
Abstract
We report a case of antibody-mediated rejection (AMR) of a unilateral donor lung in the presence of newly formed donor-specific antibodies, 10 months after living-donor lobar lung transplantation (LDLLT). Of note is that the AMR occurred in the unilateral lung. Furthermore, the lung graft was from her husband and HLA analysis on the recipient’s daughter revealed the same donor-specific HLA antigens, which strongly suggested pre-sensitization before lung transplantation. Fortunately, we could perform direct crossmatch even 1 year after lung transplantation because of the living donors.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Guidelines for the diagnosis and treatment of antibody-mediated rejection (AMR) in solid organ transplantation have recently been published [1]. AMR is an accepted form of allograft failure in solid organ transplants, and although rarely reported in patients undergoing lung transplantation [2, 3], has become a topic of interest in the field of lung transplantation [4, 5].
The shortage of donors is still a major problem all over the world. To save the life of a rapidly deteriorating critically ill patient, living-donor transplantation, particularly living-donor lobar lung transplantation (LDLLT), is being performed successfully in Japan [6, 7]. The characteristics of AMR after LDLLT are distinctly different from those of AMR after cadaveric lung transplantation. We report a case of allograft dysfunction in the presence of newly formed donor-specific antibodies (DSA), 10 months after LDLLT.
Case report
A 34-year-old woman with idiopathic pulmonary fibrosis underwent bilateral LDLLT. The donor of the right lobe was her husband and the donor of the left lobe was her mother. Preoperative direct crossmatch was negative with the anti-human globulin complement-dependent cytotoxicity (AHG-CDC) crossmatch and the flow cytometry crossmatch (FCXM) methods. HLA typing showed the following: A24, A26, B35, B61, C9, C10, DR8, DR15, DQ6, DQ8 for the patient; A31, A33, B44, B62, C7, C14, DR12, DR13, DQ 6, DQ7 for the husband; and A24, B35, B52, C9, C12, DR15, DQ6 for the mother (Table 1). The patient was screened for anti-HLA antibodies using the LABScreen Single Antigen assay (One Lamda Inc, Canoga Park, CA, USA), but no HLA antibodies were detected. Surgery was performed with cardiopulmonary bypass and there were no complications. The immunosuppressant regimen consisted of cyclosporine, azathioprine, and prednisone without induction therapy. During postoperative week 1, she experienced an episode of acute rejection, which was clinically diagnosed and treated successfully by steroid pulse therapy. The azathioprine (2 mg/kg daily) was then changed to mycophenolate mofetil (1500 mg/body daily). She was very compliant with her immunosuppressant intake and her cyclosporine level was always stable throughout the course. She remained well until 10 months after LDLLT, without any sign of oxygen desaturation on exertion (Table 2). She had even been taking care of her child by herself all day. However, 11 months after LDLLT she began to experience shortness of breath, which did not resolve within a month and she went to a regional hospital. Chest computed tomography (CT) showed diffuse infiltrates only in the right lung. Her laboratory data showed a white blood cell count of 5900 cells/dl and a CRP value of 4.6 mg/dl. Her oxygen saturation was 95% in room air, but dropped below 90% on exertion. Her pulmonary function test results were obviously deteriorating (Table 2). She was referred to our hospital for further investigation. Various microbiological tests excluded infection, but the infiltrates in the right lung worsened within 1 week (Fig. 1). She was also screened again for anti-HLA antibodies using the LABScreen Single Antigen assay. Since there was no evidence of infection and her condition was deteriorating, we decided to commence her on steroid pulse therapy with the empirical use of antibiotics. The infiltrates subsided in a couple of days, but screening for anti-HLA antibodies revealed the presence of newly developed DSA (C7 in class I and DQ7 in class II). Thus, we performed direct crossmatch between the patient and two donors again. Although the AHG-CDC crossmatch was negative, the FCXM (B cell) was positive for the patient and her husband. Based on these findings, we diagnosed AMR caused by de novo DSA. With the limited information about treatments for AMR after lung transplantation, repetitive careful informed consents were obtained and we ultimately decided to treat the patient aggressively, starting with plasmapheresis to try to eliminate DSA in the serum. Screening for anti-HLA antibodies after two courses of plasmapheresis demonstrated that C7 was gone but that mean fluorescence intensity (MFI) of DQ7 had increased as a rebound phenomenon. After discussion, we concluded that plasmapheresis could not completely remove the DSA, particularly DQ7, and it was stopped. Instead, we gave her high dose (1 mg/kg) intravenous immune globulin (IVIG), followed by a single dose of rituximab (375 mg/m2). Screening for anti-HLA antibodies 1 month later still showed the existence of DSA with almost the same MFI, but the patient’s respiratory condition was stabilized (Table 2). Chest X-ray 1 month after rituximab administration revealed remarkable improvement (Fig. 2).

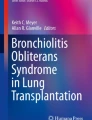
a Chest X-ray film on admission, showing diffuse infiltrates in the right lung. b Chest computed tomography (CT) scan on admission, showing diffuse patchy infiltrates only in the right lung

a Chest X-ray film 1 month after treatment, showing remarkable improvement. b Chest CT scan 1 month after treatment, showing obvious improvement
She was discharged and flew back to her hometown, where she is self-administering monthly IVIG (0.5 g/kg). Now, 4 months after rituximab treatment, the DSA is still present with almost the same MFI, but chest X-ray and CT films do not show any adverse changes. Her respiratory state is stable, but the most recent pulmonary function test suggests gradual progression of BOS (Table 2).
Discussion
Lung transplantation is an established treatment for severely ill patients with respiratory failure, but the donor shortage has led transplant programs to use organs from living related healthy donors, particularly in Japan. AMR is recognized as a form of allograft failure of solid organ transplantation, but it is uncommon after lung transplantation [2, 3]. Although AMR is an increasingly recognized entity even in lung transplantation [4, 8], to the best of our knowledge, there is no report of AMR occurring after LDLLT. This seems to be the first report of allograft dysfunction developing in the presence of de novo DSA, 10 months after LDLLT.
The 26th official adult lung and heart/lung transplantation report, published in 2009, documented disappointing long-term survival after lung transplantation, with median survival after transplantation of only 5 years [9]. Chronic lung allograft dysfunction is associated with the pre-existence or development of anti-HLA alloantibodies in lung transplant recipients [10]. The development of anti-HLA antibodies is now recognized as an important risk factor for bronchiolitis obliterans syndrome (BOS) [11–13]. Moreover, patients who developed post-transplant HLA antibodies exhibited increased prevalence of refractory acute cellular rejection and lymphocytic bronchiolitis, as well as BOS [10]. Since the most important feature of HLA antibodies in a lung transplantation recipient or candidate is most probably the donor specificity, DSA is currently considered as a target for treatment. According to the most recent article by Hachem et al. [5], we treated our patient aggressively after repetitive informed consents. Interestingly, Hachem et al. [5] reported that DSA developed in more than 50% of recipients after lung transplantation when they used the sensitive screening method of LABScreen Single Antigen assay, as used for DSA detection in our patient.
The present case report highlights several interesting points. First, AMR occurred in the hemilateral lung since there were two donor lungs in this LDLLT. During the course, there was no apparent change in the left lung donated from her mother. Unlike lung transplantation from cadaveric donors, LDLLT recipients might be advantaged in that contralateral lung would probably be free from AMR. Second, the AMR occurred in the lung graft, from her husband. Although the exact mechanism is unknown, there might have been a pre-sensitization between them at the time of pregnancy and delivery before LDLLT. This patient has one daughter and her HLA analysis revealed both C7 and DQ7 HLA antigens, which is evidence of pre-sensitization before lung transplantation (Table 1). However, there was no evidence of DSA preoperatively, so LDLLT was performed, followed by an uneventful clinical course for 9 months. Third, we could perform direct crossmatch even 1 year after lung transplantation because of the living donors. Since C4d staining for the lung tissue is still technically difficult and its results are difficult to interpret, the direct crossmatch results in our case allowed us to avoid this unreliable and invasive diagnostic method.
In conclusion, we discussed a case of allograft dysfunction developing in the presence of newly formed DSA almost 1 year after LDLLT.
References
Takemoto SK, Zeevi A, Feng S, Colvin RB, Jordan S, Kobashigawa J, et al. National Conference to assess antibody-mediated rejection in solid organ transplantation. Am J Transplant. 2004;4:1033–41.
Morrell MR, Patterson GA, Trulock EP, Hachem RR. Acute antibody-mediated rejection after lung transplantation. J Heart Lung Transplant. 2009;28:96–100.
Girnita AL, McCurry KR, Yousem SA Pilewski J, Zeevi A. Antibody-mediated rejection in lung transplantation: case reports. Clin Transpl 2006; 508–10.
Glanville AR. Antibody-mediated rejection in lung transplantation: myth or reality? J Heart Lung Transplant. 2010;29:395–400.
Hachem RR, Yusen RD, Meyers BF, Aloush AA, Mohanakumar T, Patterson GA, et al. Anti-human leukocyte antigen antibodies and preemptive antibody-directed therapy after lung transplantation. J Heart Lung Transplant. 2010;29:973–80.
Shiraishi T, Okada Y, Sekine Y, Chida M, Bando T, Oto T, et al. Registry of the Japanese Society of Lung and Heart-Lung Transplantation: the official Japanese lung transplantation report 2008. Gen Thorac Cardiovasc Surg. 2009;57:395–401.
Yoshimura N, Okajima H, Ushigome H, Sakamoto S, Fujiki M, Okamoto M. Current status of organ transplantation in Japan and worldwide. Surg Today. 2010;40:514–25.
Martinu T, Chen DF, Palmer SM. Acute rejection and humoral sensitization in lung transplant recipients. Proc Am Thorac Soc. 2009;6:54–65.
Christie JD, Edwards LB, Aurora P, Dobbels F, Kirk R, Rahmel AO, et al. The Registry of the International Society for Heart and Lung Transplantation: twenty-sixth official adult lung and heart/lung transplantation report—2009. J Heart Lung Transplant. 2009;28:1031–49.
Girnita AL, McCurry KR, Zeevi A. Increased lung allograft failure in patients with HLA-specific antibody. Clin Transpl 2007; 231–239.
Sundaresan S, Mohanakumar T, Smith MA, Trulock EP, Lynch J, Phelan D, et al. HLA-A locus mismatches and development of antibodies to HLA after lung transplantation correlate with the development of bronchiolitis obliterans syndrome. Transplantation. 1998;65:648–53.
Smith MA, Sundaresan S, Mohanakumar T, Trulock EP, Lynch JP, Phelan DL, et al. Effect of development of antibodies to HLA and cytomegalovirus mismatch on lung transplantation survival and development of bronchiolitis obliterans syndrome. J Thorac Cardiovasc Surg. 1998;116:812–20.
Palmer SM, Davis RD, Hadjiliadis D, Hertz MI, Howell DN, Ward FE, et al. Development of an antibody specific to major histocompatibility antigens detectable by flow cytometry after lung transplant is associated with bronchiolitis obliterans syndrome. Transplantation. 2002;74:799–804.
Conflict of interest
The authors of this manuscript have no conflicts of interest to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Chen, F., Chibana, N., Kanematsu, A. et al. Antibody-mediated rejection of a unilateral donor lung in bilateral living-donor lobar lung transplantation: report of a case. Surg Today 42, 808–811 (2012). https://doi.org/10.1007/s00595-012-0151-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00595-012-0151-7