
Abstract
The microsurgical approach for removal of prolapsed lumbar disc has gained popularity because of its various advantages. Localisation of the correct level is vital for the success of this procedure. We performed an audit to review our practice regarding the localisation of correct level in lumbar microdiscectomy. Twenty-eight patients were included in this study. Nearly, two-third of the patients had needles as pre-operative marker of localisation and in more than 50% the needle was inserted perpendicular to the floor. When using a needle to localise the spinal level, care should be taken to insert it perpendicular to the floor or parallel to the disc space to avoid approaching the wrong level. The gold standard is an intraoperative lateral fluoroscopy of the spine with a marker in the disc space.
Résumé
L’abord microchirurgical pour l’ablation des prolapsus discaux lombaires a gagné en popularité de par ses nombreux avantages. Le repérage exact du niveau est indispensable au succès. Nous avons réalisé un audit pour revoir notre pratique concernant ce repérage lors de la discectomie microchirurgicale. Vingt huit patients ont été inclus dans cette étude. Environ deux tiers des patients avaient eu une implantation d’aiguille en marquage pré-opératoire et dans plus de 50% des cas, cette aiguille avait été placée perpendiculairement par rapport au sol. Lorsque l’on utilise ce procédé, il faut faire attention de bien placer l’aiguille perpendiculairement par rapport au sol ou bien de façon parallèle au disque, pour éviter toute erreur de niveau. Le « gold standard » consiste à utiliser un contrôle fluoroscopique per-opératoire du rachis avec un marquage de l’espace discal.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Lumbar microdiscectomy is one of the commonly performed surgical procedures for patients with lumbar disc prolapse. Caspar [2] and Williams [14] initially reported the technique of lumbar microdiscectomy. It offers various advantages which include a smaller incision, less soft tissue dissection and consequently reduced postoperative pain, shorter hospital stay and early return to work.
However, the success of the procedure depends on various factors which include the right procedure for the right patient at the right level. The cost of unsatisfactory outcome is substantial, both to the patient in terms of quality of life and lost income and to health service providers in terms of financial costs and subsequent treatment [4]. Although, a wide range of surgical techniques for this procedure have been reported, relatively little attention has been paid to methods of identifying the correct level while performing the procedure. This is more relevant in this day and age because of increasing medico legal litigation. We performed a prospective audit to review our practice regarding the localisation of correct level in lumbar microdiscectomy. This article describes the outcome of our study.
Materials and methods
Twenty-eight patients who had lumbar microdiscectomy at Leeds General Infirmary between November 2004 and March 2005 were included in the study. A standard audit form was devised. Parameters analysed included the grade of operating surgeon, type of marker used, pre-operative (initial) fluoroscopy, method of localisation, direction of needle, need for further intraoperative fluoroscopy and duration of the operation.
Males predominated in our study (57%) and majority were in the 31–40 age group. The procedure was performed by higher surgical trainees in 69% of the patients. Needles were used as a marker of pre-operative localisation in 23 patients while the level was localised clinically in five patients. In the former group, 10 patients had needle inserted to the laminae above and below the pathological disc space, eight patients to the corresponding spinous process and in four patients, the needle was inserted in the direction of the disc space. In 57% of the patients, the needle was inserted perpendicular to the floor; in 23% it was parallel to the disc space while in the rest the direction of the needle was not perpendicular to the floor or parallel to the disc space.
Results
In seven patients the surgeons were absolutely sure of the pre-operative localisation and no further imaging was done intraoperatively. In four patients, the surgeons were sure of the correct level after initial fluoroscopy but further intraoperative fluoroscopy was performed for confirmation. In 16 patients, the surgeons were not sure of the pre-operative spinal level and chose to perform additional intra operative fluoroscopy. In one patient a wrong level was approached in spite of pre-operative fluoroscopy. However, this was corrected intraoperatively. In patients where the needle was not perpendicular, repeated fluoroscopic images had to be done to confirm the level. The duration of the procedure was longer by a mean of 30 min in patients where pre-operative fluoroscopy was done than in patients who did not have initial fluoroscopy to confirm the level.
Discussion
The primary rationale for surgery in any form of disc prolapse is to relieve nerve root irritation or compression caused by herniated disc material. The surgical management of lumbar disc herniation has evolved considerably since Mixter and Barr [11] described the treatment of ruptured intervertebral disc prolapse. Though there are several different techniques and hints about the procedure itself [1, 3, 5–10, 12, 13, 15, 16] there have been very few studies reviewing the methods of localising the correct level.
Localisation to provide guidance during surgery can be done with the use of a variety of pre-operative and intraoperative imaging methods which include plain radiographs, computed tomography (CT) and magnetic resonance imaging (MRI). The common methods used are skin markers, needles or methylene blue dye to locate the correct level with the help of fluoroscopy. Woodard et al. [17] have reported the use of intraoperative MRI in spinal surgery in a series of 12 patients.
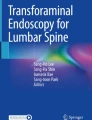
In our series, needles were preferred in more than two-third of the patients. While using needles, the direction of insertion is very important. Care should be taken to ensure that the needle is perpendicular to the floor or parallel to the disc space to avoid misinterpretation of the level. Insertion of the needle at an angle (Fig. 1) can be very misleading to the surgeon resulting in surgery at a wrong level. Twenty percent of patients had pre-operative localisation with needles that were not perpendicular to the floor. This necessitated repeated fluoroscopic images to identify the correct level with consequent increased exposure to radiation.

Radiograph with arrows showing the methods of localisation of correct level in lumbar microdiscectomy. (a) Correct method of needle insertion parallel to disc space (b) Incorrect method of needle insertion which is not parallel to the disc space
In one patient a wrong level was approached in spite of initial fluoroscopy. However, this was identified intraoperatively and corrected. This highlights the fact that in spite of pre-operative methods done to localise the level, rare instances of wrong level may still occur. We therefore suggest that an intraoperative lateral fluoroscopy of the lumbar spine, with a marker in the disc space, should be routinely performed to confirm that surgery is being done at the right level.
Conclusion
The identification of correct spinal level is important in lumbar microdiscectomy. Needles when used should be inserted perpendicular to the floor or parallel to the disc space. Intraoperative lateral fluoroscopic image with a marker in the disc space should always be obtained to ensure correct localisation of the level.
References
Brody F, Rosen M, Tarnoff M, et al (2002) Laparoscopic lateral L4–5 disc exposure. Surg Endosc 16:650–653
Caspar W (1977) A new surgical procedure for lumbar disc herniation causing less tissue damage through a microsurgical approach. Adv Neurosurg 4:74–80
Deen HG (2002) Posterolateral endoscopic excision for lumbar disc herniation: surgical technique, outcome, and complications in 307 consecutive cases. Spine 15:2081–2082
Dolan P, Greenfield K, Nelson RJ, et al (2000) Can exercise therapy improve the outcome of Microdiscectomy? Spine 25(12):1523–1532
Haines SJ, Jordan N, Boen JR, et al (2002) Discectomy strategies for lumbar disc herniation: study design and implications for clinical research. J Clin Neurosci 9:440–446
Javedan S, Sonntag VK (2003) Lumbar disc herniation: microsurgical approach. Neurosurgery 52:160–162
Javid MJ (1995) Chemonucleolysis versus laminectomy. A cohort comparison of effectiveness and charges. Spine 20:16–22
Khoo LT, Fessler RG (2002) Microendoscopic decompressive laminectomy for the treatment of lumbar stenosis. Neurosurgery 51:146–154
Maroon JC (2002) Current concepts in minimally invasive discectomy. Neurosurgery 51:137–145
McAfee PC, Lee GA, Fedder IL, et al (2002) Anterior BAK instrumentation and fusion: complete versus partial discectomy. Clin Orthop 394:55–63
Mixter WJ, Barr JS (1934) Rupture of the intervertebral disc with involvement of the spinal canal. N Engl J Med 211:210–215
Nakagawa H, Kamimura M, Uchiyama S, et al (2003) Microendoscopic discectomy (MED) for lumbar disc prolapse. J Clin Neurosci 10:231–235
Schick U, Dohnert J (2002) Technique of microendoscopy in medial lumbar disc herniation. Minim Invasive Neurosurg 45:139–141
Williams RW (1978) Micro lumbar discectomy: a conservative surgical approach to the virgin herniated lumbar disc. Spine 3:75–82
Williams RW (1993) Lumbar disc disease. Microdiscectomy. Neurosurg Clin N Am 4:101–118
Williams RW (1986) Microlumbar discectomy. A 12-year statistical review. Spine 11:851–852
Woodard EJ, Leon SP, Moriarty TM, et al (2001) Initial experience with intraoperative magnetic resonance imaging in spine surgery. Spine 26(4):410–417
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Mohanlal, P., Pal, D. & Timothy, J. Localisation of spinal level in lumbar microdiscectomy. Eur J Orthop Surg Traumatol 16, 207–209 (2006). https://doi.org/10.1007/s00590-005-0059-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00590-005-0059-7