
Abstract
Purpose
To determine whether radiological, clinical, and demographic findings in patients with cervical spondylotic myelopathy (CSM) were independently associated with loss of cervical lordosis (LCL) after laminoplasty.
Methods
The prospective study included 41 consecutive patients who underwent laminoplasty for CSM. The difference in C2-7 Cobb angle between the postoperative and preoperative films was used to evaluate change in cervical alignment. Age, sex, body mass index (BMI), smoking history, preoperative C2-7 Cobb angle, T1 slope, C2-7 range of motion (C2-7 ROM), C2-7 sagittal vertical axis (C2-7 SVA), and cephalad vertebral level undergoing laminoplasty (CVLL) were assessed. Data were analyzed using Pearson and Spearman correlation test, and univariate and stepwise multivariate linear regression.
Results
T1 slope, C2-7 SVA, and CVLL significantly correlated with LCL (P < 0.001), whereas age, BMI, and preoperative C2-7 Cobb angle did not. In multiple linear regression analysis, higher T1 slope (B = 0.351, P = 0.037), greater C2-7 SVA (B = 0.393, P < 0.001), and starting laminoplasty at C4 level (B = − 7.038, P < 0.001) were significantly associated with higher postoperative LCL.
Conclusions
Cervical alignment was compromised after laminoplasty in patients with CSM, and the degree of LCL was associated with preoperative T1 slope, C2-7 SVA, and CVLL.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Laminoplasty has widely been used for the treatment of patients with cervical spondylotic myelopathy (CSM). It is well known that laminoplasty is a posterior indirect decompression method and is not suitable for patients with preoperative cervical kyphotic alignment [1, 2]. Adequate decompression could be obtained when cervical lordosis is maintained to allow the posterior shift of the cervical spinal cord after laminoplasty. Despite sufficient preoperative lordosis, laminoplasty often diminishes cervical lordosis and straightens the cervical spine [3]. Baba et al. [4] showed that cervical lordosis following laminoplasty is associated with posterior migration of the cervical spinal cord and that posterior cord migration correlates with improved outcomes based on the JOA score. Taniyama et al. [5] also demonstrated that a preoperative index could predict clinical outcome after laminoplasty. However, they did not analyze the association between preoperative factors and loss of cervical lordosis (LCL). Therefore, it is important to investigate risk factors related with LCL after laminoplasty.
Recently, T1 slope and C2-7 sagittal vertical axis (SVA) have emerged as predictors of kyphotic alignment change after laminoplasty [6, 7]. With regard to intraoperative factors, a recent study demonstrated that starting laminoplasty at C4 level led to significantly less LCL than starting at C3 level [8]. However, a multiple linear regression analysis is rare to examine the relationship between such updated factors and LCL after laminoplasty in patients with CSM. Given this background, we sought to conduct a rigorous, prospective study of the clinical and imaging features that are predictive of LCL after laminoplasty for patients with CSM.
Materials and methods
Patient population
The research protocol was approved by the Research and Ethics Committee of The Third Hospital of Hebei Medical University, and all patients gave written informed consent for their information to be stored in the hospital database and used for research. A total of 97 consecutive patients with CSM were prospectively enrolled from January 2013 to January 2014. Forty-six patients who had myelopathy caused by cervical disk herniation or ossification of the posterior longitudinal ligament (OPLL), the previous history of cervical spine surgery, combined congenital abnormality, C2-7 lordotic angle < −5°, or preoperative lateral X-rays not showing C7 level were excluded from this study. An additional 10 patients were lost to follow up within the 12 months after surgery because of various reasons unrelated to their CSM. The remaining 41 patients who could be tracked for more than 12 months after surgery were included in this study. Diagnoses were confirmed by neurological examinations and imaging studies, such as X-rays radiographs and MRI. Preoperatively, all of the patients had lordotic or straight sagittal alignments (C2-7 lordotic angle > −5°), because we generally performed anterior decompressive surgery or posterior decompression with fusion for such patients with preoperative kyphotic alignment at our institution.
In this study, all patients underwent expansive open-door laminoplasty using a plate fixation system. If the patient’s spinal canal at the C2-3 intervertebral level was narrow, laminoplasty starting at C3 level was performed. If the cephalad extent of spinal stenosis was no further cephalad than the C3-4 intervertebral level, a laminoplasty starting at C4 level would be performed while limiting detachment of the C2 muscle insertions. In all cases, the interspinous ligaments were preserved during surgery. Postoperatively, all patients were taught to wear a Philadelphia neck collar for 4 weeks.
Radiographic assessment
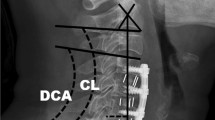
Cervical spine anteroposterior, lateral, flexion, and extension radiographs were taken preoperatively and postoperatively at the 1-year follow-up. Cervical lordosis was assessed by C2-7 Cobb angle. The Cobb angle from C2 to C7 was used as a measure of the cervical alignment, which was defined as the angle formed by the inferior endplates of C2 and C7 in standing lateral radiographs. An alignment of C2-7 Cobb angle of 0° or more was defined as lordosis, and an alignment of C2-7 Cobb angle less than 0° was defined as kyphosis [9, 10]. Changes in the cervical alignment were calculated with the following formula: alignment change (°) = (preoperative C2-7 Cobb angle) − (postoperative C2-7 Cobb angle) [7, 9]. According to this formula, alignment changes >0° were considered postoperative LCL. The C2-7 range of motion (ROM) was defined as the sum of the C2-7 Cobb angle during flexion and extension lateral radiographs. C2-7 SVA was defined as the distance from the posterosuperior corner of C7 and the vertical line from the center of the C2 body. T1 slope or T1 sagittal angle was measured as the angle between a horizontal line and the superior endplate of T1 on standing lateral radiograph [7, 9–11]. The measurement methods are summarized in Fig. 1.

Radiographic measurements. A C2-7 Cobb angle. B T1 slope. C C2-7 SVA. SVA indicates sagittal vertical axis
Statistical analysis
Data analyses were performed using SPSS version 18 for Windows (SPSS, Inc., Chicago, IL, USA). Data are presented as the number of subjects in each group or mean ± SD. To assess correlations between independent variables (age, BMI, preoperative C2-7 Cobb angle, T1 slope, C2-7 SVA, and CVLL) and dependent variable (LCL), we used Pearson and Spearman correlation coefficients. To identify the best predictors of LCL, multiple linear regression models were computed. First, univariate analysis was completed with LCL as the dependent variable and the other variables (age, gender, smoking, BMI, preoperative C2-7 Cobb angle, C2-7 ROM, T1 slope, C2-7 SVA, and CVLL) as independent variables. Then, a multiple linear regression was carried out to evaluate LCL. The independent variables that were entered into the model were those with a P < 0.10 in the univariate analysis. The final model included only independent variables with P < 0.05.
Results
Table 1 summarizes the patient characteristics and univariate analysis. The average age was 53.2 ± 6.8 years, the average BMI was 25.9 ± 6.7 kg/m2. There were 25 men and 16 women. Twenty-two patients had a history of smoking. The average C2-7 Cobb angle was 18.4 ± 10.1°, the average C2-7 ROM was 35.3 ± 13.7°, the average T1 slope was 22.2 ± 4.1°, and the average C2-7 SVA was 24.0 ± 11.7 mm before surgery. There were 21 patients who underwent laminoplasty beginning at C3, whereas 20 patients underwent laminoplasty beginning at C4. Of those clinical and imaging parameters, T1 slope, C2-7 SVA, and CVLL were significant variables (P < 0.001) associated with LCL, whereas age, gender, BMI, history of smoking, preoperative C2-7 Cobb angle, and C2-7 ROM were not significant variables.
Table 2 summarizes the Pearson and Spearman correlation coefficients. T1 slope, C2-7 SVA, and CVLL significantly correlated to LCL (P < 0.001), whereas age, BMI, and preoperative C2-7 Cobb angle did not.
Table 3 summarizes the stepwise multiple linear regression for LCL with backward elimination that combined T1 slope, C2-7 SVA, and CVLL (variables where P < 0.10 during univariate analysis), eliciting a significant regression model (F 3,37 = 100.459; P < 0.01) with R 2 0.891, and adjusted R 2 0.882; LCL is equal to −7.995 + 0.351 (T1 slope) + 0.393 (C2-7 SVA) − 7.038 (CVLL). LCL increased by 0.351° for each T1 slope, increased by 0.393° for each C2-7 SVA, and decreased by 7.038° for starting laminoplasty at C4 level. Each variable in the model showed P < 0.05.
Discussion
Anterior decompression and fusion can achieve a direct anterior decompression and stabilize the spinal column. However, posterior laminoplasty generates an indirect anterior decompression effect resulting from the posterior shift of the spinal cord from the anterior compressive lesions. Laminoplasty is a successful surgical procedure in the management of the properly selected patient with cervical compressive myelopathy and provides good surgical outcome for long-term follow-up [12, 13]. However, laminoplasty is not without its own potential complications. Sagittal malalignment is one of the important complications following laminoplasty that may be associated with pain and functional disability [14]. LCL after laminoplasty contributes to kyphotic alignment change, which prevents indirect decompression via posterior cervical spinal cord shift and leads to postoperative residual anterior compression of cervical spinal cord. Progressive kyphosis results in late neurological deterioration in long-term follow-up of laminoplasty. Sakai et al. [15] recently demonstrated that postoperative cervical sagittal alignment was maintained after anterior decompression and fusion but deteriorated following laminoplasty. Indeed, Suda et al. [2] demonstrated that preoperative kyphotic alignment impairs the outcome of laminoplasty for the treatment of CSM. Although we indeed performed posterior decompression with laminoplasty only for patients without preoperative kyphotic alignment, interestingly, LCL occurred after operation in 29 (70.7%) of our cases.
Although LCL following laminoplasty is likely multifactorial, several prior studies have focused more on preoperative risk factors for the development of kyphosis rather than LCL. Kim et al. [7] showed that a high T1 slope preoperatively is a risk factor for postoperative kyphosis. Kim et al. [16] demonstrated that patients with higher T1 slope had more lordotic curvature before surgery and demonstrated more LCL at 2-year follow-up. T1 slope or T1 sagittal angle is known to be useful in evaluating sagittal balance, and it was most strongly correlated with the C2-7 SVA [17]. Recently, Sakai et al. [18] showed that center of gravity of the head-C7 SVA (CGH-C7 SVA) was the preoperative risk factors for kyphotic deformity after laminoplasty for CSM in patients without preoperative cervical kyphotic alignment. In a retrospective cohort study, Michael et al. [8] reported significantly less LCL for laminoplasty beginning at C4 as opposed to C3. However, despite the existing literatures, a comprehensive study that includes these and other relevant factors (such as age, BMI, smoking history, et al.) is lacking. In contrast to these prior studies, this study using multiple regression analysis examined important factors that might be associated with LCL after laminoplasty.
In our study, higher T1 slope (B = 0.351, P = 0.037), greater C2-7 SVA (B = 0.393, P < 0.001), and starting laminoplasty at C4 level (B = − 7.038, P < 0.001) were significantly associated with higher postoperative LCL. T1 slope has constant morphological values within an individual and significantly influence the sagittal balance of the cervical spine. Kim et al. [7] reported that high T1 slope was a predictive risk factor of kyphotic deformity after laminoplasty. However, there is a recent report that the T1 slope does not affect the postoperative sagittal alignment change [19]. Thus, the effects of T1 slope on kyphotic changes during laminoplasty remain unclear. Our study reported that high T1 slope significantly correlated with LCL after laminoplasty. As the T1 slope increases, so does C2-7 lordosis to maintain forward gaze, thereby resulting in a greater degree of lordotic curvature. Laminoplasty is a posterior procedure, and posterior structures, including nuchal ligament, posterior neck muscle, and lamina, which act as preventive structures for kyphotic alignment change, are greatly damaged and atrophied after operation. As a result, patients cannot compensate high T1 slope with enough cervical lordosis due to weakness of posterior neck muscle or several cervical spinal canals compromise. Then, sagittal balance of cervical spine is uncompensated and weight of head will act as continuous kyphotic force for cervical sagittal balance, which ultimately leads to aggravated LCL. Furthermore, patients with high T1 slope and insufficient cervical lordosis come to have more horizontal or gravity direction oriented facet inclination, which can work in favor of such kyphotic force. Then, increased C2-7 SVA due to the head and neck tilting forward ultimately leads to more LCL. Our current findings also showed that C2-7 SVA had a positive association with postoperative LCL after laminoplasty and was an independent predictor of LCL.
The study also showed that CVLL correlate significantly with LCL and was also an independent predictor of LCL after laminoplasty. The previous studies have demonstrated the importance of the C2 extensor muscle attachments in postoperative cervical spine alignment [20, 21]. Iizuka et al. [20] previously used MRI to correlate the operative repair of the semispinalis muscle with maintenance of lordosis following laminoplasty. Iizuka et al. [22] subsequently also showed that preservation of the insertion of the deep extensor musculature to the C2 spinous process prevented significant LCL after laminoplasty. Anatomically, the distal portion of the C2 lamina is dorsal to, overlaps, and partially blocks the cephalad portion of the C3 lamina. Therefore, when a laminoplasty is performed at the C3 level, some degree of muscle detachment of C2 is almost always unavoidable to obtain the exposure necessary to be able to open C3 on C2. In contrast, although laminoplasty starting at C4 level requires at least some dissection of the C3 muscular attachments, it can generally be performed without disturbing the C2 extensor muscle insertions.
There are several limitations need to be considered in our study. First, clinical and neurological outcomes were not evaluated, because clinical and neurological outcomes, such as JOA score and Neck Disability Index, are influenced by the follow-up period after operation. However, the radiological assessment in our study had the characteristic of a prospective study with a 1-year follow-up. Second, the relationship between the LCL after laminoplasty and thoracolumbar or spino-pelvic parameters could not be confirmed, because whole sagittal radiograph was not performed.
Conclusions
Cervical alignment was compromised after laminoplasty in patients with CSM, and the degree of LCL was associated with preoperative T1 slope, C2-7 SVA, and CVLL.
References
Kimura I, Shingu H, Nasu Y (1995) Long-term follow-up of cervical spondylotic myelopathy treated by canal-expansive laminoplasty. J Bone Jt Surg Br 77(6):956–961
Suda K, Abumi K, Ito M et al (2003) Local kyphosis reduces surgical outcomes of expansive open-door laminoplasty for cervical spondylotic myelopathy. Spine (Phila Pa 1976) 28(12):1258–1262
Aita I, Wadano Y, Yabuki T (2000) Curvature and range of motion of the cervical spine after laminaplasty. J Bone Jt Surg Am 82(12):1743–1748
Baba H, Uchida K, Maezawa Y et al (1996) Lordotic alignment and posterior migration of the spinal cord following en bloc open-door laminoplasty for cervical myelopathy: a magnetic resonance imaging study. J Neurol 243(9):626–632
Taniyama T, Hirai T, Yoshii T et al (2014) Modified K-line in magnetic resonance imaging predicts clinical outcome in patients with nonlordotic alignment after laminoplasty for cervical spondylotic myelopathy. Spine (Phila Pa 1976) 39(21):E1261–E1268
Suk KS, Kim KT, Lee JH et al (2007) Sagittal alignment of the cervical spine after the laminoplasty. Spine (Phila Pa 1976) 32(23):E656–E660
Kim TH, Lee SY, Kim YC, Park MS, Kim SW (2013) T1 slope as a predictor of kyphotic alignment change after laminoplasty in patients with cervical myelopathy. Spine (Phila Pa 1976) 38(16):E992–E997
Michael KW, Neustein TM, Rhee JM (2016) Where should a laminoplasty start? The effect of the proximal level on post-laminoplasty loss of lordosis. Spine J 16(6):737–741
Machino M, Yukawa Y, Hida T et al (2012) Cervical alignment and range of motion after laminoplasty: radiographical data from more than 500 cases with cervical spondylotic myelopathy and a review of the literature. Spine (Phila Pa 1976) 37(20):E1243–E1250
Yukawa Y, Kato F, Ito K et al (2007) Laminoplasty and skip laminectomy for cervical compressive myelopathy: range of motion, postoperative neck pain, and surgical outcomes in a randomized prospective study. Spine (Phila Pa 1976) 32(18):1980–1985
Fujimura Y, Nishi Y (1996) Atrophy of the nuchal muscle and change in cervical curvature after expansive open-door laminoplasty. Arch Orthop Trauma Surg 115(3–4):203–205
Kawaguchi Y, Kanamori M, Ishihara H et al (2003) Minimum 10-year followup after en bloc cervical laminoplasty. Clin Orthop Relat Res 411:129–139
Ratliff JK, Cooper PR (2003) Cervical laminoplasty: a critical review. J Neurosurg 98(3 Suppl):230–238
Tang JA, Scheer JK, Smith JS et al (2012) The impact of standing regional cervical sagittal alignment on outcomes in posterior cervical fusion surgery. Neurosurgery 71(3):662–669 (discussion 669)
Sakai K, Yoshii T, Hirai T et al (2016) Impact of the surgical treatment for degenerative cervical myelopathy on the preoperative cervical sagittal balance: a review of prospective comparative cohort between anterior decompression with fusion and laminoplasty. Eur Spine J (Epub ahead of print)
Kim B, Yoon DH, Ha Y et al (2016) Relationship between T1 slope and loss of lordosis after laminoplasty in patients with cervical ossification of the posterior longitudinal ligament. Spine J 16(2):219–225
Ames CP, Blondel B, Scheer JK et al (2013) Cervical radiographical alignment: comprehensive assessment techniques and potential importance in cervical myelopathy. Spine (Phila Pa 1976) 38(22 Suppl 1):S149–S160
Sakai K, Yoshii T, Hirai T et al (2016) Cervical sagittal imbalance is a predictor of kyphotic deformity after laminoplasty in cervical spondylotic myelopathy patients without preoperative kyphotic alignment. Spine (Phila Pa 1976) 41(4):299–305
Cho JH, Ha JK, Kim DG et al (2014) Does preoperative T1 slope affect radiological and functional outcomes after cervical laminoplasty? Spine (Phila Pa 1976) 39(26):E1575–E1581
Iizuka H, Shimizu T, Tateno K et al (2001) Extensor musculature of the cervical spine after laminoplasty: morphologic evaluation by coronal view of the magnetic resonance image. Spine (Phila Pa 1976) 26(20):2220–2226
Lin S, Zhou F, Sun Y et al (2015) The severity of operative invasion to the posterior muscular-ligament complex influences cervical sagittal balance after open-door laminoplasty. Eur Spine J 24(1):127–135
Iizuka H, Nakajima T, Iizuka Y et al (2007) Cervical malalignment after laminoplasty: relationship to deep extensor musculature of the cervical spine and neurological outcome. J Neurosurg Spine 7(6):610–614
Acknowledgements
We thank Dr. Jie Li for his assistance in the statistical analysis.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
The author(s) declare that they have no competing interests.
Rights and permissions
About this article

Cite this article
Zhang, J.T., Li, J.Q., Niu, R.J. et al. Predictors of cervical lordosis loss after laminoplasty in patients with cervical spondylotic myelopathy. Eur Spine J 26, 1205–1210 (2017). https://doi.org/10.1007/s00586-017-4971-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-017-4971-4