
Abstract
Lateral unicompartment knee replacements are performed infrequently in the United Kingdom. This study evaluates the experience of two knee surgeons in a District General Hospital for all lateral unicompartmental arthroplasties performed between October 2007 and August 2011. Two different implants were used in this time period, the Oxford domed and the Zimmer fixed-bearing system. Twenty-seven procedures were completed in this time span (15 Oxford domed and 12 Zimmer fixed bearing), all of which once completed were followed up and 21 patients completed an Oxford knee score. Average Oxford knee scores were 36.6 (95 % CI 29.0–44.2) for the Oxford domed prosthesis and 28.6 (19.8–37.5) for the Zimmer fixed-bearing prosthesis (p = 0.15). One patient with an Oxford domed prosthesis required revision for bearing dislocation. The follow-up Oxford knee scores support the use of this technique as an alternative to total knee replacement but with no significant difference in functional outcome. Our results, however, may encourage a more cautious approach to the use of a mobile-bearing prosthesis in favour of a fixed-bearing prosthesis.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Since its introduction in the 1970s, the use of unicompartmental knee replacements (UKR) has remained contentious. In osteoarthritis, lone medial tibiofemoral compartment is much more common than lateral compartment degeneration [11]. There is increasing evidence for the use of medial compartment knee replacements as an alternative to total knee replacements (TKR) in isolated medial compartment osteoarthritis. Though there is a lack of large randomised controlled trials comparing UKRs to TKRs, pooled results from small randomised controlled studies and case controlled studies show that there is an increase in knee function when an unicompartmental prosthesis is used [6] and the implants have an 85–97 % 5-year survival rate [8, 15, 18]. In the UK, 6,257 unicompartmental knee replacements were completed in 2011. This was 8 % of the number of total knee replacements completed [13].
Due to the relative rarity of isolated lateral compartment osteoarthritis, the lateral UKR has even less supporting evidence for its use. Of the unicompartment knee replacements completed in the UK, only 6 % were lateral unicompartment replacements (2052 of the 32,847 reported the National Joint registry before December 2010) [1]. It has been suggested that centres performing fewer than 23 of these procedures per year will have significantly poorer medium term results than centres performing more than this [16]. In addition, it has been noted that complications tend to occur with this procedure in the early to medium term, though this has been suggested to be mainly a result of poor patient selection rather than prosthesis failure [9, 12, 18].
The Royal Gwent Hospital is a medium-sized District General Hospital (DGH) in South-East Wales. It has approximately 774 beds with elective orthopaedic operations also being performed in the nearby trauma and orthopaedic unit in St Woolos Hospital and St Joseph’s Hospital. Two senior knee surgeons (MWL and WMC) have been undertaking lateral unicompartment knee replacements between these 3 sites.
Two prosthesis are used in our department and thus have been included in this study. These are shown in Fig. 1. The first is the Oxford domed Lateral mobile-bearing prosthesis (Biomet UK, Bridgend). The tibial and femoral components of this prosthesis are made from a cast cobalt chromium molybdenum alloy. The meniscal bearing is constructed from a high molecular weight polyethylene. The bearing has a biconcave spherical design to minimise impingement and reduce the chance of bearing dislocation [19]. The alternative prosthesis was a Zimmer unicompartmental high flex knee system (Zimmer, Indiana), which is the latest prosthesis based on the M/G design. It has a round on flat articulation with a net-shape polyethylene articular surface designed to improve rollback and allow flexion to 155° [2].

Prostheses used in this study. a Zimmer unicompartmental high flex knee system (Zimmer, Indiana). b Oxford domed Lateral mobile-bearing prosthesis (Biomet UK, Bridgend)
The purpose of this study is to answer the question: what are the outcomes following lateral compartment replacement in our DGH? Knowledge of these outcomes would allow comparison to larger centres and also to other series of total knee replacements in similar patients. Evaluation is completed using complication and revision rate, and also with functional outcome scoring.
The design of the study is a retrospective analysis of outcomes of all patients undergoing lateral unicompartment replacement. The primary outcome is complication rate and revision rate, and individuals in the cohort were also contacted by telephone to obtain functional scoring (Fig. 2).

Post-operative radiographs. a, b Zimmer fixed bearing, c, d Oxford mobile bearing
Patients and methods
All patients who received lateral UKR between October 2007 and August 2011 were reviewed. During this period, UKRs were completed by one of two knee surgeons (MWL or WMC) working at a DGH using either the Oxford phase III domed prosthesis (Biomet, Bridgend) or the fixed-bearing high flex knee system (Zimmer, Indiana). All patients had isolated lateral tibiofemoral compartment arthritis at arthroscopy with clinical symptoms sufficient to warrant a knee replacement.
The surgical approach was via a lateral parapatellar incision. The tibial cut was completed using an extramedullary jig with conservative bone resection. Femoral cuts were made at a 6° valgus position using an intra-medullary jig. The tibial and femoral components were sized and trialled intra-operatively to give optimum coverage. Flexion and extension gaps were then confirmed to be equal with parallel joint lines. A trial reduction with insert was completed to ensure good soft tissue tension and alignment through full range of movement. Finally, components were cemented, and closure was in layers with subcutaneous vicryl to skin.
Complication and revision rates were obtained from patient notes. Patients were contacted by telephone and asked to complete an Oxford knee score [3] to measure their functional outcome. Patients were also asked to complete a subjective score about how satisfied they were with the procedure, with 0 being very unsatisfied and 10 being completely satisfied.
Results
Between 1/10/2007 and 1/8/2011, 27 lateral UKRs were completed. No patients were lost to follow-up and 22 (81.2 %) completed an Oxford knee score. The patient demographics are summarised in Table 1. The mean follow-up at review was 34.7 months (minimum 15.1 months, maximum 60.1 months). Twelve (44 %) of the UKR completed were with the Oxford domed prosthesis, and 15 (56 %) were the Zimmer fixed bearing. Average age at operation was 57.8 years. The average number of knees replaced was 5.4 per year with spread shown in Table 2. An average number of 2.4 Oxford domed prostheses were used per year, and 3.0 Zimmer fixed-bearing prostheses were implanted per year (p = 0.68).
The complication rate for lateral unicompartmental knee replacements was 4/27 (15 %) with a total revision rate of 1/27 (4 %).
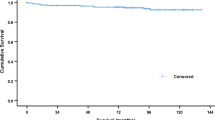
There were no implant or wound infections. Of the 12 Oxford domed procedures, 2 have required a further procedure (1 patient dislocated the bearing requiring a revision and 1 patient required a manipulation under anaesthetic). This revision results in a calculated relative survival of this implant at 4 years of 0.90 as shown in Fig. 3. In the 15 fixed-bearing Zimmer procedures, 1 patient who is on warfarin required aspiration for a haemarthrosis on three occasions. His OKS at follow-up was 19. One patient was in the process of being investigated for unexplained knee pain when contacted to complete his OKS. His Oxford knee score was 5 and reported that his lateral unicompartment implant was “good for 6 months”. He has since been followed up again and diagnosed with a medial meniscal tear. He has accepted the level of function with his knee and is currently awaiting second side surgery.

Survival curves for the two implants
The functional outcome parameters are shown in Table 3. There is no significant difference in scores between those having received an Oxford domed prosthesis compared to those who had received a Zimmer fixed-bearing prosthesis. Average Oxford knee score is 39.1 for all knees, and average satisfaction score is 7.3 out of 10 for all knees.
Discussion
This study demonstrates the experience with lateral unicompartment knee replacement from a DGH. Overall, the results are good, with few complications and high Oxford knee scores in patients with Oxford domed or Zimmer fixed-bearing prosthesis. Most patients had good knee function at follow-up, though 23 % had severe knee symptoms, as defined by the Oxford knee scores. There was no significant difference in function or subjective scoring between the patients who had received a domed or fixed-bearing implant. The failure rate was higher in the domed prosthesis group, with a single bearing dislocation requiring revision.
A recent retrospective analysis of the UK National Joint Registry has revealed that the 7-year revision and complication rate appears to be similar between unicompartmental replacements placed in either medial or lateral compartments. It also suggests that the revision rate is not associated with device selection with either mobile or fixed bearing [1].
Dislocation of the bearing is a recognised complication of unicompartmental knee replacements, and one that has required the design of the Oxford domed prosthesis to be revised three times. The dislocation rate for the phase III implant, as used in this study, is quoted to be 1.7 % [14]. This rate is from the Oxford group who were integral to the design of the prosthesis, and earlier designs had a higher dislocation rate of 11 % [7]. This difference has been attributed to both prosthesis design and improvements in surgical technique. Our dislocation rate in this series is 8 %, which is most likely due to the smaller sample size evaluated in this study. However, it is concerning, as it has considerable impact on the patient but was our only cause for revision.
One other study is available which has compared the use of mobile-bearing to fixed-bearing prostheses in lateral unicompartmental arthroplasty [5]. This study evaluated 30 knee arthroplasties in 28 patients using a Preservation mobile- or fixed-bearing prosthesis. No significant difference in the Oxford knee score or range of movement measures was reported at a 2-year follow-up. However, they had a 23 % revision rate in the mobile-bearing group, all due to tibial component loosening. There is a lack of consensus as to which type of implant is superior, as mimicked in the literature in medial compartment unicompartment arthroplasty. In a recent meta-analysis, no difference was found between complication rates or functional outcomes between mobile-bearing implants and fixed-bearing implants [17].
In this study, there are some methodological weaknesses. These mainly relate to the relative rarity of the procedure, which has a direct bearing on the numbers available for analysis. For this reason, the study could only be completed as an observational cohort rather than a more powerful randomised controlled trial. The low numbers included inhibit making firm assertions regarding the comparison of the two implants, but the general trend is of good results both functionally and in revision rates. A power calculation has not been included as we had no preceding data to calculate power prospectively, and the design was to collect as many patients as possible. However, a retrospective power calculation shows that this study has a power of 50 % [4].
Unfortunately, further limits are placed on the direct comparison of fixed- and mobile-bearing prosthesis due to a lack of pre-operative metrics that can be presented here. As there are no pre-operative knee function scores, it is impossible to be sure that the two groups receiving different implants were comparable.
It has been suggested that the use of a mobile-bearing implant closer mimics the natural kinematics of the knee and thus makes a superior implant. Evidence for this belief is found in radiological evidence which shows a significantly lower incidence of radiolucent lines developing in patients with Oxford mobile-bearing medial unicompartment replacements than with Miller-Galante fixed-bearing prostheses [10]. However, this theoretical advantage does not seem to be demonstrated in the available follow-up data, as both mobile-bearing and fixed-bearing prostheses show good follow-up results. It is possible that an advantage will be seen in the longer term as the improved kinematics will reduce the progression of arthritis over time. This theoretical advantage is tempered by the increased failure rate. Though this increased failure rate is not statically significant in this study (p = 0.44), it is still concerning and has resulted in a local preference for fixed-bearing prostheses.
It must be noted that these results are from a large DGH and the surgeons involved are experienced in completing medical compartment unicompartmental knee replacements. In the study time period, the senior author completed 194 medial unicompartment replacements alongside the 15 lateral unicompartmental replacements. Lateral unicompartmental knee replacements are more technically demanding than the medial counterparts and so should not be attempted by persons who complete infrequent medial unicompartmental replacements.
Conclusions
We conclude that functional and subjective scores from patients receiving lateral unicompartmental knee replacements are good, and this procedure represents a valid alternative to total knee replacements in isolated lateral compartment osteoarthritis. We do not have any evidence as to the superiority of fixed-bearing or mobile-bearing devices, but we do note that the dislocation had significant impact on the patient involved; therefore, we advise caution when selecting the use of a domed prosthesis.
References
Baker PN, Jameson SS, Deehan DJ, Gregg PJ, Porter M, Tucker K (2012) Mid-term equivalent survival of medial and lateral unicondylar knee replacement: an analysis of data from a National Joint Registry. J Bone Joint Surg Br 94:1641–1648
Berger RA, Nedeff DD, Barden RM, Sheinkop MM, Jacobs JJ, Rosenberg AG, Galante JO (1999) Unicompartmental knee arthroplasty. Clinical experience at 6- to 10-year followup. Clin Orthop Relat Res 50–60
Dawson J, Fitzpatrick R, Murray D, Carr A (1998) Questionnaire on the perceptions of patients about total knee replacement. J Bone Joint Surg Br 80:63–69
DSS Research (2013) Power calculator. https://www.dssresearch.com/KnowledgeCenter/toolkitcalculators/statisticalpowercalculators.aspx. Accessed 18 June 2013
Forester M, Bauze A, Keen G (2007) Lateral unicompartment knee replacement; fixed or mobile bearing? Knee Surg Sports Traumatol Arthrosc 15:1107–1111
Griffin T, Rowden N, Morgan D, Atkinson R, Woodruff P, Maddern G (2007) Unicompartmental knee arthroplasty for the treatment of unicompartmental osteoarthritis: a systematic study. ANZ J Surg 77:214–221
Gunther TV, Murray DW, Miller R, Wallace DA, Carr AJ, O’Connor JJ, McLardy-Smith P, Goodfellow JW (1996) Lateral unicompartmental arthroplasty with the Oxford meniscal knee. Knee 3:33–39
Kuipers BM, Kollen BJ, Bots PCK, Burger BJ, Van Raay JJAM, Tulp NJA, Verheyen CCPM (2010) Factors associated with reduced early survival in the Oxford phase III medial unicompartment knee replacement. Knee Elsevier BV 17:48–52
Kumar AU, Fiddian NJ (1999) Medial unicompartmental arthroplasty of the knee 1998–2000
Li M, Yao F, Ioppolo J, Nivbrant B, Wood D (2006) Mobile vs. fixed bearing unicondylar knee arthroplasty: a randomized study on short-term clinical outcomes and knee kinematics. Knee 13:365–370
McAlindon TE, Snow S, Cooper C, Dieppe PA (1992) Radiographic patterns of osteoarthritis of the knee joint in the community: the importance of the patellofemoral joint. Ann Rheum Dis 51:844–849
Murray DW, Goodfellow JW, Connor JJO (1998) The Oxford medial unicompartmental arthroplasty. J Bone Joint Surg Br 80:983–989
National Joint Registry for England and Wales (2012) 9 annual report. Porter M, Borroff M, Gregg P, Howard P, MacGregor A, Tucher K (eds) National Joint Registry for England and Wales, Hemel Hempstead
Pandit H, Jenkins C, Beard DJ, Price AJ, Gill HS, Dodd CAF, Murray DW (2010) Mobile bearing dislocation in lateral unicompartmental knee replacement. Knee Elsevier BV 17:392–397
Pandit H, Jenkins C, Gill HS, Barker K, Dodd CAF, Murray DW (2011) Minimally invasive Oxford phase 3 unicompartmental knee replacement: results of 1000 cases. J Bone Joint Surg Br 93:198–204
Robertsson O, Knutson K, Lewold S, Lidgren L (2001) The routine of surgical management reduces failure after unicompartmental knee arthroplasty. J Bone Joint Surg Br 83:45–49
Smith TO, Hing CB, Davies L, Donell ST (2009) Fixed versus mobile bearing unicompartmental knee replacement: a meta-analysis. Orthop Traumatol Surg Res 95:599–605
Svärd UC, Price AJ (2001) Oxford medial unicompartmental knee arthroplasty. A survival analysis of an independent series. J Bone Joint Surg Br 83:191–194
Van Duren BH, Gallagher J, Pandit H, Beard D, Dodd C, Gill HS, Murray D (2009) EFORT—European federation of national associations of orthopaedics and traumatology (8th congress): a new domed tibial lateral component provides improved range of movement and retains normal kinematics for the oxford UKR. J Bone Joint Surg Br 91-B:47–48
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Marson, B., Prasad, N., Jenkins, R. et al. Lateral unicompartmental knee replacements: early results from a District General Hospital. Eur J Orthop Surg Traumatol 24, 987–991 (2014). https://doi.org/10.1007/s00590-013-1277-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00590-013-1277-z