
Abstract
Purpose
The aim of this study was to compare the clinical and radiographical outcomes between OLIF and ALIF in treating lumbar degenerative diseases.
Methods
We searched PubMed, Embase, Web of Science, and Cochrane Library for relevant studies. Changes in disc height (DH), segmental lordosis angle (SLA), lumbar lordosis (LL), visual analogue scale (VAS) score, and Oswestry disability index (ODI) between baseline and final follow-up, along with other important surgical outcomes, were assessed and analysed. Data on the global fusion rate and main complications were collected and compared.
Results
Approximately, 2041 patients from 36 studies were included, consisting of 1057 patients who underwent OLIF and 984 patients who underwent ALIF. The results reveal no significant difference in DH, SLA, VAS score, and ODI between the two groups (all P > 0.05). The operation time, estimated blood loss, and length of hospital stay were also comparable between the two groups. Over 90% of the fusion rate was achieved in both groups. The OLIF group showed a higher complication rate than the ALIF group (OLIF 18.83% vs ALIF 7.32%).
Conclusions
OLIF leads to a higher complication rate, with the most notable complication being cage subsidence. Both OLIF and ALIF are effective treatments for degenerative lumbar diseases and have similar therapeutic effects. ALIF was expected to be more expensive for patients because of the necessity of involving vascular surgeons.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Compared with traditional posterior approaches, anterior or lateral approaches, such as anterior lumbar interbody fusion (ALIF) and oblique lumbar interbody fusion (OLIF), can provide a similar fusion rate while avoiding violating posterior muscles and nerve structures [1, 2], thus reducing operation time and blood loss, and have relatively fewer postoperative complications [3]. These techniques are widely used in patients based on the above advantages. ALIF has been used to treat degenerative lumbar diseases in the past few decades [4], with the method leading to satisfying clinical relief for patients. However, the need to move abdominal contents and the aorta/vena cava during the operation to obtain a more satisfactory working corridor [5, 6] is likely to cause vascular injury, deep vein thrombosis, and ileus [5]. OLIF is a newly introduced surgical approach first conducted in 2012. Unlike traditional LLIF, OLIF naturally protects the lumbar plexus because it avoided incision into the psoas muscle [7]. Consequently, there is no need for interoperating nerve monitoring, and OLIF leads to fewer complications compared with LLIF [8].
OLIF shares the same retroperitoneal working corridor as ALIF, but as a newly established surgical approach, few existing studies have revealed the direct comparison of OLIF and ALIF. Zhuo et al. [6] compared ALIF and OLIF in patients with degenerative lumbar diseases and found that OLIF can achieve similar clinical outcomes compared with those of ALIF, with shorter operation times and less blood loss. However, the ALIF approach allowed a larger cage to be implanted; therefore, patients in the ALIF group achieved a larger increase in postoperative disc height. Hee et al. [9] found that patients in the OLIF group had larger disc heights and greater sagittal disc angles than those of the ALIF group, in contrast to Zhuo et al., who concluded OLIF to be more effective in restoring sagittal balance. As it is still controversial whether ALIF or OLIF is a better option for degenerative lumbar diseases, we conducted this systematic review to further discuss the issue. The aim of this study was to compare the pre- and post-operative clinical effectiveness (visual analogue scale [VAS] score, Oswestry disability index [ODI]), radiographical parameters (disc height [DH], segmental lordosis angle [SLA], lumbar lordosis [LL], and fusion rate), intraoperative parameters (operation time [OT], estimated blood loss [EBL], and length of hospital stay [LOS]) and complication rate of ALIF and OLIF to comprehensively evaluate the two surgical approaches for degenerative lumbar diseases.
Methods
This study was performed following the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses. (PRISMA 2020 Checklist) [10]
Search strategy
Based on the PRISMA 2020 Checklist, a systematic literature search was performed in PubMed, Embase, Web of Science, and Cochrane Library without time limitations in April 2022. The terms to find relevant studies were as follows: “oblique lateral interbody fusion,” “oblique lumbar interbody fusion,” “oblique lateral lumbar interbody fusion,” “retroperitoneal lumbar interbody fusion,” “pre-psoas lateral interbody fusion,” “anterior to psoas lumbar interbody fusion,” “anterolateral approach to lumbar,” “OLLIF,” “OLIF,” “ATP approach,” “anterior lumbar interbody fusion,” “ALIF,” “degenerative disc disease,” “degenerative lumbar disease,” “lumbar degenerative spondylolisthesis,” degenerative kyphoscoliosis,” and “spinal stenosis.” The search results were exported into NoteExpress V3.0 for further processing. Meanwhile, we checked the reference lists of the included studies to access more relevant studies.
Selection criteria
The inclusion criteria for the present study were as follows:
-
1.
Population: patients treated by OLIF or ALIF with a diagnosis of lumbar degenerative disease, degenerative disc disease, degenerative kyphoscoliosis, or degenerative spondylolisthesis using computed tomography and magnetic resonance imaging.
-
2.
Interventions: the patients treated by oblique lateral interbody fusion were in the OLIF group, while patients treated by anterior lumbar interbody fusion were designated as the ALIF group.
-
3.
Outcomes: the primary outcomes of the study were to compare clinical (including VAS score, ODI score, and complication rate) and radiographical (including DH, SLA, LL, and fusion rate) parameters after OLIF or ALIF surgical strategies. The secondary outcomes included the measurements of mean OT, EBL, and LOS between the two surgery strategies.
-
4.
Article type: published clinical research articles, excluding case reports and review articles.
We excluded duplicated, nonclinical studies, studies without primary outcomes, and studies with unavailable data.
Data extraction
Two reviewers (D.S. and W.S.L) independently extracted the following data from the included studies using a predesigned data extraction form: first author, publication year, study design, demographic information (number, sex, and mean age), inclusion disease, DH, SLA, LL, VAS score, ODI, fusion rate, complication rate, OT, EBL, and LOS. Any discrepancies in data extraction between the two reviewers were resolved through mutual agreement or consulting the third reviewer (Y.H.).
Statistical analysis
Statistical analyses were conducted using SPSS version 20.0 for Windows. Continuous variables were reported as mean ± standard deviation (SD) and were compared with the unpaired t test or nonparametric Mann–Whitney test. Two-sided P values were reported, and significance was established at a level of P < 0.05.
Results
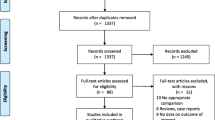
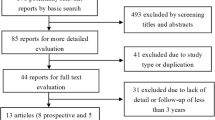
Thirty-six articles were eventually included in the study (Fig. 1): 1 was of level II evidence [11], 32 were of level III evidence [6, 9, 12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41] and 3 were of level IV of evidence [42,43,44]. Overall, 1057 patients were included in the OLIF group (mean age 63.64 ± 3.51 years; mean body mass index 23.96 ± 1.25 kg/m2; women accounted for 61.97% of cases), and the mean follow-up (FU) period was 15.96 ± 8.36 months. Approximately, 984 patients who underwent ALIF were included in the study (mean age 53.14 ± 8.20 years; mean body mass index 26.31 ± 1.63 kg/m2; women accounted for 57.93% of cases), and the mean FU period was 25.68 ± 10.35 months. The general information of included patients is summarized in Table 1.

PRISMA flow chart for the search and inclusion strategy
Twenty-nine articles included the treated levels: the surgeries were performed at a total of 2103 segment levels (1006 in the OLIF group, 1097 in the ALIF group), and 77.6% of the surgeries were performed at L4–S1 segments. There were 904 cases (43.13%) at L5–S1, 725 cases (34.37%) at L4–5, 347 cases (16.50%) at L3–4, 110 cases (5.24%) at L2–3, 14 cases (0.67%) at L1–2. The main indication for surgery was degenerative disc disease, spondylolisthesis, spinal stenosis, and adult degenerative scoliosis.
In the OLIF group, six articles included the size of the cage used in the surgery, with the cage height ranged from 8 to 14 mm, and an average height of 10.85 ± 1.09 mm [6, 9, 15, 19, 23, 26]. In the ALIF group, one article included a significantly higher cage [37], ranging from 12 to 19 mm, with the average cage height in five articles of the ALIF group being 13.61 ± 2.00 mm [6, 9, 30, 37, 41]. The cage used in the ALIF group is significantly higher than that in the OLIF group (P < 0.05).
In the OLIF group, 11 articles included the use of posterior percutaneous pedicles screw fixation for stabilization of all included patients [9, 12, 14,15,16, 18, 20, 21, 23, 25, 43], three articles included the use of lateral screw after OLIF [13, 26, 27], and four articles included posterior depression and screw fixation only for the patient with persistent radiculopathy [6, 22, 24, 42]. Only two articles used stand-alone OLIF with an anterior locking plate [17, 19]. In the ALIF group, six articles reported percutaneous pedicles screw fixation for all patients [9, 33, 34, 36, 40, 44], 10 articles included stand-alone ALIF [6, 28,29,30,31,32, 35, 37, 38, 41], and the stabilization was achieved by anterior plate fixation or using other self-locking devices along with the cage. A total of two articles used posterior fixation only for patients with Grade I spondylolisthesis, interarticularis fractures, or a history of laminectomy/facetectomy [11, 39]. A total of 361 ALIF procedures (36.38%) were accomplished with the assistance of vascular surgeons [6, 28, 31, 35, 37, 40].
For clinical effectiveness, pain relief was commonly measured by calculating the VAS scores of back and leg as well as ODI. VAS leg pain scored improved by a mean of 5.01 ± 1.16 in the OLIF group [9, 13, 17, 18, 20,21,22, 25, 26] and 3.81 ± 2.14 in the ALIF group [9, 11, 28, 30, 34, 36, 39], with no significate difference found between the groups (P = 0.17). VAS back pain scores improved by a mean of 3.59 ± 1.86 in the OLIF group [9, 13, 16, 18,19,20,21,22, 25] and 4.04 ± 1.28 in the ALIF group [9, 11, 28, 30, 32, 34, 36, 39], with no significate difference was found between groups (p > 0.05). In terms of ODI, the OLIF group [9, 12, 13, 16, 17, 19,20,21, 24,25,26,27, 42, 43] showed a mean improvement of 32.61 ± 13.55, while the ALIF group [9, 11, 28,29,30,31,32, 34, 35, 39, 44] showed a mean improvement of 28.50 ± 12.44. These data were higher than the reported minimum clinically important difference of ODI (11%) after adult spinal deformity surgery [45]. There was no significant difference in the ODI between groups (P > 0.05). The clinical results are summarized in Table 2.
As for radiographic parameters, we compared the change of DH, SLA, and LL between the OLIF and ALIF groups. A total of 13 authors in the OLIF group [6, 9, 13,14,15, 17,18,19,20, 23, 26, 42, 43] reported a mean increase of 3.48 ± 1.26 mm DH (53.9% improvement), while 9 authors in the ALIF group [6, 9, 28, 30, 32,33,34, 37, 40] reported a mean increase of 4.70 ± 2.52 mm DH (81.2% improvement); however, the difference between groups was not significant.
A total of 10 authors reported the change in SLA in the OLIF group [6, 9, 13,14,15, 18, 19, 23, 26, 43], with an average of 4.40 ± 2.05°increase. Approximately, nine authors in the ALIF group [6, 9, 28,29,30, 32, 34, 39, 41] reported an average of 6.72 ± 2.82°increase in SLA, with no significant difference found between the groups.(P > 0.05).
As for LL, five authors in the OLIF group [14, 16, 17, 19, 43] reported mean of 8.35 ± 3.29°alteration, while eight authors in the ALIF group [29, 30, 32, 34, 39,40,41, 44] reported a mean of 3.64 ± 1.94°alteration. The change of LL was significantly larger in the OLIF group than in the ALIF group. The result of radiographical changes is listed in Table 3.
In the evaluation of surgical parameters, we compared operation time, estimated blood loss, and the length of hospital stay between the two surgical strategies. Operation time was recorded by 16 authors in the OLIF group and 8 authors in the ALIF group. The mean operation time in the OLIF surgery was 134.12 min and in the ALIF surgery was 126.09 min, with no significant difference between the two groups (P > 0.05). Estimated blood loss was reported in 16 OLIF articles and 9 ALIF articles, with the average blood loss being 105.18 ml in OLIF surgery, and 131.71 ml in ALIF surgery. No significant difference was found between the groups. For the length of hospital stay, patients in the OLIF group generally experienced 6.08 ± 2.14 days of hospital care, while those in the ALIF group stayed in the hospital for 4.06 ± 2.56 days. There was no significant difference between the groups (all P > 0.05). The results of operation-related parameters are summarized in Table 4.
Over 90% of the total fusion rate was achieved using both methods (90.83% in the OLIF group, 93.66% in the ALIF group). In terms of complications, the overall complication rate was 18.83% (199 in 1057 patients) in the OLIF group and 7.32% (72 in 984 patients) in the ALIF group. The most common complications in the OLIF group were cage subsidence (11.35%), pain/numbness/weakness in the thigh or psoas (2.37%), sympathetic chain symptoms (1.7%), and lumbar plexopathy (1.04%). Postoperative ileus (1.52%) was the most common complication in the ALIF group, followed by cage subsidence (1.32%), and pain/numbness/weakness in the thigh or psoas (1.32%), and other complications are listed in Table 5. Compared with the OLIF group, the ALIF group rarely presented cage subsidence (1.32%) and pain/numbness/weakness in the thigh or psoas (1.32%).
Discussion
We systematically reviewed the difference in radiographical and clinical outcomes between OLIF and ALIF for degenerative lumbar diseases. To the best of our knowledge, there has been no systematic review of the literature directly comparing the two techniques. For the radiographical results, obtaining larger DH and SLA restoration indicates that the surgery is more beneficial for the patients. We found that both OLIF and ALIF can significantly increase the DH and SLA compared with the preoperative data. DH restoration is closely related to the size of the cage implanted in the surgery, and higher cages were used for the ALIF group compared with the OLIF group (10.85 ± 1.09 mm vs 13.61 ± 2.00 mm, P < 0.05). The change of DH in the ALIF group was relatively larger (4.70 ± 2.52 mm vs 3.48 ± 1.26 mm); however, no statistical difference was found. The size of cage chosen would depend on the patient’s individual condition, and patients inserted with a larger cage gain more DH [6, 9, 26]. We believe the variation of cage size in the two groups is not approach-related. Although an oversized interbody cage would more effectively increase the intervertebral height, stress between the cage and the osseous endplate would increase, readily causing the sinking of the cage [17]. This mechanism might be the possible explanation for the similar change of DH between the OLIF and the ALIF group.
In terms of SLA restoration, a study [46] showed larger preoperative disc angle, more considerable lift up of the disc space, and a more anterior cage position associated with larger SLA restoration in LLIF. Studies have shown that the LLIF operation may cause approximately 34% of the cage to be implanted in the anterior position [47]; thus, LLIF or OLIF should be more beneficial for postoperative SLA restoration. Our result showed no significant difference between the two groups (P > 0.05), with the average change of SLA was more remarkable in the ALIF group (4.40 ± 2.05°vs 6.72 ± 2.82°). This result was consistent with that of Watkins et al.[48], who found that compared with LLIF, ALIF can significantly increase the SLA, but they did not further explore the reasons. We further compared preoperative disc angles between the two groups and found the ALIF group showed larger preoperative SLA. In conclusion, the slight difference in SLA restoration might be caused by preoperative SLA variation and difference in DH restoration.
A well-balanced spine is the goal of all spine surgeries. We evaluated the postoperative sagittal balance of patients by restoration of general LL. The OLIF group gained more LL restoration than the ALIF group (8.35 ± 3.29°vs 3.64 ± 1.94°, p < 0.05). We found that the majority of patients in the OLIF group (11 of 20 studies) underwent percutaneous pedicles screw fixation after cage implantation, while most ALIF procedures were strengthened by self-locking plate or intrinsic screws. Additional posterior fixation could help maintain the correction of the LL previously achieved by the cage implantation [41]; this larger LL restoration in the OLIF group might be a selective bias. The effective restoration of LL could strongly prevent flat back syndrome upon long-term follow-up after lumbar fusion surgeries [49]; we believe additional posterior fixation can be beneficial for patient.
Clinical relief of pain is critical to patients’ quality of life. We evaluated the clinical effectiveness of OLIF and ALIF by VAS leg and back pain scores, as well as ODI. The postoperative change of VAS score and ODI revealed a notable clinical relief of pain among patients in both groups, and no significant statistical difference was found. The change in ODI was higher than the reported minimum clinically important difference of ODI (11%) after adult spinal deformity surgery [45] in both groups. ALIF has been performed for decades and may have the best outcomes in indirect decompression methods [50]; many studies showed significant indirect foraminal decompression using ALIF [51, 52]. As a newly introduced anterolateral indirect decompression method, OLIF could reach a comparable clinical and radiographical effectiveness to that of the ALIF technique; we believe OLIF can emerge as a new indirect decompression method that can be utilized in treating degenerative lumbar diseases.
We found that fusion rates in OLIF and ALIF were both satisfying (> 90%). The complication rate of OLIF was significantly higher than that of ALIF (18.83% vs 7.32%). Cage subsidence (11.35%, total of 120 levels) is the most common complication in the OLIF group; however, this complication only happened in 1.32% of the ALIF group. Kotheeranurak et. al [53] found age > 60 years, bone mineral density < -2.5, higher cage height, and severe multifidus muscle fatty degeneration were the top risk factors of cage subsidence after OLIF. Patients included in the OLIF group were characterized a mean age over 60 years old, while patients’ mean age in the ALIF group was younger (around 53 years old); this might be an explanation for the difference. Meanwhile, the cage used in ALIF surgeries is often accompanied by a self-locking anterior plate or screw; this design further prevented cage subsidence after stand-alone ALIF surgeries. The most common complication in the ALIF group was postoperative ileus; this is an approach-related complication. Traditional ALIF was performed using a supine position; bowel mobilization was required to get access to the spine. OLIF surgeries were operated on right lateral decubitus, abdominal contents would automatically shift aside because of gravity, so less bowel mobilization is needed in OLIF surgeries, and postoperative ileus was rarely seen (less than 1%). Other complication includes thigh or psoas pain/numbness/weakness, sympathetic chain symptoms, lumbar plexopathy, vascular injury, deep venous thromboses, pseudarthrosis, wound infection, and incisional pain. Most of the complications were relieved within 3 months after the surgeries and with no need for special treatment, only a few cases needed reoperation.
Surgical expenditure is critical for patient when making surgery decisions. However, none of the included articles reported total cost of the surgeries. We assume the OLIF technique can be cheaper for patients, for about 36.68% ALIF surgeries were accomplished by assistance of vascular surgeons, and that would surely increase the expected surgical expenditure.
This study has some limitations. First, there is no published RCT study on OLIF. Many included studies were designed as prospective or retrospective cohort studies. Secondly, surgical indications of the included population were highly variable, so the result could just establish a general impression between the two surgical approaches; more multicentre prospective randomized controlled trials directly comparing OLIF and ALIF are required to provide the possibility of further evaluation.
Conclusion
In conclusion, for the surgical treatment of lumbar degenerative diseases, both ALIF and OLIF could provide satisfactory outcomes with an overall fusion rate of over 90% in both groups. OLIF showed comparable radiographic and clinical results to the ALIF, with lower expected surgical expenditure. However, the complication rate in the OLIF group was significantly higher than in the ALIF group; the most concerning complication in the OLIF group was cage subsidence. More prospective randomized controlled trials directly comparing OLIF and ALIF are needed, to promote the development of precision therapy for lumbar degenerative diseases in geriatric spine surgery.
References
Fan SW, Hu ZJ, Fang XQ, Zhao FD, Huang Y, Yu HJ (2010) Comparison of paraspinal muscle injury in one-level lumbar posterior inter-body fusion: modified minimally invasive and traditional open approaches. Orthop Surg 2:194–200. https://doi.org/10.1111/j.1757-7861.2010.00086.x
Han B, Liang W, Hai Y, Liu Y, Chen Y, Ding H, Yin P (2022) Elucidating the potential mechanisms underlying distraction spinal cord injury-associated neuroinflammation and apoptosis. Front Cell Dev Biol 10:839313. https://doi.org/10.3389/fcell.2022.839313
Allain J, Dufour T (2020) Anterior lumbar fusion techniques: ALIF, OLIF, DLIF, LLIF, IXLIF. Orthop Traumatol Surg Res 106:S149–S157. https://doi.org/10.1016/j.otsr.2019.05.024
Teng I, Han J, Phan K, Mobbs R (2017) A meta-analysis comparing ALIF, PLIF, TLIF and LLIF. J Clin Neurosci 44:11–17. https://doi.org/10.1016/j.jocn.2017.06.013
Manunga J, Alcala C, Smith J, Mirza A, Titus J, Skeik N, Senthil J, Stephenson E, Alexander J, Sullivan T (2021) Technical approach, outcomes, and exposure-related complications in patients undergoing anterior lumbar interbody fusion. J Vasc Surg 73:992–998. https://doi.org/10.1016/j.jvs.2020.06.129
Xi Z, Burch S, Mummaneni PV, Chang CC, Ruan H, Eichler C, Chou D (2020) Supine anterior lumbar interbody fusion versus lateral position oblique lumbar interbody fusion at L5–S1: a comparison of two approaches to the lumbosacral junction. J Clin Neurosci 82:134–140. https://doi.org/10.1016/j.jocn.2020.10.043
Mobbs RJ, Phan K, Malham G, Seex K, Rao PJ (2015) Lumbar interbody fusion: techniques, indications and comparison of interbody fusion options including PLIF, TLIF, MI-TLIF, OLIF/ATP, LLIF and ALIF. J spine surg 1(1):2
Guerin P, Obeid I, Bourghli A, Masquefa T, Luc S, Gille O, Pointillart V, Vital JM (2012) The lumbosacral plexus: anatomic considerations for minimally invasive retroperitoneal transpsoas approach. Surg Radiol Anat 34:151–157. https://doi.org/10.1007/s00276-011-0881-z
Chung HW, Lee HD, Jeon CH, Chung NS (2021) Comparison of surgical outcomes between oblique lateral interbody fusion (OLIF) and anterior lumbar interbody fusion (ALIF). Clin Neurol Neurosurg 209:106901. https://doi.org/10.1016/j.clineuro.2021.106901
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, Chou R, Glanville J, Grimshaw JM, Hrobjartsson A, Lalu MM, Li T, Loder EW, Mayo-Wilson E, McDonald S, McGuinness LA, Stewart LA, Thomas J, Tricco AC, Welch VA, Whiting P, Moher D (2021) The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. J Clin Epidemiol 134:178–189. https://doi.org/10.1016/j.jclinepi.2021.03.001
Rickert M, Fleege C, Papachristos I, Makowski MR, Rauschmann M, Arabmotlagh M (2019) Clinical outcome after anterior lumbar interbody fusion with a new osteoinductive bone substitute material: a randomized clinical pilot study. Clin Spine Surg 32:E319–E325. https://doi.org/10.1097/BSD.0000000000000802
Zeng ZY, Xu ZW, He DW, Zhao X, Ma WH, Ni WF, Song YX, Zhang JQ, Yu W, Fang XQ, Zhou ZJ, Xu NJ, Huang WJ, Hu ZC, Wu AL, Ji JF, Han JF, Fan SW, Zhao FD, Jin H, Pei F, Fan SY, Sui DX (2018) Complications and prevention strategies of oblique lateral interbody fusion technique. Orthop Surg 10:98–106. https://doi.org/10.1111/os.12380
Hung SF, Liao JC, Tsai TT, Li YD, Chiu PY, Hsieh MK, Kao FC (2021) Comparison of outcomes between indirect decompression of oblique lumbar interbody fusion and MIS-TLIF in one single-level lumbar spondylosis. Sci Rep 11:12783. https://doi.org/10.1038/s41598-021-92330-9
Jin C, Jaiswal MS, Jeun SS, Ryu KS, Hur JW, Kim JS (2018) Outcomes of oblique lateral interbody fusion for degenerative lumbar disease in patients under or over 65 years of age. J Orthop Surg Res 13:38. https://doi.org/10.1186/s13018-018-0740-2
Shimizu T, Fujibayashi S, Otsuki B, Murata K, Matsuda S (2021) Indirect decompression via oblique lateral interbody fusion for severe degenerative lumbar spinal stenosis: a comparative study with direct decompression transforaminal/posterior lumbar interbody fusion. Spine J 21:963–971. https://doi.org/10.1016/j.spinee.2021.01.025
Wen J, Shi C, Yu L, Wang S, Xi Y, Ye X (2020) Unilateral versus bilateral percutaneous pedicle screw fixation in oblique lumbar interbody fusion. World Neurosurg 134:e920–e927. https://doi.org/10.1016/j.wneu.2019.11.035
Xiao L, Zhao Q, Sun X, Liu C, Zhang Y, Xu H (2020) Relationship between alterations of spinal/pelvic sagittal parameters and clinical outcomes after oblique lumbar interbody fusion. World Neurosurg 133:e156–e164. https://doi.org/10.1016/j.wneu.2019.08.158
Kotani Y, Ikeura A, Tokunaga H, Saito T (2021) Single-level controlled comparison of OLIF51 and percutaneous screw in lateral position versus MIS-TLIF for lumbosacral degenerative disorders: clinical and radiologic study. J Orthop Sci 26:756–764. https://doi.org/10.1016/j.jos.2020.08.005
Miscusi M, Trungu S, Ricciardi L, Forcato S, Ramieri A, Raco A (2020) The anterior-to-psoas approach for interbody fusion at the L5–S1 segment: clinical and radiological outcomes. Neurosurg Focus 49:E14. https://doi.org/10.3171/2020.6.FOCUS20335
Jung J, Lee S, Cho DC, Han IB, Kim CH, Lee YS, Kim KT (2021) Usefulness of oblique lumbar interbody fusion as revision surgery: comparison of clinical and radiological outcomes between primary and revision surgery. World Neurosurg 149:e1067–e1076. https://doi.org/10.1016/j.wneu.2020.12.172
Sato J, Ohtori S, Orita S, Yamauchi K, Eguchi Y, Ochiai N, Kuniyoshi K, Aoki Y, Nakamura J, Miyagi M, Suzuki M, Kubota G, Inage K, Sainoh T, Fujimoto K, Shiga Y, Abe K, Kanamoto H, Inoue G, Takahashi K (2017) Radiographic evaluation of indirect decompression of mini-open anterior retroperitoneal lumbar interbody fusion: oblique lateral interbody fusion for degenerated lumbar spondylolisthesis. Eur Spine J 26:671–678. https://doi.org/10.1007/s00586-015-4170-0
DiGiorgio AM, Edwards CS, Virk MS, Mummaneni PV, Chou D (2017) Stereotactic navigation for the prepsoas oblique lateral lumbar interbody fusion: technical note and case series. Neurosurg Focus 43:E14. https://doi.org/10.3171/2017.5.FOCUS17168
Fujibayashi S, Hynes RA, Otsuki B, Kimura H, Takemoto M, Matsuda S (2015) Effect of indirect neural decompression through oblique lateral interbody fusion for degenerative lumbar disease. Spine 40:175–182. https://doi.org/10.1097/BRS.0000000000000703
Miscusi M, Ramieri A, Forcato S, Giuffre M, Trungu S, Cimatti M, Pesce A, Familiari P, Piazza A, Carnevali C, Costanzo G, Raco A (2018) Comparison of pure lateral and oblique lateral inter-body fusion for treatment of lumbar degenerative disk disease: a multicentric cohort study. Eur Spine J 27:222–228. https://doi.org/10.1007/s00586-018-5596-y
Ohtori S, Orita S, Yamauchi K, Eguchi Y, Ochiai N, Kishida S, Kuniyoshi K, Aoki Y, Nakamura J, Ishikawa T, Miyagi M, Kamoda H, Suzuki M, Kubota G, Sakuma Y, Oikawa Y, Inage K, Sainoh T, Sato J, Fujimoto K, Shiga Y, Abe K, Toyone T, Inoue G, Takahashi K (2015) Mini-open anterior retroperitoneal lumbar interbody fusion: oblique lateral interbody fusion for lumbar spinal degeneration disease. Yonsei Med J 56:1051–1059. https://doi.org/10.3349/ymj.2015.56.4.1051
Li R, Shao X, Li X, Liu Y, Jiang W (2021) Comparison of clinical outcomes and spino-pelvic sagittal balance in degenerative lumbar spondylolisthesis: minimally invasive oblique lumbar interbody fusion (OLIF) versus transforaminal lumbar interbody fusion (TLIF). Medicine 100:e23783. https://doi.org/10.1097/MD.0000000000023783
Yang Z, Chang J, Sun L, Chen CM, Feng H (2020) Comparing oblique lumbar interbody fusion with lateral screw fixation and transforaminal full-endoscopic lumbar discectomy (OLIF-TELD) and posterior lumbar interbody fusion (PLIF) for the treatment of adjacent segment disease. Biomed Res Int 2020:4610128. https://doi.org/10.1155/2020/4610128
Malham GM, Parker RM, Blecher CM, Chow FY, Seex KA (2016) Choice of approach does not affect clinical and radiologic outcomes: a comparative cohort of patients having anterior lumbar interbody fusion and patients having lateral lumbar interbody fusion at 24 months. Global Spine J 6:472–481. https://doi.org/10.1055/s-0035-1569055
Bassani R, Morselli C, Querenghi AM, Nuara A, Sconfienza LM, Peretti GM (2020) Functional and radiological outcome of anterior retroperitoneal versus posterior transforaminal interbody fusion in the management of single-level lumbar degenerative disease. Neurosurg Focus 49:E2. https://doi.org/10.3171/2020.6.FOCUS20374
Szadkowski M, d’Astorg H, Bouhali H, Aleksic I, Ramos-Pascual S, Fiere V (2020) Outcomes of stand-alone anterior lumbar interbody fusion of L5–S1 using a novel implant with anterior plate fixation. Spine J 20:1618–1628. https://doi.org/10.1016/j.spinee.2020.05.555
Mobbs RJ, Maharaj M, Rao PJ (2014) Clinical outcomes and fusion rates following anterior lumbar interbody fusion with bone graft substitute i-FACTOR, an anorganic bone matrix/P-15 composite. J Neurosurg Spine 21:867–876. https://doi.org/10.3171/2014.9.SPINE131151
Norotte G, Barrios C (2018) Clinical and radiological outcomes after stand-alone ALIF for single L5–S1 degenerative discopathy using a PEEK cage filled with hydroxyapatite nanoparticles without bone graft. Clin Neurol Neurosurg 168:24–29. https://doi.org/10.1016/j.clineuro.2018.01.037
Pavlov PW, Meijers H, van Limbeek J, Jacobs WC, Lemmens JA, Obradov-Rajic M, de Kleuver M (2004) Good outcome and restoration of lordosis after anterior lumbar interbody fusion with additional posterior fixation. Spine 29:1893–1899. https://doi.org/10.1097/01.brs.0000137067.68630.70
Kim JS, Kim DH, Lee SH, Park CK, Hwang JH, Cheh G, Choi YG, Kang BU, Lee HY (2010) Comparison study of the instrumented circumferential fusion with instrumented anterior lumbar interbody fusion as a surgical procedure for adult low-grade isthmic spondylolisthesis. World Neurosurg 73:565–571. https://doi.org/10.1016/j.wneu.2010.02.057
Kleeman TJ, Ahn UM, Talbot-Kleeman A (2001) Laparoscopic anterior lumbar interbody fusion with rhBMP-2: a prospective study of clinical and radiographic outcomes. Spine 26:2751–2756. https://doi.org/10.1097/00007632-200112150-00026
Shim JH, Kim WS, Kim JH, Kim DH, Hwang JH, Park CK (2011) Comparison of instrumented posterolateral fusion versus percutaneous pedicle screw fixation combined with anterior lumbar interbody fusion in elderly patients with L5–S1 isthmic spondylolisthesis and foraminal stenosis. J Neurosurg Spine 15:311–319. https://doi.org/10.3171/2011.4.SPINE10653
Phan K, Davies S, Rao PJ, Mobbs RJ (2017) Worker’s compensation status and outcomes following anterior lumbar interbody fusion: prospective observational study. World Neurosurg 103:680–685. https://doi.org/10.1016/j.wneu.2017.04.123
Chung SK, Lee SH, Lim SR, Kim DY, Jang JS, Nam KS, Lee HY (2003) Comparative study of laparoscopic L5–S1 fusion versus open mini-ALIF, with a minimum 2-year follow-up. Eur Spine J 12:613–617. https://doi.org/10.1007/s00586-003-0526-y
Moses ZB, Razvi S, Oh SY, Platt A, Keegan KC, Hamati F, Witiw C, David BT, Fontes RBV, Deutsch H, O’Toole JE, Fessler RG (2021) A retrospective comparison of radiographic and clinical outcomes in single-level degenerative lumbar disease undergoing anterior versus transforaminal lumbar interbody fusion. J Spine Surg 7:170–180. https://doi.org/10.21037/jss-20-673
Hsieh PC, Koski TR, O’Shaughnessy BA, Sugrue P, Salehi S, Ondra S, Liu JC (2007) Anterior lumbar interbody fusion in comparison with transforaminal lumbar interbody fusion: implications for the restoration of foraminal height, local disc angle, lumbar lordosis, and sagittal balance. J Neurosurg Spine 7:379–386. https://doi.org/10.3171/SPI-07/10/379
Jaeger A, Giber D, Bastard C, Thiebaut B, Roubineau F, Flouzat Lachaniette CH, Dubory A (2019) Risk factors of instrumentation failure and pseudarthrosis after stand-alone L5–S1 anterior lumbar interbody fusion: a retrospective cohort study. J Neurosurg Spine 31:338–346. https://doi.org/10.3171/2019.3.SPINE181476
Zhang C, Wang K, Jian F, Wu H (2018) Efficacy of oblique lateral interbody fusion in treatment of degenerative lumbar disease. World Neurosurg. https://doi.org/10.1016/j.wneu.2018.11.139
Heo DH, Kim JS (2017) Clinical and radiological outcomes of spinal endoscopic discectomy-assisted oblique lumbar interbody fusion: preliminary results. Neurosurg Focus 43:E13. https://doi.org/10.3171/2017.5.FOCUS17196
Crandall DG, Revella J (2009) Transforaminal lumbar interbody fusion versus anterior lumbar interbody fusion as an adjunct to posterior instrumented correction of degenerative lumbar scoliosis: three year clinical and radiographic outcomes. Spine 34:2126–2133. https://doi.org/10.1097/BRS.0b013e3181b612db
Yoshida G, Hasegawa T, Yamato Y, Kobayashi S, Shin O, Banno T, Mihara Y, Arima H, Ushirozako H, Yasuda T, Togawa D, Matsuyama Y (2019) Minimum clinically important differences in oswestry disability index domains and their impact on adult spinal deformity surgery. Asian Spine J 13:35–44. https://doi.org/10.31616/asj.2018.0077
Otsuki B, Fujibayashi S, Takemoto M, Kimura H, Shimizu T, Murata K, Matsuda S (2020) Analysis of the factors affecting lumbar segmental lordosis after lateral lumbar interbody fusion. Spine 45:E839–E846. https://doi.org/10.1097/BRS.0000000000003432
Regev GJ, Haloman S, Chen L, Dhawan M, Lee YP, Garfin SR, Kim CW (2010) Incidence and prevention of intervertebral cage overhang with minimally invasive lateral approach fusions. Spine 35:1406–1411. https://doi.org/10.1097/BRS.0b013e3181c20fb5
Watkins RG, Hanna R, Chang D, Watkins RG (2014) Sagittal alignment after lumbar interbody fusion: comparing anterior, lateral, and transforaminal approaches. J Spinal Disord Tech 27:253–256. https://doi.org/10.1097/BSD
Choi MK, Kim SM, Jo DJ (2020) Anterior lumbar interbody fusions combined with posterior column osteotomy in patients who had sagittal imbalance associated with degenerative lumbar flat-back deformity: a retrospective case series. Neurosurg Rev 43:1117–1125. https://doi.org/10.1007/s10143-019-01129-w
Yoshihara H (2017) Indirect decompression in spinal surgery. J Clin Neurosci 44:63–68. https://doi.org/10.1016/j.jocn.2017.06.061
Cho W, Sokolowski MJ, Mehbod AA, Denis F, Garvey TA, Perl J, Transfeldt EE (2013) MRI measurement of neuroforaminal dimension at the index and supradjacent levels after anterior lumbar interbody fusion: a prospective study. Clin Orthop Surg 5:49–54. https://doi.org/10.4055/cios.2013.5.1.49
Rao PJ, Maharaj MM, Phan K, Lakshan Abeygunasekara M, Mobbs RJ (2015) Indirect foraminal decompression after anterior lumbar interbody fusion: a prospective radiographic study using a new pedicle-to-pedicle technique. Spine J 15:817–824. https://doi.org/10.1016/j.spinee.2014.12.019
Kotheeranurak V, Jitpakdee K, Lin GX, Mahatthanatrakul A, Singhatanadgige W, Limthongkul W, Yingsakmongkol W, Kim JS (2021) Subsidence of interbody cage following oblique lateral interbody fusion: an analysis and potential risk factors. Global Spine J. https://doi.org/10.1177/21925682211067210
Funding
This study was supported by grants from the National Key Research and Development Program of China (No.2019YFC0120604), and the Innovation Grant of the National Clinical Research Center for Orthopedics, Sports Medicine & Rehabilitation (No2021-NCRC-CXJJ-PY-34).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that there are no conflicts of interest.
Consent to participate
We state that we have consented to participate.
Consent for publication
We state that we have consent for publication.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Sun, D., Liang, W., Hai, Y. et al. OLIF versus ALIF: Which is the better surgical approach for degenerative lumbar disease? A systematic review. Eur Spine J 32, 689–699 (2023). https://doi.org/10.1007/s00586-022-07516-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-022-07516-0