
Abstract
Late complications in type 2 diabetic patients are commonly associated with accelerated development of atherosclerosis. In type 2 diabetes mellitus, non-enzymatic glycosylation of apo-B that is a function of hyperglycaemia is an efficient biochemical way of low-density lipoprotein atherogenic modification. So, proper metabolic control is needed to prevent late complications of diabetes. The study was performed to estimate the effects of time-released garlic powder tablet Allicor on the parameters of metabolic control and plasma lipids in type 2 diabetes mellitus. The metabolic action of Allicor was investigated in the 4-week double-blinded placebo-controlled study in 60 type 2 diabetic patients. Fasting blood glucose was measured daily, and serum fructosamine as well as cholesterol and triglyceride levels were determined at the baseline, after 1, 2, 3 and 4 weeks. It has been demonstrated that treatment with Allicor resulted in better metabolic control due to the lowering of fasting blood glucose, serum fructosamine and serum triglyceride levels. The results of this study may allow recommending garlic powder tablets Allicor for the treatment of type 2 diabetes mellitus along with dietary treatment and/or sulfonylurea derivatives to achieve better metabolic control. The benefits from garlic preparations may lead to the reduction of cardiovascular risk in diabetic patients.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Type 2 diabetes mellitus is characterized by premature accelerated atherosclerosis development leading to early invalidization and high mortality in this category of patients [1, 2]. Atherosclerosis, by far the greatest killer in modern society, is a complex disease that develops because of many risk factors including alterations in plasma lipid and lipoprotein levels, blood pressure regulation, platelet function, clotting factors, arterial smooth muscle cell metabolism, etc. [3]. Among all risk factors of atherosclerosis, diabetes mellitus is thought to be one the most potent that greatly increases the risk of cardiovascular diseases of atherosclerotic origin [4, 5]. Dietary therapy is generally considered to be the first step in the treatment of diabetic patients. Garlic (Allium sativum) is used in the traditional medicine of many cultures for the treatment of different diseases, including diabetes [6]. The medicinal use of garlic dates back to thousands of years. Historically, there has been great interest in the role of garlic in reducing cardiovascular risk factors, but there was little scientific support of its therapeutic and pharmacologic properties until recently, when the effects of garlic have been extensively evaluated. The modern interest in the use of garlic in the treatment of diabetes mellitus increased due to the new data on its hypoglycaemic, hypolipidemic and antiatherosclerotic properties [7–9]. Since diabetes mellitus induces complex alterations in metabolic state including not only hyperglycaemia but also dyslipidaemia and increased blood serum atherogenicity, the pluripotent effects of garlic demand further profound investigations. This study was performed to evaluate the glucose- and lipid-lowering potency of new garlic-based formulation, namely, time-released garlic powder tablets Allicor, in type 2 diabetic patients. Evidence obtained from this randomized placebo-controlled study supports the hypothesis that garlic has the potential to prevent cardiovascular disorders in diabetic patients due to the regulation of metabolic control.
Subjects, materials and methods
The primary goal of the study was the estimation of the effects of garlic powder tablets Allicor (INAT-Farma, Russia) on the parameters of metabolic control and plasma lipids in type 2 diabetes mellitus. Allicor contains 150 mg of dehydrated garlic powder and possesses a prolonged action due to slow-release technology employed in manufacturing process.
This study was kept in accordance with the Helsinki Declaration of 1975 as revised in 1983. It was approved by the local ethical committee. All participants gave their informed consent prior to their inclusion in the study.
This study was 4-weeks randomized double-blinded placebo-controlled outpatient clinical trial of 60 type 2 diabetic patients (26 men, 34 women) of varying ages, from 34 to 62 years (mean age, 48.2 ± 2.6 years), receiving oral hypoglycaemics–sulfonylurea derivatives. The patients eligible for recruitment did not receive beta-blockers, calcium antagonists, angiotensin-converting enzyme inhibitors or diuretics. According to the state of metabolic control at the time of inclusion in the study, the patients were divided into two groups.
Those patients who had steady levels of fasting blood glucose below or equal to 8.0 mmol/l (20 patients, 8 men and 12 women) were randomized to receive monotherapy either with Allicor (300 mg twice a day, 10 patients) or placebo (10 patients). Placebo and Allicor tablets looked identical. The treatment regimen included the withdrawal of oral hypoglycaemics–sulfonylurea derivatives for the whole period of the study. During the study, all participants were maintained on the standard diet usually recommended for diabetic patients. The daily measurements of fasting blood glucose were used to monitor the early changes in metabolic control, and the steady increase of fasting blood glucose above 9.5 mmol/l served as the exclusion criterion, and such patients were excluded from the study and turned to previously used regimen of treatment with oral hypoglycaemics.
Those patients who had steady levels of fasting blood glucose above 8.0 mmol/l (40 patients, 18 men and 22 women) were included into the group of combined therapy, i.e., were randomized either to receive Allicor (300 mg twice a day, 20 patients) or placebo (20 patients) in addition to continuing treatment with oral hypoglycaemics–sulfonylurea derivatives. During the study, all participants were maintained on the standard diet recommended for diabetic patients, as well.
The venous blood for lipid analysis and estimation of metabolic control was taken after overnight fasting at the baseline, after 1, 2, 3 and 4 weeks of placebo-controlled treatment phase. To obtain serum, the blood was incubated for 1 h at 37°С and centrifuged for 15 min at 1,500g. Cholesterol and triglyceride levels were measured by commercial enzymatic kits (Boehringer Mannheim GmbH, Germany). Serum HDL cholesterol concentrations were measured after precipitation with magnesium chloride phosphotungstic acid reagent (Boehringer Mannheim GmbH, Germany). Serum LDL cholesterol was calculated by Friedewald formula as the difference between total cholesterol and the sum of HDL cholesterol and 1/2.3 triglycerides. Serum fructosamine was determined colorimetrically by the kinetics of reaction with nitroblue tetrazolium [10] using calibrated hyperglycaemic human serum (Boehringer Mannheim GmbH, Germany) as a standard.
Results are expressed in terms of means and SEM. Significance of differences was evaluated using SPSS 10.1.7 statistical program package (SPSS Inc., USA) and defined at the 0.05 level of confidence. The changes in lipid levels, fasting blood glucose and serum fructosamine levels from baseline to the mean of follow-up measurements were analyzed by a two-way ANCOVA and paired two-tailed t-test.
Results
The results of the study are shown in Tables 1 and 2.
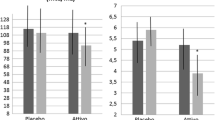
In Type 2 diabetic patients who received monotherapy with Allicor, a significant decrease in serum triglyceride levels was observed after 3 weeks of treatment, and by the end of the study the difference from baseline levels accounted for 36% (p < 0.05). At the same time, the levels of total cholesterol, HDL cholesterol and LDL cholesterol did not change significantly (Table 1). The improvement of metabolic control was also observed in Allicor-treated patients. Serum fructosamine levels were significantly lower after 3 and 4 weeks of treatment as compared to placebo group, and decreased significantly as compared to baseline levels by the end of the study (p < 0.05) (Table 2). Additionally, fasting blood glucose levels decreased and were maintained at the mean levels below than 7.0 mmol/l during the whole period of the study (Table 2). The significant difference in mean fasting blood glucose levels from placebo patients was observed after 2, 3 and 4 weeks of treatment. None of Allicor-treated patients was excluded from the study due to the impairments in fasting glucose levels.
In placebo group, no significant changes in lipid levels were observed (Table 1). There were no significant changes in serum fructosamine levels, as well (Table 2). However, fasting blood glucose levels began increasing after the withdrawal of oral hypoglycaemics, and this lead to the discontinuation of the study in six patients out of ten due to the steady increase of fasting blood glucose above 9.5 mmol/l. Two patients in placebo group were excluded from the study during the second week, three patients—during the third week, and one patient—during the fourth week of the study.
In type 2 diabetic patients who received combined therapy with Allicor and oral hypoglycaemics, serum triglyceride levels decreased, and significant changes were observed after 3 weeks of treatment, similar to the patients who received monotherapy with Allicor. By the end of the study the difference from baseline levels accounted for 26% (p < 0.05). The levels of total cholesterol, HDL cholesterol and LDL cholesterol did not change significantly (Table 1). Additionally, improvement of metabolic control was observed, namely, serum fructosamine levels were significantly lower after 1, 3 and 4 weeks of treatment as compared to placebo group, and decreased significantly as compared to baseline levels after 3 weeks of treatment and by the end of the study (p < 0.05) (Table 2). Fasting blood glucose was maintained at the mean levels below or equal to 9.0 mmol/l during the whole period of the study (Table 2). Moreover, the significant difference in mean fasting blood glucose as compared to baseline levels was observed after the first week of treatment, and some patients experienced hypoglycaemic episodes that demanded the correction of daily dosage of oral hypoglycaemics. By the end of the study the daily dosage of glucose-lowering drugs was decreased by 15% on an average, as compared to baseline (p < 0.05). Nobody of Allicor-treated patients discontinued the study.
In placebo group, no significant changes in lipid levels were observed (Table 1). There were no significant changes in fasting blood glucose and serum fructosamine levels, as well (Table 2). None of patients in placebo group discontinued the study.
Discussion
Garlic-based preparations are generally supposed to be effective in atherosclerosis prevention [8]. Garlic-based preparations are known to reduce serum cholesterol levels in humans, inhibit cholesterol biosynthesis, suppress low density lipoprotein (LDL) oxidation, lower plasma fibrinogen and increase fibrinolytic activity, and thus to possess antiatherosclerotic properties [7, 11–14]. Garlic contains a variety of organosulfur compounds, amino acids, vitamins and minerals [15]. Some of the sulfur-containing compounds such as allicin, ajoene, S-allylcysteine, S-methylcysteine, diallyl disulfide and sulfoxides may be responsible for antiatherosclerotic activity of garlic [14, 16, 17]. However, little is known on the possible beneficial effects of garlic-based preparations in type 2 diabetes mellitus, one of the major risk factors of premature atherosclerosis development.
Late complications of diabetes mellitus include various syndromes associated with damage to large and small arteries, i.e., micro- and macroangiophaties. It was suggested that macroangiophaties result from atherosclerosis [2], although some pathomorphological alterations typical especially for diabetes mellitus have been described [18]. Premature development and accelerated progression of atherosclerosis are the specific features of diabetes mellitus, as was confirmed by epidemiological studies [19–21]. Hyperglycemia occurring in diabetes mellitus leads to an increase in the concentration of the non-enzymatic glycosylation products in circulation [22]. Non-enzymatic glycosylation of proteins is a cascade of chemical reactions yielding stable covalent bonds between glucose molecule and free amino groups of protein. Enhanced glycosylation in diabetes mellitus can lead to the formation of modified atherogenic LDL as well as advanced glycation end products, including glycated collagen in arterial wall, the factors that could be attributed to accelerated atherogenesis in diabetics. Particularly, it is known that non-enzymatic glycosylation impairs LDL metabolism, which manifests as a reduced affinity of LDL to the classical LDL-receptor [23], lower rate of LDL clearance from blood plasma [24], increased LDL uptake by macrophages [25], enhanced covalent binding of LDL to the connective tissue matrix of the vessel wall [26] and generation of free radicals participating in oxidative damage to lipid and proteins moieties of a lipoprotein particle [27]. It is quite obvious that improved metabolic control in diabetic patients can lead to the reduction in non-enzymatic glycosylation and therefore decrease biochemical risk for atherosclerosis development and progression [28].
The possibility of glucose-lowering effects of garlic was supported experimentally in the number of studies. The first report considering the beneficial effects of allicin, biologically active sulphoxide from garlic, in alloxan-induced diabetic mice was published as far back as in 1973 [29]. Further studies have demonstrated that sulphur-containing amino acids from garlic possess a direct hypoglycaemic action, potentiate the effects of insulin in blood serum and increase the hepatic glycogen synthesis in alloxan-induced diabetes in mice and rabbits [30–34]. Additionally, garlic constituents decreased significantly the concentration of serum lipids, blood glucose and activities of serum enzymes like alkaline phosphatase, acid phosphatase and lactate dehydrogenase and liver glucose-6-phosphatase [35, 36]. Treatment of alloxan diabetic rats with the antioxidant S-allyl cysteine sulfoxide isolated from garlic, ameliorated the diabetic condition almost to the same extent, as did glibenclamide and insulin. In addition, S-allyl cysteine sulfoxide controlled lipid peroxidation and significantly stimulated in vitro insulin secretion from B cells isolated from normal rats [37]. The effectiveness of garlic-based preparations was also demonstrated in streptozotocin-induced diabetes in mice and rats [38–41].
So, the anti-diabetic action of garlic established in animal studies provided a background for further investigations concerning possible clinical implications for garlic-based preparations. However, the use of garlic compounds as antidiabetic remedies in clinical practice is not well recognized, although dried garlic is widely used in traditional medicine of many cultures in the treatment of diabetes mellitus. There are few clinical data on the effects of garlic in the improvement of metabolic control in diabetic patients. The results of the clinical study performed in South-East Asia more than 15 years ago were first to demonstrate the effectiveness of garlic in diabetes mellitus [42]. The beneficial effects of garlic-based dietary supplement in diabetes were also supported in a recent study by Melchinskaya et al. [43].
This study seems to be the first placebo-controlled trial aimed to estimate the effects of garlic-based drug on the parameters of metabolic control and plasma lipids in type 2 diabetes mellitus. In patients receiving monotherapy with Allicor, time-released garlic powder tablets, fasting blood glucose level tended to decrease. More remarkably, serum fructosamine that is considered to be a reliable and stable measure of long-term compensation of metabolic control, decreased significantly. Similar results were obtained in patients receiving Allicor along with continuing treatment with oral hypoglycaemics. Additionally, Allicor treatment resulted in substantial decrease in serum triglycerides in both groups of patients. It is possible that the decrease in serum triglycerides was due to better metabolic control that is characterized by the inhibition of lipolysis and decrease of hepatic production of very low-density lipoprotein. The improvement of lipid profile is generally considered to reduce cardiovascular risk, and serum triglyceride level is used as significant variable Cox proportional hazards model for 10-year prognostic risk of fatal or non-fatal myocardial infarction and sudden death derived from PROCAM study [44]. On the other hand, hypertriglyceridemia is the common pattern of dyslipidemia in type 2 diabetics. The observed reduction of serum triglycerides may also be related to antioxidant action of biologically active compounds from garlic that may inhibit generation of free radicals and stimulate catalase, superoxide dismutase and glutathione peroxidase activities [45], so that they might increase insulin sensitivity in peripheral and hepatic cells via the inhibition of lipid peroxidation in cell membranes. Thus, glucose-lowering and triglyceride-lowering effects of garlic may be possibly due to its peripheral action through the lowering of insulin resistance in target tissues.
It is notable that in diabetic patients receiving the combined therapy with Allicor and oral hypoglycaemics the moderate but statistically significant reduction in the daily dosage of glucose-lowering drugs occurred. This can be regarded as an additional beneficial effect of Allicor, since sulfonylurea derivatives may possess some unfavorable side effects that can be regarded as proatherogenic. It has been shown that oral hypoglycaemics produce a direct proatherogenic effect in cultured cells, inducing a substantial intracellular cholesterol accumulation [46]. So, the use of minimally possible dose of antidiabetic drugs to sustain adequate metabolic control is theoretically and experimentally justified and may be the rationale for Allicor assignment for complex therapy of type 2 diabetes mellitus.
By far, a lot of garlic-based products are present in the market now. They can be generally classified into four groups, i.e., garlic essential oil, garlic oil macerate, garlic powder and garlic extract. The manufacturing process can markedly influence the composition of garlic product, thus sulfur-containing compounds in garlic preparations may vary greatly. As compared to other garlic preparations, dehydrated garlic powder is thought to retain the same ingredients as raw garlic, both water-soluble and organic-soluble, although the proportion and amount of various constituents may differ significantly [47, 48]. Allicor contains just garlic powder; on the other hand, it possesses a prolonged mode of action, as its biological effect lasts for 12–16 h after single-dose administration [49, 50]. So, Allicor differs greatly from other garlic-based preparations and may have considerable benefits in medicinal use.
The results of this study may allow recommending garlic powder tablets for the treatment of type 2 diabetes mellitus along with dietary treatment and/or sulfonylurea derivatives to achieve better metabolic control. Additional benefits from garlic-based dietary supplements may include the substantial reduction of serum triglycerides (major lipid characteristic of an atherogenic lipid profile in diabetic patients), thus resulting in the decrease of cardiovascular risk. The other known effects of garlic preparations (e.g., inhibition of cholesterol biosynthesis, suppression of low-density lipoprotein oxidation, lowering plasma fibrinogen and increasing fibrinolytic activity) can also play angioprotective role.
References
Krolewski AS, Warram JH, Valsania P, Martin BC, Laffel LM, Christlieb AR (1991) Evolving natural history of coronary artery disease in diabetes mellitus. Am J Med 90:56S–61S
Burchfiel CM, Reed DM, Marcus EB, Strong JP, Hayashi T (1993) Association of diabetes mellitus with coronary atherosclerosis and myocardial lesions. An autopsy study from the Honolulu Heart Program. Am J Epidemiol 137:1328–1340
Schwartz CJ, Valente AJ, Sprague EA (1993) A modern view of atherogenesis. Am J Cardiol 71:9B–14B
Pyorala K, Laakso M, Uusitupa M (1987) Diabetes and atherosclerosis: an epidemiologic view. Diabetes Metab Rev 3:463–524
Nesto R (2001) CHD: a major burden in type 2 diabetes. Acta Diabetol 38(1):S3–S8
Swanston-Flatt SK, Flatt PR, Day C, Bailey CJ (1991) Traditional dietary adjuncts for the treatment of diabetes mellitus. Proc Nutr Soc 50:641–651
Harenberg J, Giese C, Zimmermann R (1988) Effect of dried garlic on blood coagulation, fibrinolysis, platelet aggregation and serum cholesterol levels in patients with hyperlipoproteinemia. Atherosclerosis 74:247–249
Berthold HK, Sudhop T (1998) Garlic preparations for prevention of atherosclerosis. Curr Opin Lipidol 9:565–569
Wang HX, Ng TB (1999) Natural products with hypoglycemic, hypotensive, hypocholesterolemic, antiatherosclerotic and antithrombotic activities. Life Sci 65:2663–2677
Kruse-Jarres JD, Jarausch J, Lehmann P, Vogt BW, Rietz P (1989) A new colorimetric method for the determination of fructosamine. Lab Med 13:245–253
Bordia AK, Joshi HK, Sanadhya YK, Bhu N (1977) Effect of essential oil of garlic on serum fibrinolytic activity in patients with coronary artery disease. Atherosclerosis 28:155–159
Lau B, Lam F, Wang-Chen R (1987) Effect of odor-modified garlic preparation on blood lipids. Nutr Res 7:139–149
Phelps S, Harris WS (1993) Garlic supplementation and lipoprotein oxidation susceptibility. Lipids 28:475–477
Campbell JH, Efendy JL, Smith NJ, Campbell GR (2001) Molecular basis by which garlic suppresses atherosclerosis. J Nutr 131:1006S–1009S
Block E (1985) The chemistry of garlic and onions. Sci Am 252:114–119
Orekhov AN, Tertov VV (1997) In vitro effect of garlic powder extract on lipid content in normal and atherosclerotic human aortic cells. Lipids 32:1055–1060
Yeh YY, Liu L (2001) Cholesterol-lowering effect of garlic extracts and organosulfur compounds: human and animal studies. J Nutr 131:989S–993S
Ledet T, Rasmussen LM, Heickendorff L, Barfod K, Thogersen VB (1990) The nature of large vessel disease in diabetes mellitus. J Diabet Complications 4:63–65
Koskinen SV, Reunanen AR, Martelin TP, Valkonen T (1998) Mortality in a large population-based cohort of patients with drug-treated diabetes mellitus. Am J Public Health 88:765–770
Goraya TY, Leibson CL, Palumbo PJ (2002) Coronary atherosclerosis in diabetes mellitus: a population-based autopsy study. J Am Coll Cardiol 40:946–953
Nesto RW, Rutter MK (2002) Impact of the atherosclerotic process in patients with diabetes. Acta Diabetol 39(2):S22–S28
Koskinen P, Irjala K, Viikari J, Panula O, Matikainen MT (1987) Serum fructosamine in the assessment of glycaemic control in diabetes mellitus. Scand J Clin Lab Invest 47:285–292
Witztum JL, Mahoney EM, Branks MJ, Fisher M, Elam R, Steinberg D (1982) Nonenzymatic glucosylation of low-density lipoprotein alters its biologic activity. Diabetes 31:283–291
Wiklund O, Witztum JL, Carew TE, Pittman RC, Elam RL, Steinberg D (1987) Turnover and tissue sites of degradation of glucosylated low density lipoprotein in normal and immunized rabbits. J Lipid Res 28:1098–1109
Witztum JL, Koschinsky T (1989) Metabolic and immunological consequences of glycation of low density lipoproteins. Prog Clin Biol Res 304:219–234
Brownlee M, Vlassara H, Cerami A (1985) Nonenzymatic glycosylation products on collagen covalently trap low-density lipoprotein. Diabetes 34:938–941
Bucala R, Makita Z, Koschinsky T, Cerami A, Vlassara H (1993) Lipid advanced glycosylation: pathway for lipid oxidation in vivo. Proc Natl Acad Sci USA 90:6434–6438
Brownlee M (2001) Biochemistry and molecular cell biology of diabetic complications. Nature 414:813–820
Mathew PT, Augusti KT (1973) Studies on the effect of allicin (diallyl disulphide-oxide) on alloxan diabetes. I. Hypoglycaemic action and enhancement of serum insulin effect and glycogen synthesis. Indian J Biochem Biophys 10:209–212
Jain RC, Vyas CR, Mahatma OP (1973) Hypoglycaemic action of onion and garlic. Lancet 2:1491
Jain RC, Vyas CR (1974) Hypoglycaemia action of onion on rabbits. Br Med J 2:730
Jain RC, Vyas CR (1975) Garlic in alloxan-induced diabetic rabbits. Am J Clin Nutr 28:684–685
Augusti KT, Mathew PT (1975) Effect of allicin on certain enzymes of liver after a short term feeding to normal rats. Experientia 31:148–149
Begum H, Bari MA (1985) Effect of garlic oil on the pancreas of experimental diabetes in guineapigs. Bangladesh Med Res Counc Bull 11:64–68
Sheela CG, Augusti KT (1992) Antidiabetic effects of S-allyl cysteine sulphoxide isolated from garlic Allium sativum Linn. Indian J Exp Biol 30:523–526
Sheela CG, Kumud K, Augusti KT (1995) Anti-diabetic effects of onion and garlic sulfoxide amino acids in rats. Planta Med 61:356–357
Augusti KT, Sheela CG (1996) Antiperoxide effect of S-allyl cysteine sulfoxide, an insulin secretagogue, in diabetic rats. Experientia 52:115–120
Farva D, Goji IA, Joseph PK, Augusti KT (1986) Effects of garlic oil on streptozotocin-diabetic rats maintained on normal and high fat diets. Indian J Biochem Biophys 23:24–27
Swanston-Flatt SK, Day C, Bailey CJ, Flatt PR (1990) Traditional plant treatments for diabetes. Studies in normal and streptozotocin diabetic mice. Diabetologia 33:462–464
Ohaeri OC (2001) Effect of garlic oil on the levels of various enzymes in the serum and tissue of streptozotocin diabetic rats. Biosci Rep 21:19–24
Patumraj S, Tewit S, Amatyakul S (2000) Comparative effects of garlic and aspirin on diabetic cardiovascular complications. Drug Deliv 7:91–96
Sitprija S, Plengvidhya C, Kangkaya V, Bhuvapanich S, Tunkayoon M (1987) Garlic and diabetes mellitus phase II clinical trial. J Med Assoc Thai 70(2):223–227
Melchinskaya EN, Popovtseva ON, Gromnatskii NI (1997) Immunologic aspects of alisate in diabetes mellitus patients. Biull Eksp Biol Med 124:595–597
Assmann G, Cullen P, Schulte H (2002) Simple scoring scheme for calculating the risk of acute coronary events based on the 10-year follow-up of the prospective cardiovascular Münster (PROCAM) study. Circulation 105(3):310–315
Ide N, Lau BH (1999) Aged garlic extract attenuates intracellular oxidative stress. Phytomedicine 6:125–131
Sobenin IA, Maksumova MA, Slavina ES, Balabolkin MI, Orekhov AN (1994) Sulfonylureas induce cholesterol accumulation in cultured human intimal cells and macrophages. Atherosclerosis 105:159–163
Iberl B, Winkler G, Miller B, Knobloch K (1990) Quantitative determination of allicin and alliin from garlic by HPLC. Planta Med 56:320–326
Amagase H, Petesch BL, Matsuura H, Kasuga S, Itakura Y (2001) Intake of garlic and its bioactive components. J Nutr 131:955S–962S
Orekhov AN, Tertov VV, Sobenin IA, Pivovarova EM (1995) Direct anti-atherosclerosis-related efects of garlic. Ann Med 27:63–65
Orekhov AN, Grunwald J (1997) Effects of garlic on atherosclerosis. Nutrition 13:656–663
Acknowledgments
The authors thank the participants of this study for their time, effort and support. This work was supported with grant from the Institute for Atherosclerosis Research, Moscow, Russia.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Sobenin, I.A., Nedosugova, L.V., Filatova, L.V. et al. Metabolic effects of time-released garlic powder tablets in type 2 diabetes mellitus: the results of double-blinded placebo-controlled study. Acta Diabetol 45, 1–6 (2008). https://doi.org/10.1007/s00592-007-0011-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00592-007-0011-x